
Abstract
Low strength of evidence was found for the use of occupational therapy interventions to improve the driving performance of older people with MCI or early-stage dementia; development of evidence and guidelines in this area is critical.
An estimated 46.8 million people worldwide live with dementia, and this number is predicted to increase to 74.7 million by 2030 (Prince et al., 2015). Dementia is a syndrome characterized by a decline in multiple areas of cognitive functioning such as memory, thinking, orientation, and judgment (World Health Organization [WHO], 2016). People with dementia experience dependence in managing daily activities (Sousa et al., 2010), the need for formal and informal care (Wimo et al., 2002), and significant health care costs (Wimo et al., 2017). Mild cognitive impairment (MCI) is also common in older people, and some people with MCI are later diagnosed with dementia (Mitchell & Shiri‐Feshki, 2009). Unlike those with dementia, people with MCI preserve their functional independence (Albert et al., 2011; Petersen et al., 1999), although research suggests that they commonly experience difficulty with instrumental activities of daily living (IADLs; Jekel et al., 2015) and cognitively demanding activities such as doing two tasks at the same time (Reppermund et al., 2011). The prevalence of dementia and MCI increases as people enter older age (Prince et al., 2013; Sachdev et al., 2015).
Driving is a complex IADL (Sherman, 2006) that involves attending to the environment and integrating relevant information to plan a response (Anstey et al., 2005). People with dementia have more difficulty following routes (Uc et al., 2004), identifying traffic signs (Uc et al., 2005), and maintaining correct lane positioning (Dawson et al., 2009) than do healthy older adults, and they drive more slowly than surrounding traffic (Eby et al., 2012). Guidelines developed through consensus by a team of international experts recommend that people who experience symptoms of dementia that has progressed to the moderate stage should be strongly discouraged from driving because of safety concerns (Rapoport et al., 2018). However, in people with MCI or early-stage dementia, the extent to which safety is affected is less clear. Some studies have found significant impairment in the driving performance of people with MCI using driving simulators (Hird et al., 2017; Pavlou et al., 2017) compared with healthy controls, whereas other studies have found that most people with MCI display minor driving difficulties that have little or no impact on safety in on-road driving and driving simulation (Anstey et al., 2017; Frittelli et al., 2009; Wadley et al., 2009).
Two recent systematic reviews of on-road driving evaluations and other driving outcomes for people with dementia found fail rates of between 11% and 13.6% in people with very mild dementia and 18% to 33.3% in people with mild dementia (Chee et al., 2017; Hird et al., 2016). These rates were higher than those of control participants (0%–2%; Chee et al., 2017; Hird et al., 2016) but nonetheless demonstrate that many people are capable of passing an on-road evaluation after a diagnosis of mild dementia. Because on-road evaluation is the main method used in practice to inform licensing status, the results of these studies suggest that although driving performance is variable, in many cases people continue to drive despite a diagnosis of MCI or early-stage dementia.
Achieving a balance between promoting driving for community participation and restricting driving because of safety concerns presents a challenge for society. Dementia is a progressive condition, people with cognitive impairment can have a reduced ability to self-regulate their driving attributable to a lack of insight (Wong et al., 2012), and family members often feel uncertain about their relative’s ability to continue driving safely (Liddle et al., 2013). However, many people wish to continue driving for as long as possible and do not plan for driving cessation (Kostyniuk & Shope, 2003), which is associated with negative outcomes such as depressive symptoms (Chihuri et al., 2016) and reduced community participation (Marottoli et al., 2000). Research findings have demonstrated that people with early-stage Alzheimer’s disease have preserved cognitive abilities, including sustained attention (Hopper et al., 2001), and are able to learn new skills (van Halteren-van Tilborg et al., 2007), which may support the learning of new driving behaviors. A rehabilitation approach to preserve safe driving performance may be beneficial for maintaining both independence and community participation.
Internationally, driving rehabilitation specialists (DRSs), many of whom are advanced practice occupational therapy practitioners, provide comprehensive driving evaluations and driving rehabilitation programs to people with medical conditions. Comprehensive driver evaluations are conducted when there is uncertainty about the extent to which a person’s functional limitations have an impact on their ability to drive. These evaluations typically include a clinical component, to assess the person’s visual–perceptual, physical, and cognitive abilities, and an on-road evaluation involving a specialized vehicle equipped with an emergency brake (Dickerson, 2013). Recommendations may include return to driving, retirement from driving, or driving rehabilitation, if there is potential for driving skills to be improved. Occupational therapists working as DRSs are trained to understand the impact of the specific medical condition on driving and to design individualized driving rehabilitation programs. DRSs commonly use remedial interventions, which involve retraining of skills to improve the driver’s basic capacities and functional abilities, or compensatory interventions, which involve the use of equipment and strategies to compensate for the impairment (Di Stefano & Macdonald, 2006).
Previous systematic reviews have examined occupational therapy interventions to improve driving performance in medically at-risk older drivers (Classen et al., 2014) and older people (Golisz, 2014; Hunt & Arbesman, 2008) and found mixed effects; however, only one of the interventions in these reviews were specifically evaluated for their effectiveness for people with MCI or early-stage dementia. The purpose of this systematic review was to describe the effectiveness of occupational therapy interventions to improve the driving performance of older people with MCI or early-stage dementia.
Method
Search Strategy
An electronic database search of MEDLINE, PsycINFO, and CINAHL (Table 1) and a gray literature search using a combination of relevant terms in Google Scholar were developed in consultation with a university librarian. The searches were conducted on May 29, 2020. The reference lists of the included studies were also searched to identify any additional relevant articles. No date restrictions were placed on the searches.
Search Strategy for MEDLINE (Adapted for Other Databases)
Inclusion Criteria
Studies were included if they met the following criteria: (1) Participants were older adults (M age ≥60 yr) with MCI, early-stage dementia, or both, and (2) an intervention was delivered that aimed to improve driving performance and that could be designed or delivered by an occupational therapy practitioner who specializes in driving. Driving performance included either real-world or simulated driving. Works not written in English were excluded. No restrictions were imposed on the type of study design.
Data Extraction and Synthesis
Two authors (Claire Spargo and Stacey George) independently screened the titles and abstracts of articles in the search results and identified studies potentially eligible for inclusion. The full-text versions of these articles were retrieved and assessed for eligibility by the same two authors independently. Disagreements between the authors were resolved through discussion and involvement of a third author when necessary. Information relating to level of evidence, study design, participants, inclusion criteria, intervention and control groups, outcome measures, and key results was extracted by Claire Spargo and checked for accuracy by Stacey George.
Quality Assessment
Claire Spargo and Stacey George independently conducted assessments of the quality of the studies using the Cochrane risk-of-bias guidelines (Higgins & Green, 2011). Disagreements were resolved via discussion and involvement of the third author when necessary.
Analysis
Levels of evidence were assigned on the basis of standards developed by Sackett and colleagues (1996); levels range from Level I (systematic review, randomized controlled trial [RCT]) to Level V (case reports and expert opinion).
The strength of the evidence was described on the basis of guidelines of the U.S. Preventive Services Task Force (2012). Strong strength of evidence indicates 2 or more Level I studies with consistent evidence from well-designed, well-conducted studies; moderate strength of evidence indicates at least 1 Level I high-quality study or multiple moderate quality studies that provide sufficient evidence to determine effectiveness but with confidence estimates constrained; and low strength of evidence indicates a small number of low-level studies with flaws in study design.
Results
Study Selection
The search of databases revealed 1,173 articles; citations were downloaded into Endnote (Clarivate Analytics, Philadelphia, PA). After removal of duplicates and title and abstract screening, we reviewed the full text of eight potentially relevant articles. Five of these articles were assessed as meeting the inclusion criteria. The other three were excluded because they did not refer to participants as having a diagnosis of MCI or early-stage dementia. No additional eligible studies were identified through gray literature or reference list searches. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram is presented in Figure 1.
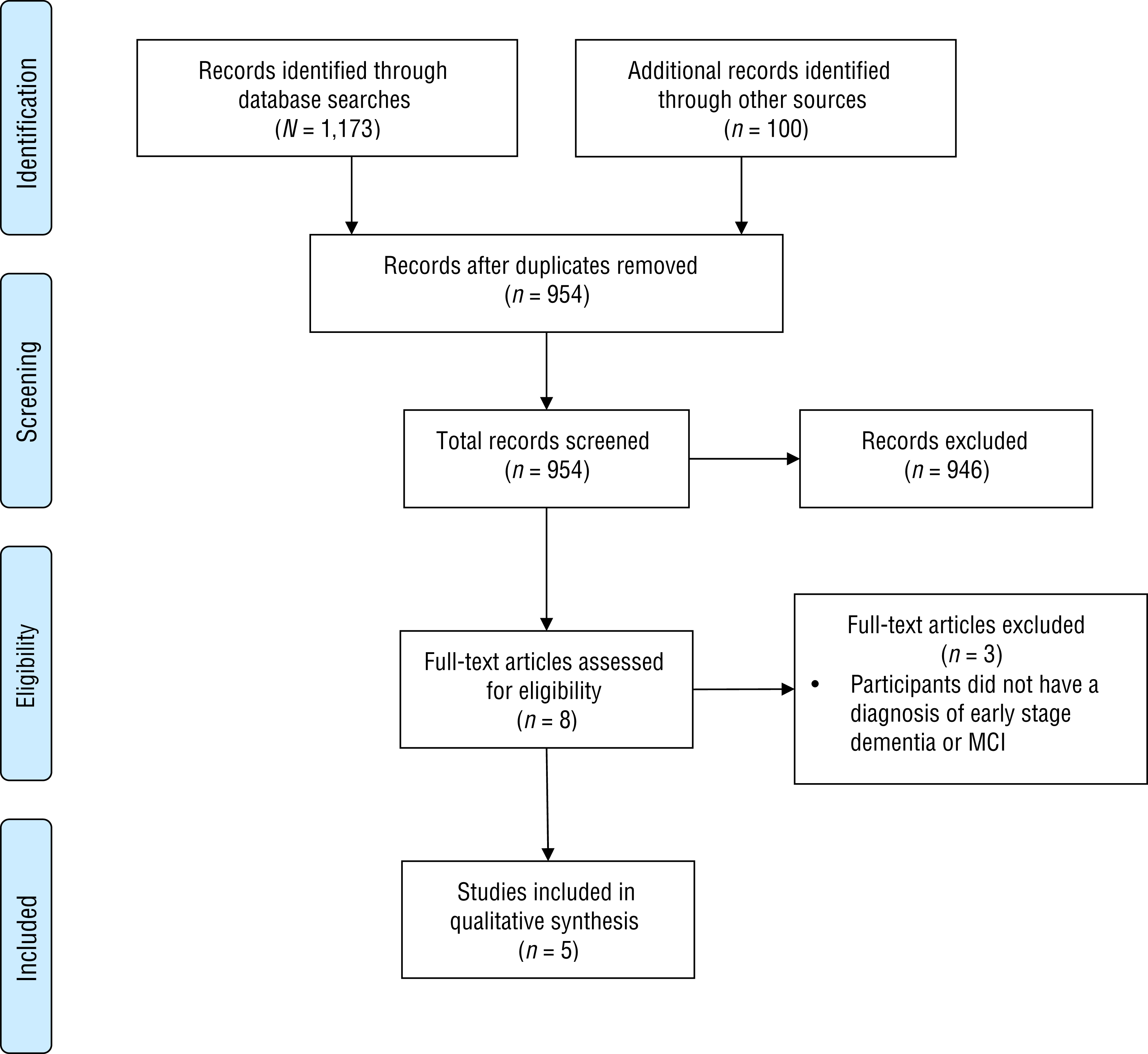
Flow diagram for the included studies in the systematic review.
Study Characteristics
Characteristics of included studies are presented in Table A.1 in the Appendix. We included 1 Level I RCT that was conducted in Japan (Shimada et al., 2019) and 4 Level III studies with quasi-experimental designs that were conducted in the United States, Canada, and Australia. Three studies included participants with MCI (Shimada et al., 2019; Teasdale, Simoneau, Hudon, Germain Robitaille, et al., 2016; Teasdale, Simoneau, Hudon, Moszkowicz, et al., 2016), 1 study included participants with very mild or mild dementia (Ott et al., 2017), and 1 study included participants with a diagnosis of either mild Alzheimer’s disease or MCI because of Alzheimer’s disease (Yi et al., 2015). The RCT involved 160 participants, whereas sample sizes in the other studies ranged from 12 to 28.
Participants allocated to the intervention group in the RCT received a remedial intervention consisting of on-road training sessions, classroom vision training, and driving simulator training sessions (Shimada et al., 2019). Three Level III studies tested remedial interventions that included driving simulator training sessions (Teasdale, Simoneau, Hudon, Germain Robitaille, et al., 2016; Teasdale, Simoneau, Hudon, Moszkowicz, et al., 2016) and the provision of tailored feedback using videotaped footage of real-life unsafe driving events (Ott et al., 2017). One study (Yi et al., 2015) used a compensatory approach involving the trialing of three different global positioning system (GPS) conditions (audio only, audio and visual, and visual only) to assist participants with following a route while using a driving simulator. One study included a single 45-min intervention session (Yi et al., 2015), whereas the other studies included multiple intervention sessions ranging from 5 sessions over 21 days (Teasdale, Simoneau, Hudon, Germain Robitaille, et al., 2016; Teasdale, Simoneau, Hudon, Moszkowicz, et al., 2016) to 20 sessions (Shimada et al., 2019) or multiple contacts (Ott et al., 2017) over 3 mo.
Risk of Bias
The results of the quality appraisal of the studies are presented in Table A.2. The RCT was generally at low risk of bias; however, it is unclear whether allocation was adequately concealed. The quality of the other studies was variable. There was significant clinical heterogeneity among studies in regard to intervention types, outcomes, and comparison interventions. Thus, it was inappropriate to pool data.
Study Outcomes
No studies reported on pass–fail rates of on-road evaluations. Outcomes examined in the included studies were categorized as real-world driving performance indicators, driving simulator performance indicators, and additional outcomes.
Real-World Driving Performance Indicators
Two studies reported on real-world driving performance indicators (Ott et al., 2017; Shimada et al., 2019). Shimada and colleagues (2019) found that compared with a single classroom education session, a combination of on-road training sessions, classroom vision training, and driving simulator training sessions resulted in significantly increased safe driving skill scores, fewer critical errors (minor to major difficulties), and fewer dangerous driving events (serious traffic violations) when assessed during an on-road evaluation with a driving instructor.
Ott and colleagues (2017) reported that the provision of feedback using videotaped footage of participants’ real-life driving performance led to fewer unsafe driving events and that these events were less dangerous than those demonstrated at baseline. Improvements were maintained during the 2-mo follow-up phase, during which video footage was recorded but no feedback was provided. Improvements were reported across 13 different driving behavior areas, including scanning at intersections, judgment, not looking far enough ahead, rolling signs, and distracted driving.
Driving Simulator Performance Indicators
Two studies tested the effect of five driving simulator training sessions on driving simulator performance. Teasdale, Simoneau, Hudon, Moszkowicz, et al. (2016) found that participants with MCI demonstrated significant improvements in speeding, use of the turn signal, verification of the blind spot, tailgating, and braking. No significant improvements were found in stopping for a red light or making an incomplete stop at an intersection. In another study led by the same author, Teasdale, Simoneau, Hudon, Germain Robitaille, et al. (2016) found a decrease in the mean number of errors that occurred across the training sessions. Over time, participants showed significant improvements in speeding, weaving, omitting to verify a blind spot, visual search at intersections with a stop sign, and vehicle control at intersections with a stop sign. Performance for tailgating, vehicle control at intersections with a traffic light, or omitting to indicate a lane change did not change over time. Effects of the intervention were not sustained at 6-mo follow-up.
Yi et al. (2015) found that participants demonstrated safer driving simulator behaviors when using audio-only GPS cues compared with visual-only cues or both audio and visual cues. Participants also demonstrated an improved ability to complete the route when using audio-only cues or audio and visual cues compared with visual-only cues.
Additional Outcomes
Shimada and colleagues (2019) found that their intervention resulted in improved on-road abilities. They also found improved dynamic vision, measured using a dynamic visual analyzer. However, they found no difference between groups in cognitive measures using the National Center for Geriatrics and Gerontology–Functional Assessment Tool to measure word memory scores, a tablet version of the Symbol Digit Substitution Test (Wechsler, 1955), and the Trail Making Test Parts A and B (Reitan, 1958). Two studies reported that some of the participants withdrew from the trials because of driving simulator sickness (Teasdale, Simoneau, Hudon, Germain Robitaille, et al., 2016; Yi et al., 2015). One study reported that more serious driving simulator errors, such as crashing into cars and pedestrians, occurred while participants were observing visual cues on their GPS displays (Yi et al., 2015). No other studies reported a significant decline in driving performance or adverse effects related to study participation.
Discussion
This review included 1 Level I study and 4 Level III studies that examined the effectiveness of occupational therapy interventions to improve driving performance in older people with MCI or early-stage dementia. Studies that tested remedial interventions reported improvement in real-world driving performance indicators, such as driving safety in an on-road evaluation (Ott et al., 2017; Shimada et al., 2019), and improvements in some, but not all, driving simulator performance indicators (Teasdale, Simoneau, Hudon, Germain Robitaille, et al., 2016; Teasdale, Simoneau, Hudon, Moszkowicz, et al., 2016); one also reported improved dynamic vision (Shimada et al., 2019). In the study using a compensatory approach, participants demonstrated improved safety when using audio-only GPS cues to complete a route using a driving simulator (Yi et al., 2015). Moreover, participants demonstrated an improved ability to complete the route successfully when using audio-only or both audio and visual GPS cues. It is unclear whether occupational therapy interventions influence pass–fail rates in on-road evaluations in this population because pass–fail rates were not measured in the included studies. Overall, low strength of evidence is available regarding the effectiveness of interventions to improve the driving performance of older people with MCI or early-stage dementia.
Several driving performance error types reported in the studies were amenable to improvement, suggesting that remediation of both habit-based errors (e.g., omitting to verify a blind spot) and more hazardous errors (e.g., impaired visual search at intersections with a stop sign) may be possible. One interesting finding from Shimada and colleagues’ (2019) RCT was that there was no improvement in dangerous errors for participants with low driving skills. People with low baseline driving performance may not be capable of improving through intervention, and for these people, driving cessation rather than retraining should be considered, particularly if the underlying cause for the impairment is progressive. Another factor in determining whether a person may benefit from intervention is working memory capacity, which Yi and colleagues (2015) found to be significantly associated with participants’ way-finding ability when using GPS. Additional factors, such as clients’ level of insight into their own driving performance difficulties, were not measured in the included studies.
Family members were involved in the intervention in 1 study (Ott et al., 2017), in which heightened caregiver safety awareness was considered an important safety outcome in itself. Findings suggest that family involvement both supported driving cessation for those who demonstrated unsafe driving behaviors and promoted safer driving for those who continued to drive. However, the involvement of family members needs careful consideration because it may result in increased burden on the family.
Interventions in the majority of the studies (Ott et al., 2017; Shimada et al., 2019; Teasdale, Simoneau, Hudon, Germain Robitaille, et al., 2016; Teasdale, Simoneau, Hudon, Moszkowicz, et al., 2016) were tailored to the characteristics of each participant’s driving performance. Individualized tailoring of intervention is likely to be important for learning given that considerable individual variation exists in driving performance, as reported by Ott and colleagues (2017) and Anstey and colleagues (2017). Interventions that involved retraining of driving skills were delivered over multiple (5 or more) sessions, which may facilitate skill learning through repetition (van Halteren-van Tilborg et al., 2007). These promising intervention characteristics should be examined in future studies.
Examination of driving interventions in the broader literature can be considered for application with people with MCI or early-stage dementia. Driving simulators, which provide repeatable driving situations (Classen & Brooks, 2014), are a potentially viable future avenue for achieving high dosages of driving skills retraining, and they have demonstrated some effectiveness in improving driving in people with traumatic brain injury. However, for the population with MCI or early-stage dementia, research is needed that evaluates whether skills learned in driving simulators transfer to the on-road environment and which components of simulator interventions are effective, including the type of simulator, the intervention program, and the professional who delivers the program (George & de la Perrelle, 2017).
One intervention approach that warrants further research with larger trials is the provision of video feedback, which may enhance participation in driving interventions by supporting people in developing self-awareness of their driving performance difficulties. With recent technological advances, compensatory approaches such as audio-only GPS cues or the use of semiautonomous vehicles to address individual driving performance difficulties in an on-road environment are also important areas for future research (Knoefel et al., 2019).
Interestingly, few of the studies reported on the involvement of interdisciplinary teamwork. It is widely recognized that clinicians with different professional backgrounds working toward common aims as part of interdisciplinary teams bring high levels of knowledge and expertise to rehabilitation settings. Interdisciplinary teamwork is particularly important for dementia care, given the complexity of the condition and the need to consider the impact of the symptoms on both the person and their caregivers (Crooks & Geldmacher, 2004). Little research has been conducted on interdisciplinary teamwork in driving rehabilitation for people with MCI or early-stage dementia.
Limitations of the studies in this systematic review include lack of a control group (Ott et al., 2017; Teasdale, Simoneau, Hudon, Germain Robitaille, et al., 2016; Yi et al., 2015), lack of randomization (Teasdale, Simoneau, Hudon, Moszkowicz, et al., 2016; Yi et al., 2015), and small sample sizes (Ott et al., 2017; Teasdale, Simoneau, Hudon, Germain Robitaille, et al., 2016; Teasdale, Simoneau, Hudon, Moszkowicz, et al., 2016; Yi et al., 2015). Two studies (Shimada et al., 2019; Teasdale, Simoneau, Hudon, Moszkowicz, et al., 2016) did not include longer term follow-up assessments after the interventions, which is a notable limitation given that testing whether the effects of an intervention, especially learning, can be maintained over time is important for determining its clinical significance for people with MCI or early-stage dementia, who commonly have memory difficulties. One study (Teasdale, Simoneau, Hudon, Germain Robitaille, et al., 2016) did not report adverse events such as driving simulator sickness, which is known to affect older adults (Keshavarz et al., 2018).
The studies included in this review used a range of outcome measures, mostly developed locally for on-road or simulator use, and the authors provided limited details on their psychometric properties. It would be beneficial for future research to develop a standardized approach to the measurement of driving outcomes in occupational therapy, which would enable consolidation of knowledge using meta-analyses to inform evidence-based practice.
This review builds on the findings of 1 systematic review (Classen et al., 2014) that reviewed the evidence related to medically at-risk older drivers and found insufficient evidence to support interventions such as retraining programs or on-board navigation and crash warning systems to improve the driving performance of people with dementia. Two other systematic reviews have examined occupational interventions relating to driving. Golisz (2014) conducted a systematic review of occupational therapy interventions to improve driving performance in older adults and found low to moderate positive effects of these interventions. Some of the interventions examined in that review were similar to those used in the current review (e.g., coaching and feedback on performance using simulator or behind-the-wheel training). Unsworth and Baker (2014), in a broader systematic review that examined driving rehabilitation occupational therapy interventions, also found limited evidence to support the effectiveness of computer-based driving simulator training and off-road skill-specific training in improving on-road fitness to drive for older people.
With the international commitment to increase dementia research (WHO, 2017), and in the context of the prevalence of dementia and MCI and forecasts of a rapidly aging population worldwide, interventions that include driving remediation and compensation techniques are of great importance. Finding a balance between public safety and continued driving when possible for people with MCI or early-stage dementia is critically important. Effectively prolonging safe driving performance in this population can have a significant effect for individuals (improved community participation, reduced loneliness), caregivers (improved well-being), and the broader society (reduced economic impact of reliance on formal services).
This review included a comprehensive search of both electronic databases and the gray literature. Articles were restricted to publication in English, which is a limitation; however, our title and abstract screening of non-English studies did not identify any that met the inclusion criteria. The main limitation of this review was that participants in most of the studies had a diagnosis of either MCI or Alzheimer’s disease, meaning that few other types of dementia (e.g., vascular dementia) were captured; thus, the effects of interventions for people with these subtypes are largely unknown. People with early-stage dementia of other types, who may experience physical or behavioral symptoms along with cognitive changes, are at greater risk of unsafe driving than people with Alzheimer’s disease (Toepper & Falkenstein, 2019) and may be less likely to benefit from intervention.
Implications for Occupational Therapy Research and Practice
The findings of this systematic review have the following implications for future research on occupational therapy interventions to improve driving performance in older people with MCI or early-stage dementia:
RCTs that have adequate power; include long-term follow-up measures; and address clinically important outcomes, such as the ability to pass or fail a driving evaluation, are needed.
Further exploration of the potential benefits of tailored, multisession interventions with caregiver involvement and interdisciplinary teamwork is needed.
Future research should identify the factors, such as level of insight into driving performance or retained working memory, that influence the ability of people with MCI or early-stage dementia to benefit from an intervention.
In the absence of conclusive high-level research evidence to support the use of occupational therapy interventions to improve the driving performance of older people with MCI or early-stage dementia, occupational therapy practitioners must rely on their clinical experience and consideration of the client’s abilities. They should also work with the client, family members, and interdisciplinary team members to carefully monitor driving fitness.
Conclusion
This review found low strength of evidence suggesting that occupational therapy interventions may improve the driving performance of older people with MCI or early-stage dementia. The clinical significance and long-term effects of the interventions are not yet known; therefore, careful monitoring of the driving performance of people with MCI or early-stage dementia is required.
Footnotes
*
Indicates articles included in the systematic review.
Acknowledgments
This systematic review was registered on PROSPERO on February 20, 2019 (CRD42019111294). This work was supported by a Dementia Australia Research Foundation PhD scholarship.
Evidence and Risk-of-Bias Tables for the Systematic Review
Risk-of Bias Table
| Citation | Selection Bias | Performance Bias: Blinding of Participants and Personnel | Detection Bias | Attrition Bias: Incomplete Outcome Data | Reporting Bias: Selective Reporting | ||
| Random Sequence Generation | Allocation Concealment | Blinding of Outcome Assessment: Self-Reported Outcomes | Blinding of Outcome Assessment: Objective Outcomes | ||||
| Ott et al. (2017) |
|
|
|
|
|
|
|
| Shimada et al. (2019) |
|
? |
|
|
|
|
|
| Teasdale, Simoneau, Hudon, Germain Robitaille, et al. (2016) |
|
|
|
|
|
|
|
| Teasdale, Simoneau, Hudon, Moszkowicz, et al. (2016) |
|
|
|
|
|
|
|
| Yi et al. (2015) |
|
|
|
|
|
|
|
Note. Categories for risk of bias: + = low risk of bias; ? = unclear risk of bias; – = high risk of bias. Risk-of-bias table format adapted from “Assessing Risk of Bias in Included Studies,” by J. P. T Higgins, D. G. Altman, and J. A. C. Sterne, in Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0, Chapter 8), by J. P. T. Higgins and S. Green (Eds.), March 2011. https://handbook-5-1.cochrane.org. Copyright © 2011 by the Cochrane Collaboration.