
Abstract
Because sleep issues have a considerable impact on family life, occupational therapy support is important young adults with ASD and their families.
Autism spectrum disorder (ASD) significantly affects family life (Bessette Gorlin et al., 2016; Ludlow et al., 2012). Families’ occupational lives revolve around the needs of their children with ASD to ensure that those needs are met (DeGrace, 2004; Hoogsteen & Woodgate, 2013; Nicholas et al., 2016). Although the understanding of family occupation and ASD is evolving, sleep is arguably the most affected and least studied occupation (Bessette Gorlin et al., 2016; Kirkpatrick et al., 2019).
Sleep, a vital occupation across the life course (AOTA, 2020; Tester & Foss, 2018), contributes significantly to the daily function, health, and well-being of both individuals and families (Buxton et al., 2015; McCombie & Wolfe, 2017). Research indicates that up to 85% of children with ASD have difficulties with sleep compared with typically developing peers (Blackmer & Feinstein, 2016; Chen et al., 2021; Souders et al., 2017; van der Heijden et al., 2018). Although for typically developing children, sleep difficulties usually resolve with age, children with ASD often demonstrate unresolved or intensified sleep challenges into adolescence and young adulthood (Goldman et al., 2012; Hodge et al., 2014). Sleep disturbance should greatly concern occupational therapy practitioners because it is associated with poorer health-related quality of life (Deserno et al., 2019; Kuhlthau et al., 2018; Liu et al., 2020) and increased challenging behaviors among the population with ASD (Bangerter et al., 2020; Mazurek & Sohl, 2016). A call for funding by the National Center for Advancing Translational Sciences stressed the need for more research to support pediatric sleep concerns (Gruber et al., 2016).
Method
Design
In this phenomenological study, we investigated the experience of sleep for families of young adults with autism spectrum disorder (YA-ASD) through semistructured family interviews (Moustakas, 1994). Because sleep problems often persist from early childhood, we targeted families with YA-ASD to discuss and understand their experiences with sleep over time. This study received institutional review board approval.
Participants
Participants were recruited through social media postings, emails, and flyers distributed at local schools and therapy centers known to the first author (Nicole Halliwell). Interested families contacted the first author, who followed up by phone or email to discuss study-related information, determine eligibility, and obtain verbal consent. Families met inclusion criteria if they had a YA-ASD age 15 to 21 yr living at home and members of the family other than the YA-ASD were able to verbally participate in the interview process in English. The inclusion of 15- to 17-yr-olds as young adults reflects the expanding awareness of the need to begin focusing on the transition to adulthood for this population at a younger age. Families with children diagnosed with developmental disabilities other than ASD were excluded. Family composition was self-identified, and that composition was used for interviews to understand the experience of sleep as a co-constructed family occupation.
Six eligible families participated: 4 two-parent households and 2 single-parent households. Only 1 family included an adult sibling living in the home. All YA-ASD in this study were limited verbally and unable to contribute to the interview. Relevant demographic information is presented in Tables 1 and 2.
Demographic Information for Parents, Adults, and Children in the Household
Note. n/a = not applicable.
Family interview participant.
Demographic Information for Young Adults With Autism Spectrum Disorder in Household
Procedure
The first author conducted 60- to 90-min interviews of the families in their homes (Figure 1). The interviews were recorded, transcribed verbatim, and deidentified before analysis. Interviews were conducted until saturation of the data, or hearing similar core experiences across families, was achieved (Moustakas, 1994). Interviewing 6 families is consistent with previous phenomenological studies that have used family interviews (Bessette Gorlin et al., 2016; DeGrace, 2004; Suarez et al., 2014).
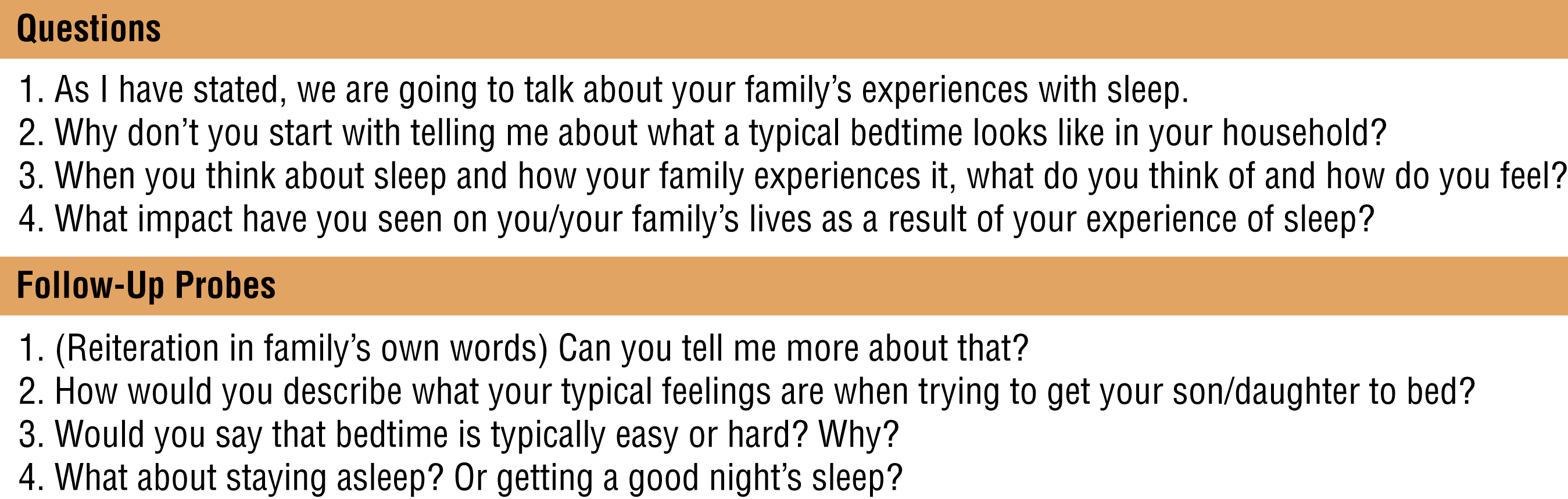
Semistructured interview questions.
Data Analysis
The research team consisted of the first author, an entry-level professional occupational therapy student (Katelyn Harris), and two occupational therapy faculty members (Julie D. Smith and Beth W. DeGrace), both with qualitative research experience focused on the ASD population. The first author was responsible for recruitment, data collection, and data management and led the data analysis process. Over 2 mo of weekly meetings, the team used four stages of data analysis: (1) epoché, (2) phenomenological reduction, (3) imaginative variation, and (4) synthesis (Moustakas, 1994).
All transcripts were reviewed and cross-checked with digital audio recordings. Each transcript was analyzed individually by at least three of the researchers, and coding results were compared across three or more researchers to triangulate. Families confirmed accuracy with verbal summaries of their responses. Audit trails and epoché diaries were maintained throughout data analyses and used as an additional source of data to achieve rigor.
Results
This study revealed five emotional themes: (1) endlessness, (2) attempts to manage, (3) difficulty, (4) persistence, and (5) the need to restructure.
Theme 1: Endlessness—“We’re Never Done”
Endlessness captures the relentless nature of ASD, which extends even into sleep. Each family reported making continuous efforts over time to facilitate sleep, leaving them taxed and overwhelmed because the “stress is 24 hours” (Family 1) and they “don’t have the luxury of saying . . . I can sleep a little longer” (Family 2). The lack of YA-ASD self-sufficiency generated feelings of hypervigilance, caused considerable stress, and denied parents rest or recuperation because they had to “[sleep] with one ear open” (Family 5).
The experience of sleep was complicated because life demands continue, regardless of inadequate sleep: “When he didn’t sleep at all . . . I still had to go to work. . . . I just had to keep going” (Family 1). This lack of physical and mental restoration made parental functions challenging or overwhelming, affecting the performance of other life occupations by both parents and the YA-ASD:
If either of us are not feeling like we got enough sleep, it really impacts the day. It makes taking care of the kids and being available to them mentally much more difficult . . . if they don’t sleep well, they’re not able to focus as well in school. (Family 2)
One family reported, “You never have your own time. It’s affecting our lives, because who [does] not want to have a life . . . [to] do something for you[rselves]?” (Family 4).
Theme 2: Attempts to Manage—“We Tried Everything”
This theme captures the experience of trying to mitigate unrelenting sleep challenges presented and faced by YA-ASD. Families tried many strategies, including calming teas, melatonin, sensory activities, diet changes, essential oils, pre-bedtime music interventions, and changes to the sleep environment (e.g., blackout curtains or sound machines). “We tried different things . . . like bath[s], relaxing things. And I think instead of work[ing], it got worse” (Family 4). Limited success and wasted resources caused frustration.
Theme 3: Difficulty—“It’s Difficult, So Difficult”
Families stressed the extreme difficulty they experienced, using terms like nightmare and absolute hell. Many YA-ASD engaged in highly disruptive nighttime activities, such as “walking around/pacing,” “clapping/making loud noises,” “watching videos,” “ransacking the kitchen,” seeking “midnight snacks,” “painting the walls,” and “kicking the door/wall.” These activities had a spillover effect on family members:
If everyone’s calm, everyone has a good night’s sleep, we kind of get a good day. If one of them had a bad sleep, then I had a bad sleep . . . that definitely has a negative impact on the next day. (Family 1)
Families expressed complex feelings of frustration, anger, and guilt from living with the sleep difficulties of their YA-ASD. Parents reported clumsiness; headaches; loss of patience; and strained marital relationships, including separation or divorce. The transcripts revealed how stressful the lack of sleep could be, with words such as trauma, wrecked, debilitating, hell, torture, and nightmare noted.
Theme 4: Persistence—“Because It’s Not Going to Change”
This theme represents the experience of hopelessness when sleep issues recurred or worsened with transitions or life changes: “Any time we have to do some change, like medication, it’s hard. We know that we have [it] again . . . the sleep problem” (Family 4). Realizing that the sleep difficulties of their YA-ASD would likely never fully resolve caused feelings of hopelessness. Families wanted improvement in sleep but also feared negative side effects from some efforts:
We never want to have the drugs change who he is. . . . We’ve always been very careful. . . . We didn’t want him to be a zombie . . . to lose his personality . . . and our choice has been to live through some of these issues. (Family 5)
Parents reported no expectation for restful sleep: “I feel like it’s a normal life for me. . . . But it’s hard to accept that I could be sleeping a full night.” (Family 3)
Theme 5: Need to Restructure—“So We Gotta Change Our Life for Him”
Families concluded that they needed to restructure and moved away from efforts to change the sleep habits of their YA-ASD, focusing instead on restructuring their lives to support it. This included sacrificing the ability to relax while using a family teamwork approach to try to balance and maintain individual health:
We had a good understanding when the other one needed a break . . . just trying to balance it out so that who’s in the worst shape needs to sleep . . . because if neither one of us were healthy, then we couldn’t deal. (Family 5)
Families described using highly structured routines, hypervigilance, and constructing their lives around the needs of the YA-ASD to preserve and maintain family life. Although restructuring caused some familial strain, families expressed feeling more positive and better overall:
If it’s raining, you’re going to complain about it raining? No. It’s not going to help, right? So you’re going to accept, “Oh, it’s raining. So what are you going to do? Get [an] umbrella.” . . . That’s life . . . we’re not sleeping, but we’re happy. So we are in the rain, we’re dancing in the rain now. (Family 4)
Restructuring family life seemed to contribute positively to the families’ experience, even though sleep remained difficult for all.
Discussion
To our knowledge, this is the first phenomenological study to examine the sleep experiences of families raising a YA-ASD. The verbatim representations of the five themes, when combined, become a powerful summary of the essence of this experience: “We’re never done. We tried everything. It’s difficult, so difficult. Because it’s not going to change. So we gotta change our life for him.”
As families navigated the occupation of sleep, they felt that their responsibility toward their YA-ASD was never ending and, despite managing over time, the impact on the families continued to be extremely difficult. Although the families felt the sleep experience could be improved, they appeared to accept the fact that sleep challenges would never fully resolve. Therefore, they relinquished their sleep preferences and patterns to meet the needs of the YA-ASD. These findings are congruent with those of studies that have examined everyday life for families raising children with autism, which identified four broad themes: (1) pervasiveness of ASD; (2) feeling overwhelmed, stressed, frustrated, and anxious; (3) structuring life around ASD; and (4) feelings of judgment, exclusion, and isolation (Bessette Gorlin et al., 2016; DeGrace, 2004; Hoogsteen & Woodgate, 2013; Kirkpatrick et al., 2019; Ludlow et al., 2012; Nicholas et al., 2016; Swinth et al., 2015). The similarity of these themes supports the established research literature describing the pervasive effect of ASD on the family and shows that ASD affects the occupation of sleep.
Despite differences in family composition and socioeconomic level, the experiences of the families in this study surrounding sleep were similar. Every YA-ASD demonstrated difficulty with the occupation of sleeping, including falling asleep, staying asleep, and engaging in various disruptive nighttime activities. To improve sleep, each family spent time and energy exploring myriad tools and strategies, seeking professional help (including from occupational therapy practitioners), and continually working to accommodate the needs of the YA-ASD. This persistent family effort often led to substantial experiences of occupational imbalance, which raises concerns for family well-being. This persistence resonates with existing family research emphasizing the toll that seeking services has on families raising a child with ASD (Hodgetts et al., 2014).
During analyses, the experience of constantly being needed, or co-occupation for sleep, elicited discussions about the similarities between parenting a YA-ASD and parenting an infant. The sleep disruption for parents of typically developing infants, although it prompts an occupational imbalance, is temporary (Creti et al., 2017). As children develop, the need for caregiving and co-occupation decreases, but this is not the experience of families raising YA-ASD (Bessette Gorlin et al., 2016; DeGrace, 2004; Hoogsteen & Woodgate, 2013; Ludlow et al., 2012; Nicholas et al., 2016; Suarez et al., 2014; Swinth et al., 2015). In contrast, this study revealed that families continue to support the sleep patterns of a YA-ASD and thus are co-occupied, limiting occupational engagement and threatening the health and well-being of all family members.
The American Academy of Neurology recently published evidence-supported practice guidelines for the treatment of sleep disturbances in children and adolescents with ASD. They recommended four approaches: (1) addressing coexisting medical conditions, (2) implementing behavioral strategies, (3) using melatonin, and (4) exploring complementary alternative medicine (Buckley et al., 2020). The results of this study indicate that these strategies and other environmental modifications that are conventionally recommended to support sleep (e.g., good sleep hygiene, melatonin) may not adequately help YA-ASD and their families.
Limitations and Future Research
Future studies might benefit from a larger sample size of YA-ASD participants, families with greater socioeconomic or ethnic diversity, YA-ASD with increased communicative participation in the interview process, or the use of a mixed-methods design to incorporate an objective sleep measure. Of note, despite vast distribution of recruitment materials across multiple platforms, all families who elected to participate were known to the first author. We believe this phenomenon is a function of the inherent intimacy surrounding the topic of sleep to families raising YA-ASD and the trust required to openly share these experiences in an in-person interview. This research demonstrates the need for further studies designed to demonstrate the effectiveness of occupational therapy providers’ interventions and strategies to support sleep for families raising children with ASD.
Implications for Occupational Therapy Practice
Research using qualitative methodology both adds value to a body of literature and informs practice by focusing on the values and opinions of the participants, being client centered while “deepening practitioners’ understanding, and by enhancing capacity for empathy and therapeutic use of self” (Tomlin & Swinth, 2015, p. 2). The lack of evidence-based interventions supporting people with ASD also reveals a considerable area of growth for research and warrants further investigation to identify helpful strategies for improving sleep for this population and then to use those strategies in research to build the evidence in support of the effective implementation of sleep interventions across disciplines. The families in this study reported an overwhelming appreciation for the time we took to understand their sleep experiences, which reinforced the notion of sleep as an overwhelming experience that often is not given adequate attention by health professionals.
This study has implications for occupational therapy practice because it
reveals the profound importance of an overlooked occupation—sleep—and its influence on the health, participation, and occupational identity of the person with ASD and their family;
indicates the significant power of the trust built between occupational therapy providers and the families they serve as an asset to better understand the impact of sleep difficulties on family life and generate potential supportive interventions; and
highlights the opportunity for occupational therapy providers to address occupational performance of sleep, specifically for families with a YA-ASD.
Conclusion
This study provides insight into the ways family life is transformed by and revolves around the needs of the YA-ASD. Our investigation unveiled the fact that challenges persist even during sleep, further confirming the pervasive influence of ASD on family life. The results suggest that families have little opportunity for restoration or reprieve and, more important, reveal a notable disconnect between the standard recommendations from health professionals to support sleep for this population and their real-world efficacy.
Footnotes
Acknowledgments
We thank the participant families, without whom this study would not have been possible, for graciously opening their homes and openly sharing their experiences. Nicole Halliwell thanks the data analysis team, her thesis committee, and her close family and friends for their unwavering and continued support throughout the research and publication process. The contents of this article were supported by a Research and Creativity Grant awarded by the University of Oklahoma Health Sciences Center Allied Health department and developed under a grant from the U.S. Department of Education (H325K120310); however, the contents do not necessarily represent the policy of the U.S. Department of Education, and readers should not assume endorsement by the U.S. government.