
Abstract
Caregivers of people with chronic conditions may benefit from problem-solving and coping skills training, dyadic self-management education, and hands-on training.
More than 40 million informal caregivers (e.g., family, partners, neighbors, friends) provide unpaid care to adults who have at least one chronic condition (AARP & National Alliance for Caregiving, 2020). Informal caregivers provide assistance in completion of activities of daily living and instrumental activities of daily living and support for health care coordination and navigation (Schulz et al., 2020). Given the high prevalence of and anticipated rise in chronic conditions, caregivers play an integral role in maintaining the health and safety of a growing population in need of unpaid care (Stone, 2015).
Yet, people in the caregiver role are at significantly higher risk of poor psychosocial outcomes than their non-caregiving peers (Schulz et al., 2020). To ameliorate poor outcomes and support caregivers in this role, health care practitioners need to systematically address the needs of this group. The provision of role-related training and strategies to manage the caregiver’s own health can in turn improve health outcomes and service utilization for the care receiver (Aksoydan et al., 2019; Rodakowski et al., 2017). However, evidence indicates that assessment of caregivers’ ability to manage the care receiver’s or their own health is limited (AARP & National Alliance for Caregiving, 2020).
Legislation such as the Recognize, Assist, Include, Support, and Engage (RAISE) Family Caregivers Act of 2017 (Pub. L. 115-119) is responding to the lack of caregiver training by prioritizing the systematic inclusion of caregivers in health care planning. To address policy priorities and equip health care practitioners with evidence-based strategies, a comprehensive examination is needed of intervention research focused on preparing caregivers to support adults with chronic conditions. In response to this need, we conducted a systematic review to evaluate evidence for the effectiveness of interventions and intervention components to support caregivers of adults with chronic conditions.
Method
The systematic review was executed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). The research question and search terms were developed through a collaborative process with the American Occupational Therapy Association (AOTA) research methodologist and staff, a medical research librarian, and an external advisory group of occupational therapy practitioners, intervention and health services researchers, and health care administrators with expertise across community and post-acute care settings. The research librarian conducted the search using MEDLINE, PsycINFO, CINAHL, OTseeker, and Cochrane Library databases, and results were reviewed by the AOTA research methodologist to verify that the database search identified articles addressing the research question “What is the evidence for the effectiveness of interventions for caregivers of people with chronic conditions within the scope of occupational therapy practice that facilitate the ability to maintain participation in the caregiver role?”
Inclusion and Exclusion Criteria
Articles were included if they were published in English between 1995 and 2019 and described a study at the following levels (Oxford Centre for Evidence-Based Medicine, 2009):
Level 1b: well-designed individual randomized controlled trial (RCT; not a pilot or feasibility study with a small sample)
Level 2b: individual prospective cohort study, low-quality RCT (e.g., <80% follow-up or low number of participants, pilot or feasibility study), ecological study, or two-group nonrandomized study
Level 3b: individual retrospective case–control study, one-group nonrandomized pretest–posttest study, or cohort study.
In addition, interventions had to be within the scope of occupational therapy practice, defined as not requiring a non–occupational therapy educational degree or licensure. Study participants had to include caregivers for a care receiver age ≥18 yr with at least one chronic condition (e.g., cardiovascular disease, Type 2 diabetes mellitus, hypertension, chronic respiratory problems, kidney disease, stroke) or characterized as a frail older adult with chronic conditions. The intervention had to take place in the community or in a post acute care setting with outcomes collected in the community after discharge. Caregiver outcomes had to be reported. Excluded studies focused on chronic conditions covered in AOTA Practice Guidelines (e.g., Alzheimer’s disease; Piersol & Jensen, 2017) or reported outcomes captured only during the health care stay. Systematic reviews were excluded because the study descriptions lacked the necessary detail on the intervention components, but their references were hand searched for relevant articles.
Study Review and Data Extraction
The AOTA research methodologist performed the initial screening and removed articles that clearly did not meet the inclusion criteria (e.g., not research). Upon receiving the initial sample from AOTA, four authors (Stephanie A. Rouch, Beth E. Fields, Hussain A. Alibrahim, and Natalie E. Leland) completed study review and data extraction (Figure 1). Initially, two authors (Rouch and Leland) reviewed studies at the title level; once they achieved 100% agreement on 10% of the sample, title review was distributed evenly among these two authors and completed independently. At the abstract and full-text level, four authors (Rouch, Fields, Alibrahim, and Leland) reached 97% agreement on inclusion, and included studies were distributed to two pairs of authors for review. At each level of the review process, the authors discussed decisions on each study and reconciled any differences. Pairs of authors conducted data extraction for the final sample (N = 48), including diagnostic population, intervention summary, mode of delivery, caregiver and care receiver demographic information, and caregiver outcomes. Consistent with our research question, we report only on caregiver outcomes.
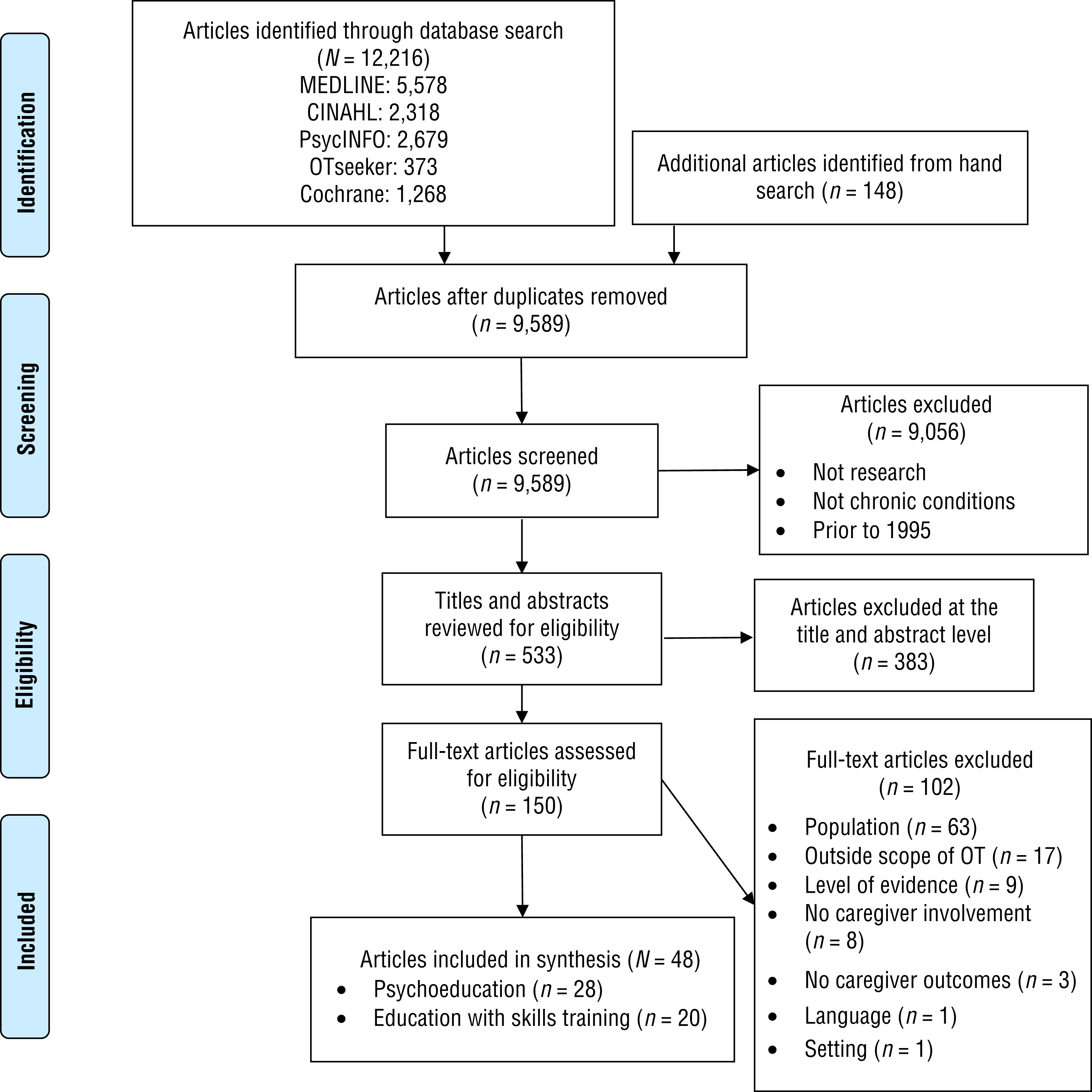
Flow of articles through the systematic review process.
Level of Evidence and Risk of Bias
Intervention studies were categorized by level of evidence according to criteria developed by the Oxford Centre for Evidence-Based Medicine (2009). An adaptation of the Cochrane risk-of-bias tool for randomized clinical trials was used to assess randomized and nonrandomized controlled studies (Higgins et al., 2011). Noncontrolled research studies were assessed using an adapted tool (National Heart, Lung, and Blood Institute, 2014).
Data Synthesis
Through an iterative process, the authors independently categorized each study into intervention themes, followed by a team discussion to achieve consensus on assignment to themes. The strength of evidence for each theme was evaluated using the U.S. Preventive Services Task Force (2018) ratings:
Strong strength of evidence: 2 or more well-designed Level 1 studies
Moderate strength of evidence: 1 or more well-designed Level 1 studies or multiple well-designed Level 2 or 3 studies with sufficient evidence to determine effects on health outcomes
Low strength of evidence: small number of low-level studies or inconsistencies across studies providing insufficient evidence to determine effects on health outcomes.
Results
The final sample included 48 articles describing studies of interventions to support and maintain the role of caregiver for an adult with one or more chronic conditions (Table A.1 in the Appendix). Of these studies, 13 provide Level 1b, 29 provide Level 2b, and 6 provide Level 3b evidence. Risk of bias was low for 35 studies and moderate for 13 studies (Tables A.2 and A.3). The interventions were categorized into one of two mutually exclusive themes: (1) psychoeducation or (2) education with skills training. Most studies reported on three or more primary outcomes; therefore, in the sections that follow, we report the three outcomes most frequently measured for each theme and provide the corresponding strength of evidence. See Table A.1 for details on additional outcomes, delivery mode, and intensity and duration of interventions.
Psychoeducation
Psychoeducation studies (n = 28) embedded cognitive–behavioral intervention components, including counseling, problem solving, coaching, and case management, to help caregivers cope. Many interventions were grounded in the stress coping or cognitive–behavioral model with the intent of empowering caregivers to manage their emotions to maintain caregiving roles.
Intervention Content
Fourteen studies focused on providing support and counseling as caregivers adjusted to their role (Ågren et al., 2012; Bakas et al., 2009; Burton & Gibbon, 2005; Clark et al., 2003; Dew et al., 2004; Goldberg et al., 1997; Hartford et al., 2002; Hartke & King, 2003; Johnston et al., 1999, 2007; Klemm et al., 2014; Lenz & Perkins, 2000; Pierce et al., 2009; Smith et al., 2012). Six studies explicitly used problem-solving strategies to address challenges related to the caregiving role (Grant, 1999; Grant et al., 2002; King et al., 2007; Perrin et al., 2010; van den Heuvel et al., 2000, 2002). Six studies provided multicomponent coaching in coping skills to manage emotions and caregiving responsibilities (Draper et al., 2007; Gräsel et al., 2005; Toseland et al., 2004; Wilz & Barskova, 2007; Wolff et al., 2009, 2010). Two studies provided counseling in caregiving strategies and case management support to facilitate access to additional resources (Dennis et al., 1997; Douglas et al., 2005).
Caregiver Outcomes
Caregiver outcomes varied across studies. The outcomes most frequently studied were depression (n = 21), burden or strain (n = 16), and quality of life (n = 10).
Depression.
Six of the 21 studies measuring depression found a significant effect. Two Level 1b studies found significant improvements for the treatment group compared with the control group at 13 wk (Grant et al., 2002) and 1 yr (Toseland et al., 2004). Three Level 2b studies found significant improvements for the treatment group compared with the control group at 5 wk (Grant, 1999), 6 mo (Wilz & Barskova, 2007), and 1 yr (Johnston et al., 1999). One Level 3b study (King et al., 2007) found significant improvements for the intervention group at 2-mo follow-up. The remaining 15 studies (5 Level 1b, 10 Level 2b) found no significant differences between groups. Inconsistent results across studies provide low strength of evidence for psychoeducation interventions to improve caregiver depression.
Burden or strain.
Three of the 16 studies measuring burden or strain found a significant effect. Positive findings were found in 3 Level 2b studies at 3 mo (Burton & Gibbon, 2005; Perrin et al., 2010) and 8 wk (Bakas et al., 2009). Alternatively, 1 Level 2b study found significantly increased burden for the treatment group compared with the control group at 6 mo (Hartke & King, 2003). The remaining 12 studies (6 Level 1b, 5 Level 2b, 1 Level 3b) found no significant between-group differences. Given the inconsistent findings, low strength of evidence is available for interventions to improve burden or strain.
Quality of life.
Two of the 10 studies measuring quality of life demonstrated a significant effect. A Level 1b study (Grant et al., 2002) and a Level 2b study (Wilz & Barskova, 2007) found significant improvements in three domains of quality of life at 3- and 6-mo follow-up, respectively. The remaining 8 studies (4 Level 1b, 4 Level 2b) found no significant improvements, indicating low strength of evidence for interventions to improve quality of life.
Education With Skills Training
Twenty articles described interventions consisting of education with skills training. These caregiver interventions were centered around providing key information about the disease process and skills training in managing the health of the care receiver to support the caregiver.
Intervention Content
Six studies provided didactic instruction focused on adapting daily living skills, managing finances, and navigating the recovery process (Björkdahl et al., 2007; Deyhoul et al., 2018; Larson et al., 2005; Louie et al., 2006; Rodgers et al., 1999; Smith et al., 2004). Six studies built on didactic education by using hands-on training and the teach-back method to increase safe patient handling skills (Hirsch et al., 2014; Kalra et al., 2004; Oupra et al., 2010; Patel et al., 2004; Shyu et al., 2010; Wang et al., 2015). Five studies focused on education in and application of self-management principles for the caregiver–care receiver dyad (Cai & Hu, 2016; Chang et al., 2015; Hu et al., 2014; Sebern & Woda, 2012; Teufel-Shone et al., 2005). Two studies facilitated a group exercise component in addition to education on disease management and recovery (Marsden et al., 2010; Molloy et al., 2006). One study trained multidisciplinary rehabilitation staff to deliver caregiver training during the care receiver’s inpatient rehabilitation stay (Forster et al., 2013).
Caregiver Outcomes
Caregiver outcomes varied across studies. The outcomes most frequently studied were quality of life (n = 11), burden or strain (n = 8), and knowledge (n = 6).
Quality of life.
Three of the 11 studies measuring quality of life found positive findings. One Level 1b study found significant improvements at 1 yr (Kalra et al., 2004), and 1 Level 2b study found an effect at 3 mo (Cai & Hu, 2016). An additional Level 2b study found significant improvements at 3 mo for the intervention group compared with the control group (Oupra et al., 2010). The remaining 8 studies (3 Level 1b, 3 Level 2b, 2 Level 3b) found no significant differences. Inconsistent results across studies provide low strength of evidence for education with skills training to improve quality of life.
Burden or strain.
Two of the 8 studies measuring burden or strain found a significant effect. A Level 1b study found significant improvements at 1 yr (Kalra et al., 2004). A Level 2b study found significant improvements at 3 mo for the intervention group compared with the control group (Oupra et al., 2010). One Level 2b study found significantly increased burden for the intervention group compared with the control group (Molloy et al., 2006). The remaining 5 studies (1 Level 1b, 4 Level 2b) found no significant differences. Inconsistent results across studies provide low strength of evidence for interventions to improve caregiver burden or strain.
Knowledge.
Of the 6 studies measuring knowledge, 5 found significant differences. Two Level 2b studies found significant differences between the intervention and control groups at 3 mo (Cai & Hu, 2016) and 6 mo (Rodgers et al., 1999), whereas 3 Level 3b studies found significant improvements for the intervention group at 2-wk (Teufel-Shone et al., 2005) and 1-mo (Hu et al., 2014; Louie et al., 2006) follow-up. The remaining Level 2b study found no significant differences (Smith et al., 2004). Based on significant results from 5 of the 6 studies, moderate strength of evidence supports education with skills training to improve knowledge.
Discussion
The rising prevalence of chronic conditions, in conjunction with federal policy prioritizing the systematic inclusion of informal caregivers in care provision, underscores the need for assessments and interventions for caregivers (RAISE Family Caregivers Act; Stone, 2015). We found low strength of evidence for caregiver psychoeducation interventions to improve psychosocial outcomes. This low strength may be attributed to the broad variability in intervention components across studies. Within psychoeducation content, we identified patterns related to significant outcomes. Problem-solving training interventions in which caregivers received education and practiced using a multistep strategy to address pressing problems provided significant positive outcomes for depression (Grant, 1999; Grant et al., 2002; King et al., 2007) and quality of life (Grant et al., 2002). High-dose group-based interventions that focused on coping strategies also demonstrated efficacy in improving depression (Toseland et al., 2004; Wilz & Barskova, 2007) and quality of life (Wilz & Barskova, 2007). These findings are consistent with past literature suggesting that problem-solving and coping skills training are promising psychosocial interventions to improve caregiver well-being (Cheng et al., 2014).
Our review found moderate strength of evidence that education with skills training can improve knowledge. Didactic instruction led to improvements in knowledge in two studies, but these results did not translate to improvements in psychosocial outcomes (Louie et al., 2006; Rodgers et al., 1999). In contrast, two lower-level studies examining family education and application of self-management principles found improvements in knowledge that did translate to improvements in psychosocial outcomes (Cai & Hu, 2016; Teufel-Shone et al., 2005). These results signify that family self-management training may be a promising approach to evaluate with more rigorous research methods.
The strength of evidence for education with skills training to improve psychosocial outcomes is low, possibly because of the variability in intervention components. Interventions that included individualized hands-on training in safe transfer and handling techniques showed the most promise for improving quality of life and burden (Kalra et al., 2004; Oupra et al., 2010). Past research has found that active education leads to improved well-being, whereas passive information provision does not improve caregiver outcomes (Corry et al., 2015).
Notably, many interventions addressed the challenge of caregiver availability to participate by engaging caregivers through telehealth. Eighteen studies in our sample were partially or fully delivered by telephone, and 4 studies were delivered or supported via web-based materials. Web-based interventions have been found to be feasible and effective for improving caregiver outcomes (Sherifali et al., 2018). Current policies support the use of these delivery models (AARP & National Alliance for Caregiving, 2020); however, reimbursement for telehealth services remains inconsistent (e.g., telehealth exemptions were granted in response to coronavirus disease 2019 [COVID-19]), and more policy pushes are needed to allow the use of telehealth interventions for caregivers (Glueckauf & Noël, 2011).
Few studies in our sample addressed outcomes related to skill competence and participation, which are pivotal caregiver assessment components that have been prioritized by recent federal policies (Fields et al., 2020). Of the 48 studies, only 3 measured social participation and function (Dennis et al., 1997; Forster et al., 2013; Kalra et al., 2004), 3 measured preparedness (Grant, 1999; Grant et al., 2002; King et al., 2007), and 1 measured performance-based skill competence (Shyu et al., 2010).
Limitations
Our review included only studies published in English that were indexed in the five databases searched; thus, relevant studies may have been missed. The overall risk of bias may be higher than reported here for the Level 1b and 2b studies because most failed to discuss all relevant threats to validity. Small sample sizes and high attrition rates in the included studies reduce the generalizability of our findings. Finally, the outcome measures used and lengths of follow-up varied greatly, making it difficult to synthesize results across studies.
Implications for Occupational Therapy Practice, Research, and Education
Together, the findings of this systematic review point to the following opportunities for occupational therapy practice, research, and education:
Practitioners should embed elements of caregiver problem-solving and coping skills training, self-management education, and hands-on training into their intervention plan.
Researchers should refine and validate outcome measures that capture caregiver skill competence to accurately measure the effects of skill-based interventions. In addition, they should design care receiver–caregiver dyadic interventions that measure key caregiver outcomes (e.g., well-being, skill competence, participation in leisure and social activities).
Occupational therapy educators should integrate family-centered geriatric care into the curriculum to draw attention to both care receiver and caregiver needs, strengths, and challenges.
Conclusion
The findings of this systematic review indicate that psychoeducational interventions embedded with problem-solving and coping skills training may lessen depression and improve quality of life for caregivers of adults with chronic conditions. Training caregivers to participate in the self-management of care receivers could improve their knowledge and well-being. Caregiver education enhanced with hands-on training may improve psychosocial outcomes. Practitioners, researchers, and educators should embed problem-solving training and hands-on practice opportunities in their intervention plans, research studies, and program curricula to better support caregivers’ ability to maintain their caregiving role. High-quality, rigorous research that develops and tests dyadic interventions designed to foster caregiver engagement is warranted.
Footnotes
Acknowledgments
We thank Deborah Lieberman, Hillary Richardson, and Beth Hunter for their input and expertise in conducting the systematic review and reviewing the manuscript. This project was supported in part by the American Occupational Therapy Association. During the time of this review, Beth E. Fields received funding support through the Pittsburgh Foundation (UN2016-85266; principal investigator: A. Everette James).
*
Indicates article included in the systematic review.
Appendix
Risk-of-Bias Table for Noncontrolled Studies
| Citation | Study Question or Objective Clear | Eligibility or Selection Criteria Clearly Described | Participants Representative of Real-World Patients | All Eligible Participants Enrolled | Sample Size Appropriate for Confidence in Findings | Intervention Clearly Described and Delivered Consistently | Outcome Measures Prespecified, Defined, Valid and Reliable, and Assessed Consistently | Assessors Blinded to Participant Exposure to Intervention | Loss to Follow-up After Baseline ≤20% | Statistical Methods Examine Changes in Outcome Measures From Before to After Intervention | Outcome Measures Were Collected Multiple Times Before and After Intervention | Overall Risk of Bias Assessment |
| Chang et al. (2015) | Y | Y | N | Y | N | Y | Y | NR | N | Y | Y | M |
| Hu et al. (2014) | Y | Y | Y | Y | N | Y | Y | NR | NR | Y | Y | M |
| King et al. (2007) | Y | Y | Y | NR | NR | N | Y | NR | N | Y | Y | M |
| Louie et al. (2006) | Y | Y | Y | NR | NR | Y | N | NR | Y | Y | Y | M |
| Sebern & Woda (2012) | Y | Y | Y | Y | N | Y | Y | NR | Y | N | Y | M |
| Teufel-Shone et al. (2005) | Y | N | N | NR | N | Y | Y | NR | NR | Y | Y | M |
Note. N = no; NR = not reported; Y = yes. Adding Yes scores for each item and dividing by 11 yields an overall risk-of-bias rating: L = low overall risk (75%–100%), M = moderate overall risk (25%–75%). Risk-of-bias tool adapted from Quality Assessment Tool for Before–After (Pre–Post) Studies With No Control Group, by National Heart, Lung, and Blood Institute, n.d. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
This table is a product of AOTA’s Evidence-Based Practice Program and AOTA and is copyright © 2021 by the American Occupational Therapy Association. It may be freely reproduced for personal use in clinical or educational settings as long as the source is cited. All other uses require written permission from the American Occupational Therapy Association. To apply, visit http://www.copyright.com.
Citation: Rouch, S. A., Fields, B. E., Alibrahim, H. A., Rodakowski, J., & Leland, N. E. (2021). Evidence for the effectiveness of interventions for caregivers of people with chronic conditions: A systematic review (Table A.3). American Journal of Occupational Therapy, 75, 7504185130. https://doi.org/10.5014.ajot.2021.042838