
Abstract
The occupational goal intervention method was found to be effective in improving executive function, occupational performance, and ADLs in people with TRS.
Schizophrenia is a serious mental illness associated with poor functional status, high levels of social exclusion, and unemployment. Performance of basic activities of daily living (BADLs) is frequently impaired, as is more complex functioning, such as that involved in instrumental activities of daily living (IADLs; Foruzandeh & Parvin, 2013). The relationship between cognitive impairment and functional disability in people with schizophrenia has been demonstrated by research (Fioravanti et al., 2012; Green et al., 2000; Shamsi et al., 2011).
Executive function (EF) is an important cognitive domain affected by schizophrenia. EF is a construct involving complex, high-order, or high-level abilities, such as goal setting, planning, and problem solving. EFs include processes, capacities, or functions that draw on, manage, or supervise low-level, primary, or basic elements of cognition or metacognition (Cramm et al., 2015). Impairment in EFs in people with schizophrenia compromises their ability to perform BADLs and IADLs independently and contributes to the burden on their caregivers (Chiu et al., 2015).
Antipsychotic medications are effective in treating most symptoms of schizophrenia, but they have limited efficacy for negative symptoms and cognitive deficits. In contrast, psychosocial interventions, especially those aimed at improving EFs, are considered essential for recovery (Kluwe-Schiavon et al., 2013).
The goal of cognitive rehabilitation is to improve performance in cognitive domains and help compensate for EF deficits. Several cognitive rehabilitation programs have been developed to address EF impairment in people with schizophrenia. For example, cognitive remediation can be delivered through computerized programs that are formatted with a gamelike audiovisual interface; alternatively, it can take the form of more traditional exercises, of varying length and complexity, completed in pencil-and-paper form or performed one on one with a trained clinician (Fioravanti et al., 2012; Levaux et al., 2012; McGurk et al., 2009; Wykes et al., 2011). The transfer of gains to the real world, however, is small to medium in scope and varies across different tasks. This is because the tasks are often disconnected from the complex, day-to-day situations that people with schizophrenia encounter in real life, which involve executive processes such as problem solving, cognitive flexibility, working memory, and planning to manage goals. Other necessary skills include defining and organizing parallel subtasks, suppression of distractions, and detection and correction of errors. These are all required for daily functioning and thus necessary for behavioral adaptation in daily life.
McGurk and Mueser (2017) suggested that coupling living skills training with cognitive training yields greater gains than living skills training alone. Kurtz et al. (2015) compared social skills training combined with cognitive remediation (experimental group) with social skills training alone (control group), with the combined group demonstrating better outcomes.
The challenge for cognitive rehabilitation, and in particular for interventions to improve EF, is to improve the person’s ability to participate in meaningful activities through transfer and generalization. For example, strategies learned during a rehabilitation program, such as preparing a meal, might be applied to daily tasks in the home environment. Metacognition is the act of thinking about thinking; it includes self-awareness, self-monitoring, and self-control while an activity is being performed (Krasny-Pacini et al., 2014). Metacognitive approaches have the most evidence for improving EF.
One of the best and most extensively studied metacognitive approaches is goal management training (GMT). This technique was originally developed for neurological rehabilitation (e.g., after traumatic brain injury) and focuses on managing deficits in goal-directed behavior in daily life (Levine et al., 2000). GMT aims to address executive dysfunction by promoting a mindful approach to complex everyday activities, raising awareness of attentional lapses, and reinstating cognitive control when behavior becomes incompatible with intended goals. GMT rehabilitation includes self-instruction strategies; self-monitoring exercises; cognitive techniques aimed at improving planning, prospective memory, and cognitive control; mindfulness exercises; stories that promote discussion of executive dysfunction in daily life; and homework assignments to practice the skills learned.
Two studies have shown occupational therapy interventions based on the principles of GMT to be effective in improving EF in people with schizophrenia (Katz & Keren, 2011; Vizzotto et al., 2016). Occupational goal intervention (OGI), as adapted by Katz and Keren (2011), is a structured strategy-learning intervention that is based on GMT but developed in an occupational therapy setting. Katz and Keren (2011) demonstrated the efficacy of OGI in a small, quasi-experimental study.
OGI targets people with schizophrenia who have EF deficits that affect daily activities and participation in the community. The method focuses on helping people learn how to use strategies to perform activities and everyday tasks. The steps of the program follow GMT but have a focus at the beginning on the individual choice of meaningful activities and at the end on debriefing of activity performance (Katz & Keren, 2011).
OGI is based on Duncan et al.’s (1996) model of goal-directed behavior and the belief that people endeavor to reach goals and subgoals to perform a task. In other words, the action is represented and controlled as a hierarchy of goals and subgoals. An important aspect of effective goal-directed behavior is the selection of new actions when previously selected actions do not achieve the goal. The treatment program is directed at the EF mechanisms that are presumed to be deficient and targets the skills required for setting goals and executing them efficiently. These skills include constructing an activity plan; setting goals; making a list of what needs to be done, step by step, to achieve the goal; keeping the steps in mind and remembering them; and self-regulating and self-monitoring performance. The purpose of a goal list is to make behavior more coherent by controlling the activation or inhibition of actions that facilitates or hinders task completion.
We previously conducted a single-blind, randomized controlled pilot study to investigate the OGI method (Vizzotto et al., 2016). Twenty-five people with treatment-resistant schizophrenia (TRS) were included. Fourteen were assigned to receive OGI, and 11 were assigned to a control group (craft activities) that did not use a therapeutic intervention. Participants attended 30 sessions over the course of 15 wk. The OGI group showed a significant improvement on both the Action Program and Key Search subtests and the total score of the Behavioural Assessment of the Dysexecutive Syndrome (BADS) scale (Krabbendam et al., 1999). Family members observed improvements on a number of EF dimensions, as measured by different subtests of the Independent Living Skills Survey, Brazilian version (ILSS–BR; Bandeira et al., 2003). Although preliminary, our results indicated that the OGI method is efficacious and effective for people with TRS.
In this article, we extend the preliminary results of our pilot study and present data from a completed trial. In this randomized controlled trial, we tested the hypothesis that the OGI method effectively improves EF in people with TRS.
Method
Study Design
A single-blind, randomized controlled design was used. The OGI method was compared with a control condition (craft activities), and outcomes were measured at three time points: baseline, posttreatment, and follow-up. Participants were outpatients receiving routine treatment in the Schizophrenia Program at the Institute of Psychiatry, University of São Paulo (Programa de Esquizofrenia [PROJESQ]), School of Medicine, São Paulo, Brazil. The study was approved by the institutional review board of the University of São Paulo General Hospital. All participants gave written informed consent.
Participant Selection
People diagnosed with schizophrenia according to the Diagnostic and Statistical Manual of Mental Disorders (5th edition; American Psychiatric Association, 2013) and between ages 18 and 55 yr were considered for the study. Participants were defined as having TRS on the basis of historical criteria (i.e., failure of two adequate trials with different antipsychotic medications; Kane et al., 1988). All participants were receiving treatment with clozapine, the best antipsychotic with proven efficacy for TRS (Howes et al., 2017). Daily doses of clozapine ranged from 230 mg to 350 mg and remained stable during the intervention period. Participants were required to have a minimum of 5 yr of primary school. Potential participants were excluded on the following grounds: hospitalization in the past 3 mo, diagnosis of substance abuse or dependence, or history of traumatic brain injury or intellectual disability. Participants were treated and referred to the study by experienced psychiatrists working in the PROJESQ under the supervision of the last author (Helio Elkis).
Sixty participants were eligible for inclusion in the study; however, 6 declined. The remaining 54 were randomized using the randomly permuted blocks method to either the OGI group (n = 28) or the control group (n = 26). The investigator responsible for randomization had no contact with the participants. Over the course of the study, 6 participants dropped out: 2 from the OGI group and 4 from the control group. Therefore, the final sample consisted of 48 participants: 26 in the OGI group and 22 in the control group. Figure 1 shows the Consolidated Standards of Reporting Trials (CONSORT) diagram for the study. Participants were evaluated at baseline, posttreatment, and follow-up.
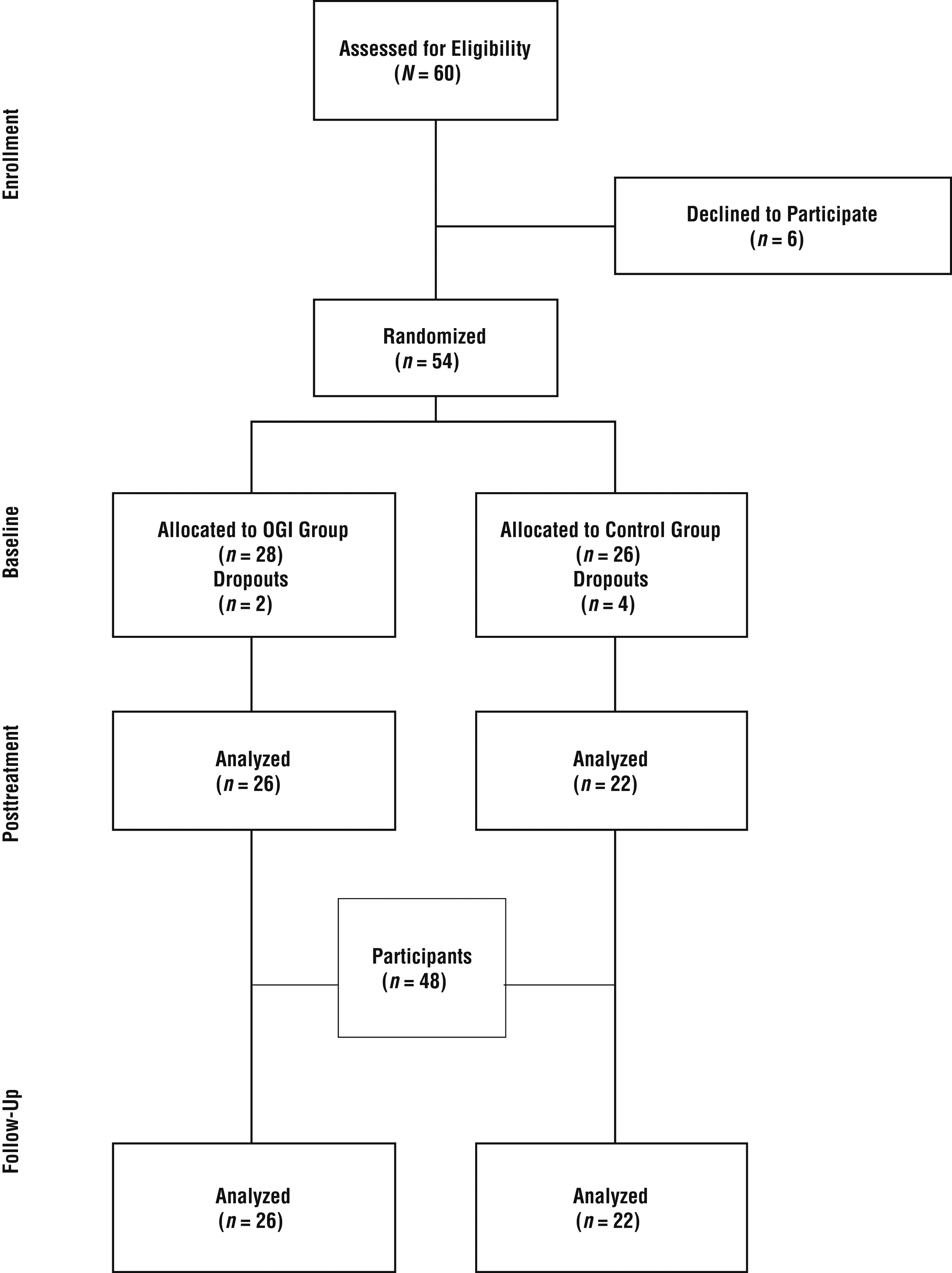
CONSORT diagram showing the flow of participants through each stage of the trial.
Procedure
Participants attended 30 sessions over a 15-wk period (2 sessions/wk). Each session lasted 90 min and involved 4 or 5 participants. In addition, participants received homework assignments, examples of which include organizing a shopping list, dealing with expenses, and preparing a simple meal. Participants were evaluated by psychologists and occupational therapists at baseline, posttreatment, and follow-up. We used the 30 items of the Positive and Negative Syndrome Scale for Schizophrenia (PANSS; Kay et al., 1987)—the gold standard in schizophrenia assessment for the appraisal of clinical stability—during the intervention rather than as an outcome measure. The Clinical Global Impression (CGI) scale (Guy, 1976), a widely used instrument whose 7 items are rated on a 7-point scale (1 = not ill, 7 = severely ill), was used to subjectively evaluate clinical improvement during the study. The experimental group sessions based on the OGI method were conducted by the first author (Adriana Vizzotto). The control group sessions were conducted by a research occupational therapist and had the same format as the experimental group sessions but included only craft activities. All participants were blinded to the assigned interventions.
Primary Outcome Measures
The BADS consists of six subtests—(1) Rule Shift Cards, (2) Action Program, (3) Key Search, (4) Temporal Judgment, (5) Zoo Map, and (6) Modified Six Elements—that measure various aspects of EF (Evans et al., 1997). The profile scores for each subtest range from 0 to 4, and the Total Profile score ranges from 0 to 24, with higher scores indicating better performance. Although one subtest (Temporal Judgment) was omitted because of cultural incompatibility, in the present study scores ranged from 0 to 20. The BADS has established reliability and validity in populations with schizophrenia (Evans et al., 1997; Katz & Keren, 2011; Krabbendam et al., 1999; Simon et al., 2003). We chose it because it has been validated in Brazil (Canali et al., 2011), as well as in several other countries, for the assessment of EFs in people with dementia and schizophrenia (Evans et al., 1997; Katz & Keren, 2011; Krabbendam et al., 1999; Simon et al., 2003). The battery was administered by a neuropsychologist who received online training from the Pearson Company, the publisher of the BADS (http://www.pearsonclinical.co.uk).
Secondary Outcome Measures
Functional Outcome
The Direct Assessment of Functional Status–Revised (DAFS–R; Loewenstein et al., 1989) was developed to objectively measure the functional capacities required for independent living. The DAFS–R was translated and culturally adapted for the Brazilian older adult population (DAFS–BR; Pereira et al., 2010) and has previously been used for evaluation of EFs in people with schizophrenia (Barrett et al., 2009; Vizzotto et al., 2016). The DAFS–BR consists of six domains with varying numbers of items. Each domain has a different score range: Time Orientation (16 points; orientation to time and ability to tell time), Communication Skills (15 points; ability to use the telephone and prepare a letter for mailing), Dealing With Finances (32 points; identify and count currency, write a check, balance a checkbook, and count change for a purchase), Shopping Skills (20 points; shopping from memory, involving verbal recall of 6 grocery items from memory, selection of the 6 items from a total of 21 items, and selection of 4 other items using a written list), Grooming Skills (13 points; ability to remove the top of a toothpaste tube, put the toothpaste onto the toothbrush, turn the water on and off, brush teeth, wash hands, and comb hair), and Eating Skills (10 points; demonstrate the motor activity involved in cutting a steak, taking a bite of the steak, eating soup, pouring water into a glass from a pitcher, and drinking water. The authors (Pereira et al., 2010) of the validation study trained the team of occupational therapists in the appropriate use of the DAFS–BR.
Autonomy
To assess participants’ autonomy, the Portuguese version of the Independent Living Skills Survey (Wallace, 1986), adapted and validated for use in Brazil—the ILSS–BR—was used. The ILSS–BR is answered by caregivers and consists of 86 items that assess the autonomy of people with chronic conditions in nine areas of BADLs and IADLs, including Self-Nourishment, Personal Hygiene, Household Activities, and Food Preparation/Storage. Scores range from 0 to 4, with lower scores indicating lesser degrees of autonomy. When we designed this study, we felt that inquiring about the families’ impressions of the participants would provide important information to help us better understand each participant’s autonomy. There are few self-reported tools for assessing autonomy. The ILSS–BR was administered by an occupational therapist with previous experience using it. Interrater reliability was not assessed because each test is performed by a single person.
Evaluation of Participant IQ
Each participant’s IQ was evaluated by a neuropsychologist using the Brazilian version of the Wechsler Abbreviated Intelligence Scale (Wechsler, 2014).
Intervention
The OGI method focuses on strategy learning using activities and everyday tasks. The steps of the program followed GMT but with a focus at the beginning on the individual choice of activities and at the end on the debriefing of activity performance. Each step relates to a specific aspect of goal-directed behavior. The steps of the OGI method are provided in Figure 2 (Katz & Keren, 2011).
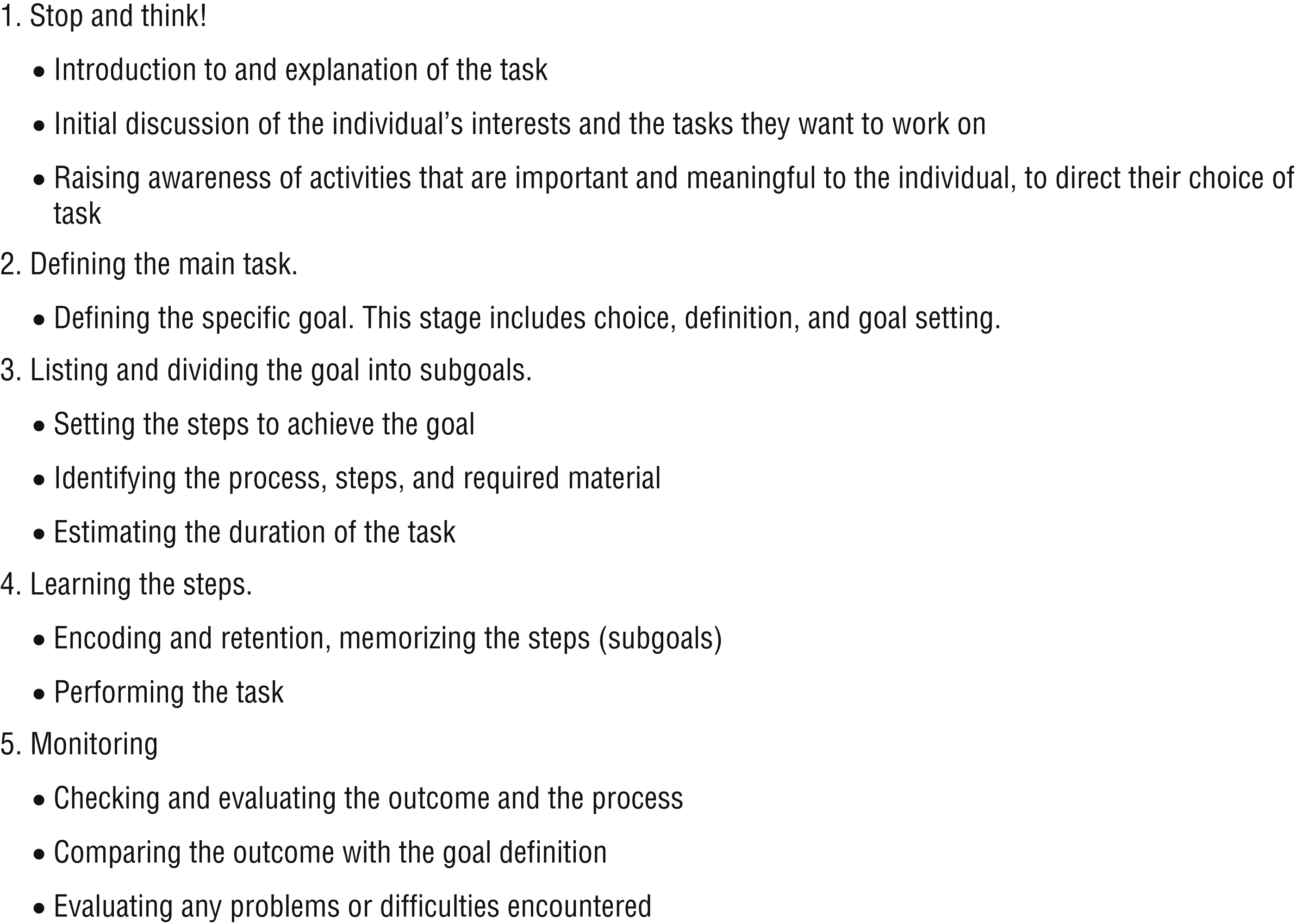
Steps of the occupational goal intervention method.
The treatment process emphasizes the use of functional activities in the three main domains originally proposed by Katz and Keren (2011): (1) Food Preparation; (2) Money Management; and (3) Reading, Writing, and Using Computers for Information Seeking. We modified Katz and Keren’s original method, adapting it to our environment; however, the functional activities in each domain were adapted to each participant’s choices and needs, according to their preferences. The OGI manual was translated into Brazilian Portuguese by members of the Occupational Therapy Service at the Institute of Psychiatry, University of São Paulo, with written permission from the authors.
For the OGI group, the initial sessions targeted BADLs (personal hygiene), followed by IADLs (housework, money management, and use of transportation), social activities, and leisure. Each participant was given four homework assignments to practice the tasks they had learned. All sessions were held in the Occupational Therapy Service of the Institute of Psychiatry, which had the necessary materials and environment to allow participants to perform real-world complex tasks such as cooking, paying bills, money management, buying goods at the supermarket, and meeting people in coffee shops or other cultural spaces, as well as undertaking other domestic tasks.
In the control group, participants engaged in craft activities such as painting or drawing on canvas and wood, but no therapeutic techniques were used. The occupational therapy professional was present at the group sessions and provided the necessary materials but did not interfere or instruct participants.
Statistical Analysis
We used χ2 or Fisher’s Exact Tests for binary values. Student’s t tests were used for means (following an underlying normal distribution; Table 1). We performed a repeated-measures analysis of variance (ANOVA) to determine whether there was a change in scores among the baseline, posttreatment, and follow-up assessment, independent of initial differences (Table 2). Treatment effects were examined at baseline, posttreatment, and follow-up, using Cohen’s d (Cohen, 1988), which was calculated as follows: the mean of the experimental group minus the mean of the control group, divided by the pooled standard deviation of both groups (Table 3). Pearson’s correlation coefficients were calculated to assess the associations between outcomes and psychopathological measures at baseline. Statistical analyses were conducted with IBM SPSS Statistics (Version 25; IBM Corp., Armonk, NY) and its Comprehensive Meta-Analysis program (Version 3) for calculation of effect sizes. The level of significance was set at p < .05.
Participants’ Demographic Data at Baseline
Note. N = 54. — = not applicable; OGI = occupational goal intervention.
χ2 test.
Fisher’s exact test.
Student’s t test.
Group Comparisons for EF, Functional Outcomes, Autonomy, Psychopathology, and Clinical Impression, With Education and IQ as Covariates
Note. Boldface text indicates significant results; italic text indicates a trend toward significance. — = not applicable; BADS = Behavioural Assessment of Dysexecutive Syndrome; CGI = Clinical Global Impression; DAFS–BR = Direct Assessment of Functional Status–Revised (Brazilian version); EF = executive function; ILSS–BR = Independent Living Skills Survey(Brazilian version); OGI = occupational goal intervention; PANSS = Positive and Negative Syndrome Scale for Schizophrenia.
Repeated-measures analysis of variance.
Effect Sizes for EF, Functional Outcomes, and Autonomy for Participants With TRS Compared With Control Participants
Note. N = 48. Numbers in boldface are significant at p < .05. — = not applicable; BADS = Behavioural Assessment of Dysexecutive Syndrome; CGI = Clinical Global Impression; CI = confidence interval; DAFS–BR = Direct Assessment of Functional Status (Brazilian version); EF = executive function; ILSS–BR = Independent Living Skills Survey (Brazilian version); OGI = occupational goal intervention; PANSS = Positive and Negative Syndrome Scale for Schizophrenia; TRS = treatment-resistant schizophrenia.
Results
Baseline Characteristics
Baseline demographic characteristics are presented in Table 1. The majority of participants were male and single, with no significant differences between the groups regarding gender, marital status, education level, employment, age at enrollment in the study, age at symptom onset, or number of hospitalizations. Although the number of years of education was slightly higher in the OGI group than in the control group, the difference was not significant (p = .064). There was also a nonsignificant difference between mean IQ values (p = .192); however, because these values can be considered low (<80) compared with the population with no mental health diagnosis, education level and IQ were included as covariates in the ANOVA.
Comparisons Between Groups at Baseline, Posttreatment, and Follow-Up
Longitudinal and Effect Size Analyses
The repeated-measures ANOVA with IQ and schooling as covariates was used to evaluate baseline, posttreatment, and follow-up measures of EFs (BADS), functional outcomes (DAFS–BR), participant autonomy (ILSS–BR), psychopathology (PANSS), and overall clinical status (CGI). As can be observed in Table 2, there were no significant differences in BADS scores between groups when IQ was included as a covariate. IQ was shown to influence most BADS subtests and some DAFS–BR subtests In the effect size analyses; a significant improvement in EF was observed in the OGI group, with medium to large effect sizes in the posttreatment and follow-up periods. This applied to the following subtests: Rule Shift Cards (posttreatment d = 0.50, follow-up d = 0.95), Action Program (posttreatment d = 0.47, follow-up d = 0.62), Key Search (posttreatment d = 0.75, follow-up d = 0.48), Zoo Map (posttreatment d = 0.42), and BADS Total score (posttreatment d = 0.73, follow-up d = 0.69; Table 3).
In regard to DAFS–BR scores, there was a significant interaction effect in Time Orientation (p < .01). In some, but not all, subtests of the DAFS–BR we noted significant differences in the scores when the covariates (IQ and education level) were included (see Table 2). According to the effect size analysis, there was a significant clinical improvement, with medium to large effect sizes at posttreatment and follow-up. This was demonstrated on the following subscales: Communication Skills (posttreatment d = 0.68, follow-up d = 0.50), Dealing With Finances (posttreatment d = 0.45), and Grooming Skills (posttreatment d = 0.53, follow-up d = 0.60), as well as in DAFS–BR Total scores (posttreatment d = 0.58).
There were, however, significant interaction effects for the ILSS–BR Total score (p = .01). On some subtests of the ILSS–BR, there were significant differences when the covariates IQ and education level were included (Table 3). The greatest effects were in the families’ and caregivers’ perceptions of participants’ autonomy and living skills in regard to ADLs. This was evidenced by large effect sizes at posttreatment and follow-up for the subtests: Self-Nourishment (posttreatment d = 0.51, follow-up d = 0.48), Personal Hygiene (posttreatment d = 0.94, follow-up d = 0.86), Household Activities (posttreatment d = 0.76, follow-up d = 0.98), Food Preparation/Storage (posttreatment d = 1.31, follow-up d = 1.37), Health Maintenance (posttreatment d = 0.50, follow-up d = 1.08), Money Management (posttreatment d = 0.97, follow-up d = 1.15), Transportation (posttreatment d = 0.58, follow-up d = 0.75), and Leisure (posttreatment d = 0.58, follow-up d = 0.89). There was also a large effect size in the Total score (posttreatment d = 1.09, follow-up d = 1.19; see Table 3).
On the PANSS, there was a significant interaction effect for the General Psychopathology subscale (p = .04). The CGI also showed an interaction effect (p < .01). The effect sizes observed in the PANSS were small, whereas the CGI showed large effect sizes (posttreatment d = −0.97, follow-up d = −0.97), suggesting that clinical stability was maintained over the course of the study (see Table 3).
Discussion
The present study provides evidence that the OGI method, compared with a placebo, is effective in the treatment of people with TRS, as demonstrated by medium to large effect size improvements on almost all subscales of the BADS. These improvements were maintained at 6-mo follow-up, during which there was no intervention.
In regard to the secondary outcomes, such as functionality, participants in the OGI group showed medium to large improvements on the DAFS–BR, which evaluates communication skills, finance management, and grooming. As with the BADS, improvements were maintained at a 6-mo follow-up without intervention. Only Time Orientation showed a significant interaction (group vs. time) at the follow-up.
The biggest impact on functional performance, however, was observed from information given by relatives, who were evaluated with the ILSS–BR. Medium to large effect sizes were found on all items of the inventory as well as the Total score, with a significant Group × Time interaction in the follow-up period. The Employment item did not, however, improve across the time points, although none of the participants were employed at baseline, making it difficult to interpret this item in isolation. Therefore, from the relatives’ perspective, the OGI intervention substantially improved performance of ADLs as compared with a placebo.
The OGI intervention was not found to have an effect on neuropsychological functions, as measured by a standard neuropsychological test. This can be observed by considering the posttreatment effect sizes.
During the study, the participants were monitored by means of PANSS and CGI scores. The results showed that the OGI method was well accepted by the participants, as demonstrated by reduced PANSS scores and clinical improvement on the CGI. There was also an interaction effect on the general symptoms assessed by the PANSS and CGI. During the course of the study, all participants remained stable, without relapses, hospitalizations, or medication changes.
This study replicates a pioneering project that used the OGI method in a smaller population of people with non–treatment-resistant schizophrenia. The OGI method was shown to produce a significant improvement in all measures of EF as well as in activities and social participation (Katz & Keren, 2011). Our aim in the present study was to evaluate the efficacy of the OGI intervention in more severely affected people (i.e., those with TRS). We demonstrated that, compared with a placebo, the OGI method is effective in improving the majority of EFs related to inhibitory control capacity, planning, problem solving, and mental flexibility. These improvements were maintained at the 6-mo follow-up. The results replicate, in part, those of a previous study of people with TRS (Buchain et al., 2003), which found significant differences between participants who received an occupational therapy intervention and control participants, in terms of occupational performance as well as interpersonal skills. The OGI method was also shown to be effective for the improvement of functional activities, and we think it is safe to assume that the thought process of learning can be transferred to any area of occupational performance (Katz & Keren, 2011).
Limitations
A meta-analysis of 247 studies of people with schizophrenia showed a mean IQ ranging from 84 to 107 (Fioravanti et al., 2012). As can be observed in Table 1, participants in the present study showed lower IQ levels than those in the Fioravanti et al. (2012) study. However, Fioravanti et al. did not discriminate people with schizophrenia from those with TRS. Because there are no studies on IQ levels in this population (Woodward & Meltzer, 2010), it is very difficult to evaluate its influence on the results of the present study.
Another limitation is that we could not evaluate premorbid IQ because there are no valid instruments in Portuguese for this purpose, as there are for English (the National Adult Reading Test; O’Carroll et al., 1992). This is important because it is well known that patients with a first episode of schizophrenia perform at 2 standard deviations below the general population (Saykin et al., 1994). To overcome such limitations, we included IQ and education level as covariates in the analyses.
It is well known that people with schizophrenia have notable cognitive impairments that are present at the onset of the disorder. In cognitive testing, people with schizophrenia perform at 2 SD below the general population (Saykin et al., 1994); therefore, it is difficult to compare our results with those of other studies that have investigated similar populations. Because of this limitation we included both IQ and education level as covariates in the analyses.
Considerations for Future Studies
A notable aspect of this work is the inclusion of participants with TRS. Treatment resistance is often mistaken for chronicity; however, schizophrenia is a chronic psychotic disorder that requires long-term treatment. At least 50% of patients, defined as treatment responders, will respond to treatment with nonclozapine antipsychotics. The majority of occupational therapy trials do not include people who are taking clozapine antipsychotics; with the exception of Buchain et al. (2003), they have included only treatment responders (Foruzandeh & Parvin, 2013; Hoshii et al., 2013; Tatsumi et al., 2012). Moreover, none of these studies used a control group with neutral activities, as we did in the present study.
Our findings have several implications for the treatment of schizophrenia. The OGI method is reliable and effective for people with TRS, but future studies should include people with non-TRS. The OGI method improved social and functional behaviors in people with TRS. Future research that compares the efficacy of the OGI method with that of other cognitive and functional interventions in patients with non-TRS is warranted.
Implications for Occupational Therapy Practice
The OGI is a reliable method that can be used by occupational therapy practitioners in the community for the improvement of EFs in people with schizophrenia, in particular those with TRS, who represent at least 30% of the patient population. The OGI is a user-friendly occupational therapy intervention that can be used as a method of cognitive rehabilitation and represents an important resource in the treatment armamentarium for people with schizophrenia receiving public mental health services in Brazil.
A recent systematic review of 106 studies conducted by Regev and Josman (2020), which aimed to capture characteristics of everyday life and EF evaluation processes for people with severe mental illness, included both Katz and Keren’s (2011) study as well as our previous project (Vizzotto et al., 2016). Of note, among the various studies with people with schizophrenia mentioned in Regev and Josman’s review, only Napal et al. (2012) included people with TRS, but it was a general cognitive rehabilitation study not specifically aimed at improving EF. On the basis of this evidence, we can affirm that, other than our previous study (Vizzotto et al., 2016) and its follow-up, the present study, no published research has used the OGI method to improve EF in people with TRS.
Despite the unequivocal evidence of the benefits of clozapine for people with TRS, it has a limited effect on improving cognition (Verma et al., 2020), which represents a major unmet treatment need for this population. Methods such as OGI constitute an important and reliable resource for people with schizophrenia, particularly those with TRS.
Conclusion
This randomized controlled trial provides evidence that, compared with control participants, people who received treatment with the OGI method demonstrated significant improvements in EF and functionality in the first phase of the study and maintained these improvements at 6-mo follow-up.
Footnotes
Acknowledgments
This study received financial support from the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), São Paulo Research Foundation (Grant 2012/01382-1), and is registered at ![]() (NCTO1879956).
(NCTO1879956).
Adriana Vizzoto selected the participants, conducted the OGI intervention, organized the database, performed statistical analysis, planned the research, and cowrote the article; Diego Celestino administered the control group activities; Patricia Buchain and Alexandra Oliveira conducted the functional evaluations; Graça Oliveria and Elaine Di Sarno conducted the neuropsychological tests; Isabel Napolitano conducted the PANSS evaluation; Helio Elkis is the principal investigator and planned the research, conducted the statistical analysis, and cowrote the article.
In 2019 and 2020, Helio Elkis received research grants from the São Paulo Research Support Foundation and honoraria for travel support or participation as an advisory board member or speaker from Aché, Janssen, Daiichi-Sankyo, and Mantecorp-Hypera. Other participants have no conflicts of interests to disclose.