
Abstract
Occupational therapy sessions conducted through videoconferencing were found to be effective and acceptable to patients.
Advances in the detection and treatment of breast cancer over the past 3 decades have resulted in a 5-yr overall survival rate of >90% among newly diagnosed patients and the estimated 3.1 million breast cancer survivors in the United States (Siegel et al., 2016). Because more women are living longer after diagnosis and treatment of breast cancer, minimizing treatment-related morbidities has a profound effect on their day-to-day function and quality of life (QOL; Beaulac et al., 2002; Binkley et al., 2012).
Systemic chemotherapy given to patients when the cancer has metastasized or is at high risk for metastasis causes fatigue, nausea, diarrhea, and hair loss (Kayl & Meyers, 2006). These side effects disrupt patients’ ability to maintain normal lives. For women diagnosed with hormone receptor–positive breast cancers, prescribed hormone-blocking therapies have side effects that include hot flashes, sleep disruption, sexual disfunction, and joint pain. Joint pain disrupts functional performance, whereas sexual dysfunction may affect QOL (Marsden et al., 2019; Roberts et al., 2017).
Breast cancer treatment may require radiation to the breast, chest wall, and regional nodal stations to decrease the likelihood of recurrence. The local side effects of radiation, such as burning of the skin (like a severe sunburn) and fibrosis of the underlying tissues, are aggravated by the systemic side effects, such as severe fatigue and malaise (Pérez et al., 2017). Together, fibrosis and fatigue lead to decreased shoulder use and mobility.
Finally, operations to treat breast cancer include lumpectomies or mastectomies, with or without immediate or delayed breast reconstruction. Patients also undergo sentinel lymph node dissection (SLND; a sampling of the lymph nodes) or axillary lymph node dissection (ALND; removal of most of the lymph nodes in the nodal basin) for staging. Each of these operations can affect patient function (Angarita et al., 2018). Postoperative complications include lymphedema, pain syndromes, and axillary web syndrome (Dunne & Keenan, 2016; Zou et al., 2018). Lymphedema, perhaps the most disabling complication, affects up to 20% of women who undergo ALND and 5% of women who undergo SLND (DiSipio et al., 2013; Zou et al., 2018). Limitations in range of motion, diminished strength, and increased risk of infection result in activity restrictions (Voogd et al., 2003), translating to reduced QOL (Beaulac et al., 2002). Other surgical sequelae include postmastectomy pain syndrome and axillary web syndrome, which interfere with the ability to engage in activities of daily living (ADLs) and instrumental activities of daily living (IADLs; Dunne & Keenan, 2016; Yeung et al., 2015).
The Breast Peri-Operative Rehabilitation Program was developed more than 20 yr ago at the of City of Hope National Medical Center to address and limit the impact of the side effects from medical, radiation, and surgical treatments and to optimize function and return to meaningful occupation. The program incorporates a holistic approach that addresses physical and psychosocial aspects of performance. The baseline assessment, completed before surgery, evaluates the patient’s ADLs and IADLs. Special attention is paid to the ADLS and IADLs that require shoulder movements >90°, such as washing hair, donning shirts overhead, and reaching items on high shelves. The preoperative assessment also includes evaluation of areas of occupation that are most meaningful for the patient and other domains that are likely to be disrupted by surgery. These areas include client factors, performance skills, performance patterns, context and environment, and activity demands (American Occupational Therapy Association, 2014). As such, the preoperative evaluation covers cognition, distress, sexuality, anxiety, pain, and social support along with baseline arm circumferential measurements and bio-impedance (L-Dex) readings.
Patients are provided with a postoperative exercise program and education regarding how to safely resume activities. The information gathered preoperatively allows the occupational therapy practitioner to tailor therapy to the needs and goals of each patient. The program also educates patients on lymphedema and lymphedema prevention techniques. Patients are reassessed 3 wk after the operation on the items listed earlier. Treatment plans are updated on the basis of the patient’s progress. Areas of diminished function are addressed and incorporated into the treatment plan. L-Dex measurements are retaken if any sign or complaint of lymphedema is present. Compression garments are recommended to patients who show early signs of lymphedema. The postoperative plan includes stretching, scar management, energy conservation techniques, activity modification, coping strategies, skin care and infection precautions, sleep hygiene strategies, sexuality discussions, and reinforcement of education regarding lymphedema precautions. Resistive exercises are added to increase strength. The number of recommended sessions is based on expected achievement of the individualized goals.
Over a short period of time, City of Hope experienced rapid expansion across a vast geographic area. Cancer-specific community clinical practices were incorporated into the institutional network. As a result, meeting the occupational therapy needs of patients from the network clinics became an enormous challenge. Using videoconferencing technology, we tested the use of telemedicine as a platform to provide our well-established Breast Peri-Operative Rehabilitation Program to patients undergoing breast cancer surgery. We addressed the following research questions:
Would patients participate in telemedicine occupational therapy sessions?
Would telemedicine patients recover to baseline function at the same rate as patients in the in-person program?
Would patients be satisfied with the telemedicine platform?
Method
Telemedicine Model
We developed a “hub-and-spoke” model of telemedicine by connecting the hub (i.e., main medical center) with the spoke (i.e., community practice cancer center) site. The two locations are 75 miles apart. The occupational therapist is at the hub site and provides the telemedicine services via videoconferencing. At the spoke site, an assistant, trained as a rehabilitation aide at the hub site, acts as the “telepresenter” by assisting with the clinical encounter; by ensuring the functioning telecommunications setup; by helping the patient with positioning and exercises; and by assisting with the actual physical examination assessments, such as measuring arm circumference and L-Dex measurements under the supervision of the occupational therapist (Figure 1).
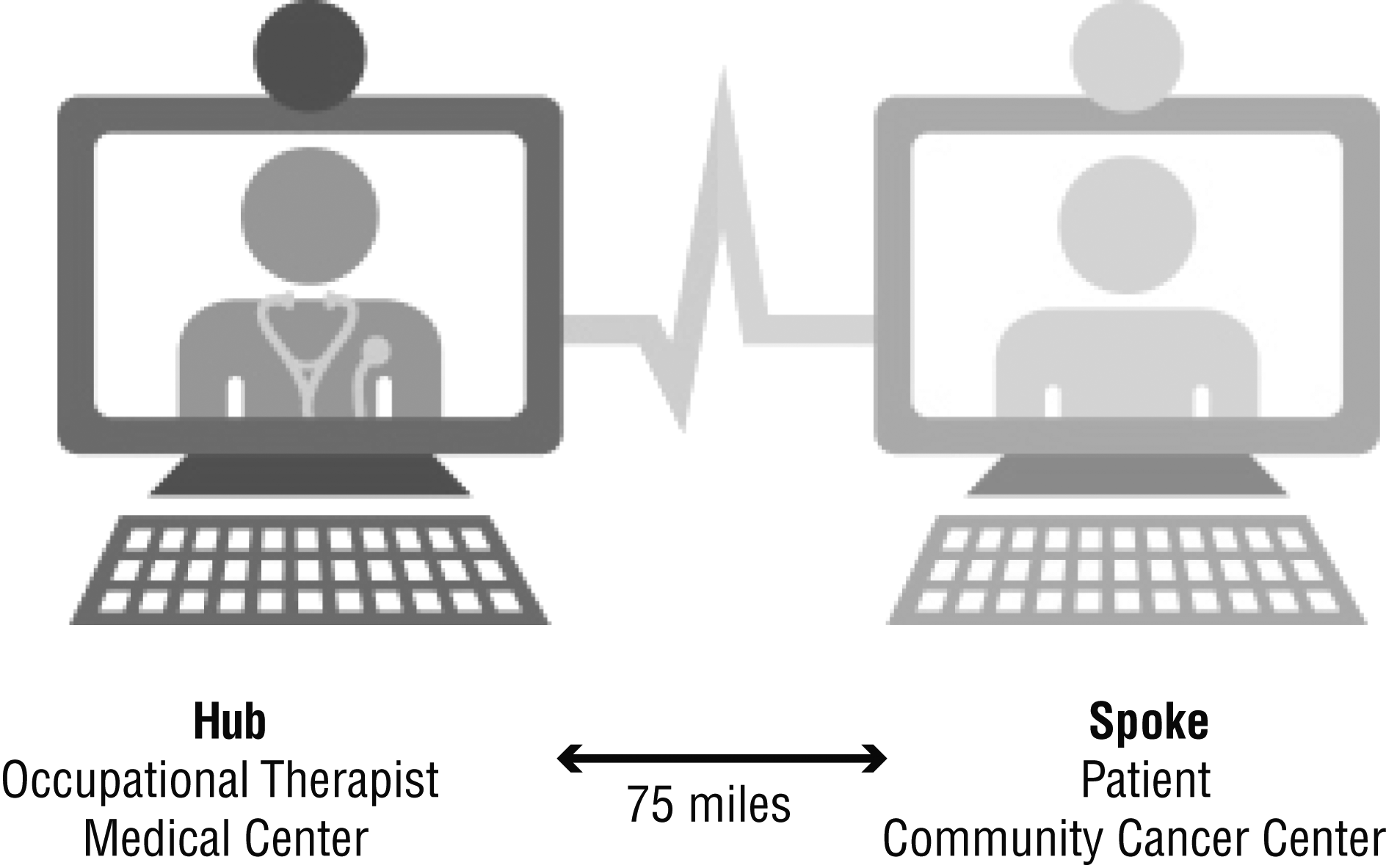
Schematic of the telemedicine breast rehabilitation program.
Preparation of Telemedicine Equipment and Infrastructure
An exam room at the spoke site was fitted with a treatment table; a high-resolution, wide-screen computer monitor; speaker system; and computer system with internet capability for videoconferencing. We used the Health Insurance Portability and Accountability Act of 1996 (HIPAA; Pub. L. 104-191)–compliant videoconferencing system approved by our institution: Zoom videoconferencing (Zoom Video Communications, San Jose, CA).
Workflow
The rehabilitation order was submitted by the physician. The patient was scheduled for the first telemedicine visit roughly a week before the operation. Consent was obtained from the patient at the initial, preoperative session. At the preoperative and postoperative sessions, the telepresenter (at the spoke site) loaded the teleconferencing program (Zoom) and contacted the hub site occupational therapist. The occupational therapist completed the evaluation and treatment of the patient as a telemedicine visit through the videoconferencing system. The telepresenter at the spoke site assisted during the session under the supervision of the occupational therapist.
Breast Peri-Operative Rehabilitation Program
Through Zoom videoconferencing, the patient is connected to the occupational therapist. Measurements, functional assessments, exercises, and education of the Breast Peri-Operative Rehabilitation Program are completed through videoconferencing technology at pre- and postoperative occupational therapy sessions, as discussed earlier.
Patient Population and Recruitment
Consecutive patients diagnosed with operable breast cancer (N = 26) who were scheduled to undergo surgical intervention at the spoke site were approached for participation in this program. Rate of participation was calculated on the basis of the number of patients who participated compared with the number of patients who were approached.
Evaluation of Telemedicine Services
Evaluation of the telemedicine rehabilitation sessions was assessed through rates of participation and completion of occupational therapy sessions, number of occupational therapy sessions and time to return to preoperative function, and patient satisfaction. Completion rate was calculated on the basis of whether patients completed all follow-up appointments as recommended by the occupational therapist. Number of occupational therapy sessions and interval time from operation to discharge from the clinic were calculated. The percentage of patients who met their treatment goals by the time of discharge from the occupational therapy sessions was calculated.
Patient Survey
Patient satisfaction was assessed through a patient-completed survey completed after the last occupational therapy session. The survey (available online at http://otjournal.net; navigate to this article, and click on “Supplemental”) consisted of 21 mixed-format questions composed of Likert scales (19 questions) and write-in answers (2 questions). The survey was developed and used at the hub site.
Statistical Analysis
Descriptive statistics were used to determine the frequencies of the population, rates of patient participation and completion of the sessions, and the results of the patient satisfaction survey.
Results
Demographic Data
During a 9-mo period, 26 consecutive patients requiring surgical management of their breast cancer were approached to participate in the Breast Peri-Operative Rehabilitation Program offered through telemedicine. Table 1 documents the demographic, clinical, and treatment characteristics of the 26 patients. Patients were female and had a mean age of 56.8 yr (range = 36–80). Of the 26 women, 14 were White, 5 were African American, 1 was Asian, and 6 identified as other. In regard to ethnicity, 6 of the women identified as Hispanic, and 20 identified as non-Hispanic. The average distance from patient’s home to the spoke site was 16 miles (range = 3–85).
Patient Demographic and Clinical Characteristics (N = 26)
Note. BRCA = breast cancer gene; CA = cancer; DCIS = ductal carcinoma in situ; ER = estrogen receptor; HER2 = human epidermal growth factor receptor 2; LND = lymph node dissection; PR = progesterone receptor.
Totals do not add to 26 because multiple histologies were identified in some specimens.
Totals do not add to 26 because multiple receptors were expressed in some of the breast cancers.
Six had bilateral mastectomies.
Totals do not add to 26 because multiple systemic therapies were given to some patients.
Of the 26 patients, 22 had a new diagnosis of breast cancer, 2 were diagnosed with recurrent ipsilateral breast cancer, and 2 were diagnosed with breast cancer gene (BRCA-1 or BRCA-2) mutations. None of the patients had metastatic disease. All patients underwent operations at the spoke site. Most of the patients were treated with mastectomy (n = 19). Six patients had bilateral mastectomies. SLNDs were completed in 50% (n = 13) of patients, whereas 7 patients had ALNDs. Most of the patients were diagnosed with hormone receptor–positive (n = 17), invasive ductal (n = 21), and node-negative (n = 16) breast cancers. Systemic treatments included neoadjuvant chemotherapy (n = 5), adjuvant chemotherapy (n = 3), and endocrine therapy (n = 8).
Patient Participation and Completion Rates
Of the 26 patients approached, 24 consented and attended the preoperative session. Of the 24, 18 attended all the recommended postoperative sessions. Of the patients who completed the recommended sessions, all regained baseline functional status and full range of motion (Table 2).The technology functioned well. The teleconferencing equipment or connection did not fail in any of the sessions.
Results of the Telemedicine Breast Rehabilitation Program (N = 26)
Patient Recovery Rates
We compared time to and rate of recovery to baseline function in the telemedicine population with a historical group at the main medical center. In the telemedicine group, the average time to complete recovery was 42.4 days after surgery (range = 26–89). The average number of telemedicine sessions attended per patient was 3.0 sessions (range = 1–5). All 18 participants (100%) met their treatment goals. In comparison, at the main medical center, where the occupational therapy sessions were conducted in person, the patients returned to baseline function in 44 days and after an average of 3.5 sessions. In addition, 75% of patients met their treatment goals (unpublished data). Overall, no difference was found between the patients treated through telemedicine and the patients treated in person on the average time to complete recovery and the number of sessions required to return patients to baseline function.
Patient Satisfaction
Patient surveys were distributed for completion after the last telemedicine session. Of the 18 patients who finished the telemedicine occupational therapy sessions, 12 patients returned completed surveys, for a response rate of 66.7%. Patient satisfaction was very high, with 100% (12 of 12) of the patients reporting being “very satisfied” with the overall services received. In addition, all patients (12 of 12) reported that they believed they received “the right amount” of information and education. As shown in Figure 2, responses to questions regarding the format and content of sessions were positive.
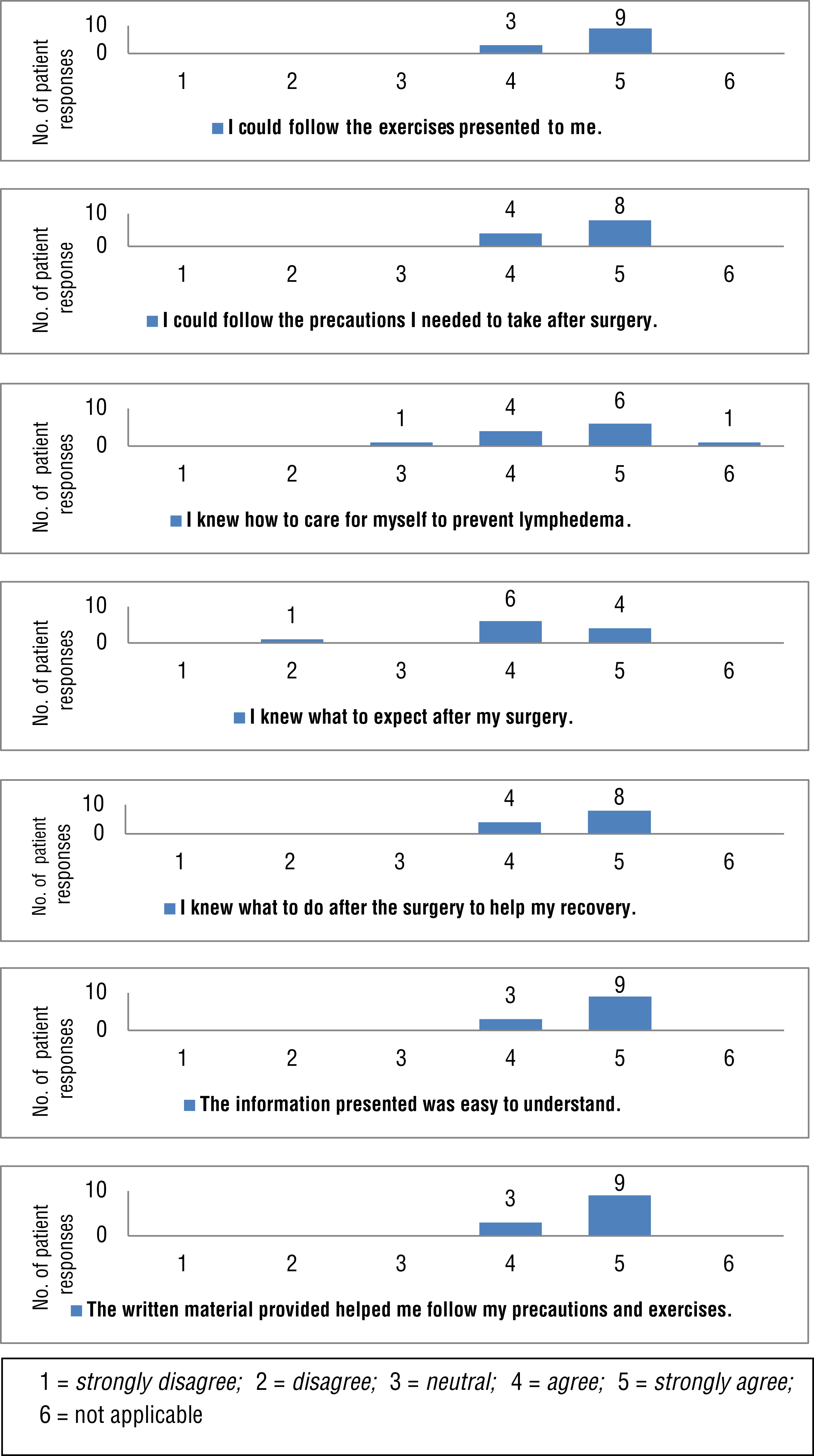
Patient survey responses.
Individual comments were enthusiastic and supportive of the telemedicine occupational therapy sessions and included the following statements: “It was a wonderful experience and helpful to have a guide to get better. It has helped a lot. Don’t change a thing”; “Loved my therapists both. You both helped to relieve my anxiety. Thank you”; and “Use of technology, what I call ‘distance learning’ was great. It also saved the exhaustion of driving through LA traffic.”
Discussion
As more women survive breast cancer, minimizing treatment-related morbidities has a profound effect on their day-to-day function and QOL (Beaulac et al., 2002; Binkley et al., 2012). For example, postoperative acute and chronic lymphedema causes pain, decreased function, and body image issues. To mitigate the symptoms, practitioners emphasize the importance of prehabilitation, defined as physical assessments that establish a baseline functional level, identify impairments, and provide targeted interventions that improve a patient’s health to reduce the incidence and severity of current and future impairments (National Lymphedema Network, 2013; Silver, 2015; Silver & Baima, 2013). Early identification, prevention, and treatment of other breast cancer therapy–related sequelae, such as neuropathy and axillary web syndrome, also lead to overall improved functional outcomes and QOL (Cheville & Tchou, 2007).
Although recognition and research supporting the importance of breast cancer–specific rehabilitation are available (Borman et al., 2017; Box et al., 2002; Dunne & Keenan, 2016; Stuiver et al., 2015), access to and care delivery issues concerning geographically remote and medically underserved communities still remain (Stubblefield, 2017). Telemedicine may provide a platform to improve access to and delivery of rehabilitation services (American Occupational Therapy Association, 2013; Galiano-Castillo et al., 2016).
Our objectives in this study were to assess (1) whether patients were willing to participate in telemedicine occupational therapy, (2) whether the time to baseline function and rate of recovery after the telemedicine sessions were comparable with that of in-person sessions, and (3) whether patients treated through the telemedicine platform were satisfied. The hub site of our telemedicine model is a National Comprehensive Cancer Center located 75 mi away from the spoke site, a community practice cancer center located in a geographically remote area. The spoke site has a population of >500,000 and spans a 2,800-square-mi area that is part of three counties (Bhaskara et al., 2008; Greater Antelope Valley Economic Alliance, 2017). One outpatient rehabilitation clinic that services the entire region is available, but it does not provide rehabilitation specific to breast cancer. In addition, patients with Medicaid insurance, such as 33% of the patients in this study, are limited to services offered by a facility located 60 mi away. As a result, most patients with breast cancer treated at the spoke site do not receive rehabilitation services.
The average distance traveled by the patient to the spoke site in this study was 16 miles one way. Of the patients who were approached, 24 of 26 participated, and 75% (18 of 24) completed all sessions. These rates suggest that patients are willing to complete rehabilitation through telemedicine.
We explored the trends for potential effectiveness of the telemedicine occupational therapy sessions by evaluating the time to return and total number of sessions required for the patients to return to baseline function. All (18 of 18) of the patients met the treatment goals within a number of sessions and time interval comparable with those of the patients treated at the hub site. These findings are consistent with results from previously published studies (Freeman et al., 2015; Galiano-Castillo et al., 2016).
We evaluated patient acceptance of telemedicine occupational therapy sessions by assessing patient satisfaction with a self-reported patient survey. The results of the survey confirmed that a high level of satisfaction was achieved with the program, the information was well presented and understandable, and the patients had the information and skills necessary to manage surgical side effects.
Limitations
The limitations of this study include the small sample size and the lack of long-term patient follow-up. The study design focused on the feasibility and acceptability of the use of telemedicine to provide rehabilitation services. Prospective studies comparing the efficacy of rehabilitation services offered via telemedicine versus in-person sessions would provide additional information on the role of telemedicine.
Implications for Occupational Therapy Practice
This study’s implications for occupational therapy practice are significant because they demonstrate the acceptability, practicality, and efficacy of our Breast Peri-Operative Rehabilitation Program offered through a telemedicine platform. This study opens the door for continued research to demonstrate the value of telemedicine occupational therapy to other patient populations, ranging from those who do not require direct hands-on therapy to those who do not have the ability to come to a traditional clinic. This study also addresses three major issues in health care today:
Patient access: The patients who lived in geographically remote communities did not have access to oncology-specific rehabilitation.
Cost: The spoke site did not have the resources to hire an oncology rehabilitation occupational therapist.
Patient satisfaction: Patient satisfaction was extremely high.
Federal and many state payers did not reimburse for occupational therapy via telemedicine before the COVID-19 pandemic. Whether reimbursement for telemedicine services continues after the current crisis remains to be determined. To support continuing reimbursement by the Centers for Medicare and Medicaid Services for telemedicine sessions, more studies are needed to demonstrate the effectiveness of telemedicine occupational therapy.
Conclusion
We conclude that telemedicine occupational therapy for patients with breast cancer receiving peri-operative treatment offers an accessible delivery platform that is acceptable to women and leads to satisfactory recovery outcomes. Our feasibility study with telemedicine occupational therapy shows that issues with access to medical care may be mitigated through the creative use of technology.
Supplemental Material
Supplementary material for Feasibility of Remote Occupational Therapy Services via Telemedicine in a Breast Cancer Recovery Program
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2021.042119.pdf for Feasibility of Remote Occupational Therapy Services via Telemedicine in a Breast Cancer Recovery Program by Lily L. Lai, Heather Player, Sherry Hite, Vikas Satyananda, Jennelle Stacey, Virginia Sun, Veronica Jones and Jennifer Hayter in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This work was funded in part by an Avon Breast Cancer Crusade Navigation Award. Portions of this article were presented at the 2017 American Occupational Therapy Association Annual Conference and Centennial Celebration, March 30–April 2, Philadelphia, PA.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.