
Abstract
The OTTO intervention provided clinically important benefits in self-perceived functional performance to people poststroke.
After a stroke, patients often report difficulty incorporating their affected upper extremity (UE) into functional tasks and activities (Gillen & Nilsen, 2016). Ineffective functional use of the affected UE may lead to reliance on inefficient compensatory movement patterns (Mackey et al., 2006), learned nonuse (Taub et al., 1999), and the development of muscle or joint contracture (Gillen, 2016). Difficulty in initiating key muscles for tasks may account for the use of compensatory movements (Mackey et al., 2006). Specifically, patients with insufficient voluntary forearm rotation movements tend to have excessive trunk flexion, shoulder rotation, or both and require more time for task completion (Pereira et al., 2012). This suggests the importance of active forearm rotation movements in functional training for people poststroke.
Intervention for stroke is more effective if it consists of individualized, goal-directed tasks that encourage repetitive practice of task-related, specific movements (Nilsen et al., 2015). Such treatment is at the core of both the occupational therapy task-oriented (OTTO) approach (Almhdawi et al., 2016) and constraint-induced movement therapy (CIMT; Taub et al., 1999). CIMT aims to improve motor function by forced used of the affected limb (Taub et al., 1999), whereas the OTTO approach aims to maximize clients’ functional performance (Mathiowetz, 2016) through practice of tasks chosen by the clients. Compared with CIMT, the OTTO approach appears to be more compatible with clinical practice because of clients’ active engagement, less intensive clinic time, and more distributed training. Both CIMT and the OTTO approach stress actual use of the affected limb, but neither explicitly addresses the role of forearm rotation movements in the training protocol.
In an effort to reduce poststroke spasticity and prevent deformity in the hand and wrist, several orthoses are used to keep muscles and soft tissues at a functional length by immobilizing the wrist, hand, or both (Gillen, 2016). The effects of these orthoses on spasticity are questionable (Lannin & Herbert, 2003). In addition, many of these orthoses are thought to interfere with functional performance, encourage compensatory movements that interfere with therapeutic neuroplasticity (Pitts & O’Brien, 2008), and foster the learned nonuse of the affected limb (Gillen, 2016). A mobilization orthosis to assist with use of the affected UE can serve as an adjunct to poststroke functional training (Pitts & O’Brien, 2008). Given the high correlation between active forearm rotation and overall UE strength and motor function (Braendvik et al., 2010), we tested a dynamic forearm rotation orthosis as an adjunct to poststroke functional training.
The purpose of this study was to examine the efficacy of a forearm rotation orthosis and of the OTTO approach, separately and together, on functional performance of people with a hemiparetic arm.
Method
Participants
The study was approved by the institutional review boards of the University of Minnesota, University of Puget Sound, and North Memorial Health Hospital (Robbinsdale, MN). Participants were recruited in a metropolitan area (by flyers in local hospitals, at a state fair, and via a stroke association) and through former clients of a university occupational therapy student clinic. Inclusion criteria were as follows: (1) a diagnosis of stroke at least 3 mo earlier, (2) age 18 yr or older, (3) sufficient cognitive function to follow three-step verbal instruction and provide independent consent, (4) trunk and lower extremity function that did not interfere with use of the UE in functional tasks, and (5) at least 10° of shoulder flexion–abduction and elbow flexion–extension and a score of ≥3 points on the UE subscale of the short form of the Fugl-Meyer Assessment (S-FM; Hsieh et al., 2007). Those who regularly received spasticity management before the study, such as pharmacological treatment or botulism toxin injection, were asked to continue their regimen, and its effect was monitored as a potential mediating variable. Exclusion criteria were (1) severe joint deformities or contractures of the affected UE limiting range of motion (ROM) for functional tasks, (2) ability to voluntarily extend the wrist and fingers through full ROM or a score of 12 points on the UE subscale of the S-FM, (3) participation in any other rehabilitation intervention concurrent with this study, and (4) serious uncontrolled medical problems, such as seizures or visual impairment.
Study Outcomes and Measures
The study outcomes were functional performance as assessed with the Canadian Occupational Performance Measure (COPM; Law et al., 2019), the Wolf Motor Function Test (WMFT; Wolf et al., 2001), and the Motor Activity Log (MAL; Uswatte et al., 2006). The COPM was used to measure participants’ perceptions of their performance of five prioritized tasks and their satisfaction with the performance. COPM data were also used to develop patient treatment plans. The WMFT was used to measure UE motor ability with timed functional tasks. Finally, the MAL was used to measure how well (Quality of Movement scale) and how much (Amount of Use scale) participants used the affected UE. Each MAL scale was based on 30 activities of daily living or instrumental activities of daily living tasks and scored on a 6-point ordinal scale ranging from 0 to 5. All three instruments have a previous record of validity (e.g., high score reliability, discriminant validity) for use with patients poststroke (e.g., Cup et al., 2003; Morris et al., 2001; Uswatte et al., 2006).
The Nike+ FuelBand (wristband; Nike, New York), a commercial mobile device equipped with three accelerometers to detect three-dimensional movements, was used to monitor study participants’ daily arm use and their adherence to orthosis wear throughout the study. Participants receiving the orthotic intervention wore the orthosis on top of the wristband. To facilitate adherence, participants in both intervention conditions received six weekly phone calls from the investigator (Chih-Huang Yu) reminding them to wear the wristband and orthosis during functional tasks. Daily arm movement recorded by the wristband was assumed to indicate that the participant was wearing the orthosis.
Procedure
Participants’ scores on the UE subscale of the S-FM, indicating the severity of the stroke’s impact on their motor function, were used to stratify them into three groups (mild, 0–3; moderate, 4–8; or severe, 9–12). Participants in each group were then randomly assigned to one of two intervention conditions, described in the following sections. Outcomes were measured at baseline (Week 1), at the end of Phase 1 (Week 7), and at the end of Phase 2 (Week 15). The WFMT and MAL but not the COPM were administered by five blinded evaluators. It was not possible to blind participants to the intervention.
Intervention 1
Participants in the first intervention condition had 6 wk of no treatment followed by 6 wk of OTTO intervention. During the first phase, participants wore the wristband and maintained their current activity level. The investigator made six weekly reminder phone calls to facilitate adherence to the study.
Participants received the OTTO intervention in the second phase. The study followed the OTTO general guidelines for evaluation and intervention developed by Mathiowetz (2016) and Almhdawi et al. (2016). Participants received 18 hr of the OTTO intervention (three 1-hr or two 1.5-hr clinical sessions per week for 6 wk). The intensity and duration of intervention were considered consistent with current clinical practice (Almhdawi et al., 2016).
Participant occupational profiles were developed in the first week of Phase 1 using the Role Checklist (Oakley et al., 1986) to understand expected functional demand, the Interest Checklist (Brown & Stoffel, 2011) for potential intervention activities, and the COPM. Activity and occupation analyses identified potential critical control parameters in person or environment systems or subsystems that enhance or inhibit functional performance. Each session addressed the identified parameters with an emphasis on developing effective task motor behavior as well as problem-solving capabilities for everyday life. A secondary focus of treatment was directly targeting client factors or body functions if they were identified as a critical parameter limiting activities and participation.
The selection of functional tasks was derived from both the COPM and tasks identified on the Interest Checklist or mentioned during interview as being problems the participant encountered in life. An essential element of OTTO intervention is that participants were urged to apply learned strategies in a home program. Participants’ functional performance was assessed at each session to adjust the intervention, because parameters may change over time, and to enhance adherence to the home program.
Intervention 2
The second intervention condition consisted of 6 wk of orthotic intervention followed by 6 wk of orthosis plus OTTO. The forearm rotation orthosis in Phase 1 of this intervention consisted of a commercial fabric wrist orthosis (Wrist Lacer™; Medical Specialties, Inc., Charlotte, NC) and a latex-free neoprene strap. The metal bars inside the wrist orthosis were removed to allow wrist movements. A strap was attached to the orthosis to serve as the force of pull assisting either pronation or supination (depending on the identified parameter) without limiting functional elbow flexion and extension. During this period, participants were encouraged to wear the orthosis daily on top of the wristband during functional tasks. To maintain blinding of the assessors, participants were asked not to bring the orthosis to evaluation sessions. Information on possible risks of using the orthosis was included in the consent form and in the written instructions. During Phase 2 of the intervention, the orthosis protocol was combined with the OTTO intervention.
Intervention and Measurement Fidelity
Chih-Huang Yu administered the COPM and was the primary interventionist, providing orthosis fabrication, OTTO intervention, and treatment plans for all participants. The information gathered from the COPM informed the treatment plan. Virgil G. Mathiowetz, the founder of the OTTO, monitored safety and fidelity to the OTTO approach during the study.
Participants’ COPM ratings were hidden from them during evaluation but were available by request after the evaluation session. Five occupational therapy students served as blinded evaluators. Each evaluator administered all evaluations except the COPM to each participant. Evaluators demonstrated 99% interrater reliability agreement on evaluations within 8 hr of training.
Data Analysis
Analyses were performed using R software (Version 3.5.2; R Core Team, 2018). To evaluate the adequacy of the random assignment in creating balanced intervention groups, differences in the distributions of the demographic variables were compared using nonparametric methods (Fisher’s Exact Test, Mann–Whitney U test). Variables with statistically significant differences (α = .05) were included as covariates in subsequent analyses.
To account for the dependency introduced by the within-subjects design, a set of linear mixed-effects models were fitted to the data (e.g., Pinheiro & Bates, 2000). These models used dummy variables (indicating participants’ level of intervention at each time point), along with potential covariates, to evaluate the three contrasts of interest for each primary outcome, namely, (1) orthosis versus no treatment, (2) OTTO versus no treatment, and (3) OTTO versus orthosis plus OTTO. These models were estimated with a Bayesian framework using the brms package (Bürkner, 2018). The Bayesian framework is advantageous in that it uses evidence about parameter estimates and uncertainty gleaned from previous studies (“prior”) and data from the current study (“posterior”; see Dunson, 2001) to give a more informed estimate of both the model parameters and the uncertainty. The use of the hierarchical Bayesian framework also avoids problematic multiple comparisons when evaluating many contrasts using traditional (frequentist) statistical methods (Gelman et al., 2012).
Results
Recruitment at two sites was active from December 2015 to January 2018. After stratification into groups, 8 of the 18 eligible participants were randomly assigned to the first intervention, and 10 were assigned to the second (Figure 1). Four participants (2 in each intervention) dropped out before the end of Phase 1 for reasons unrelated to the study. Those who dropped out and those who completed the study did not differ significantly on any variable.
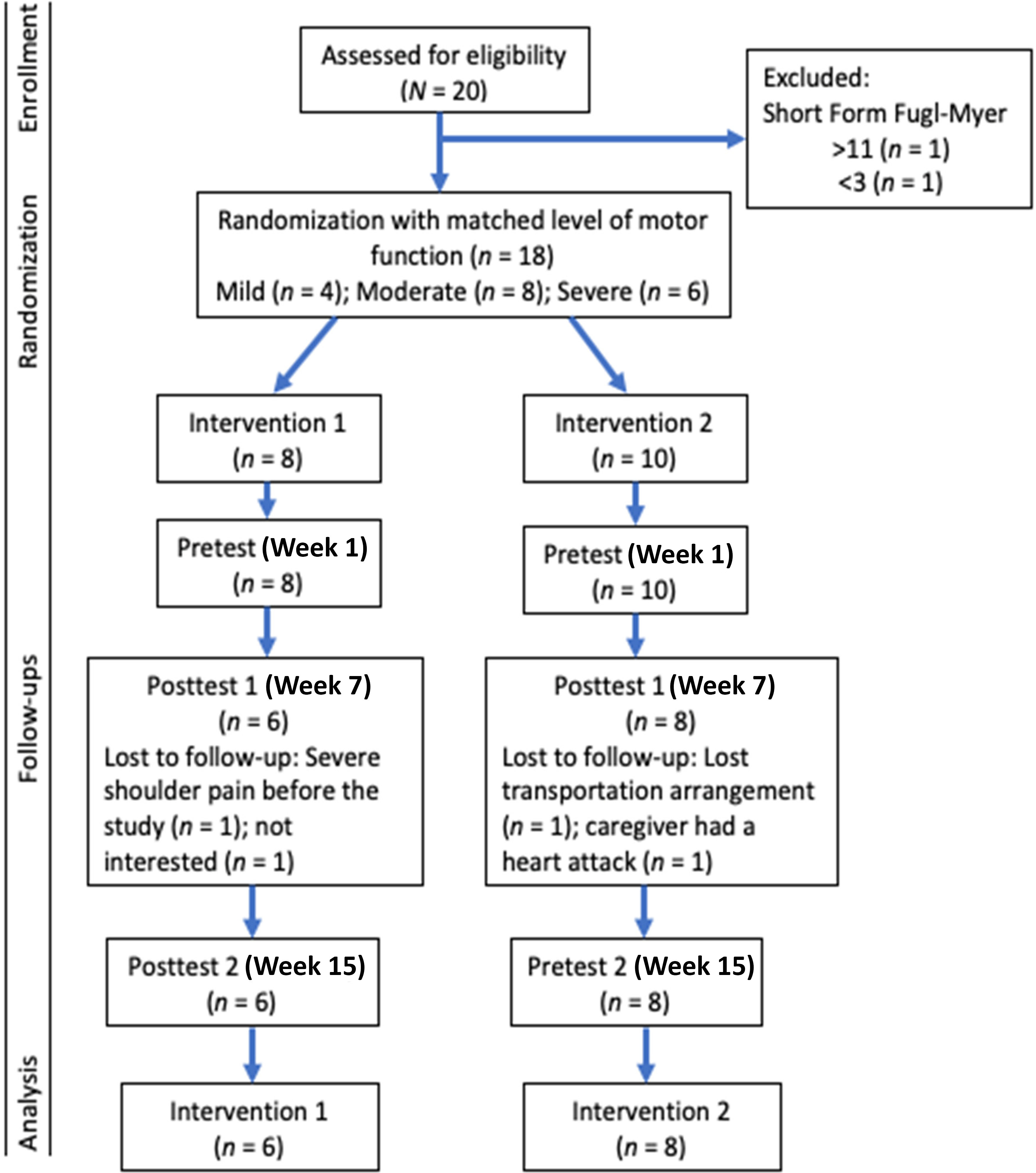
Flow of study participants throughout the study.
Table 1 summarizes the outcome and demographic variables for each of the two interventions and four outcomes. None of the demographic variables showed significant differences between groups. As such, none were included as covariates in any of the subsequent analyses, and the model fitted was as follows:
Participants by Demographics and Intervention Status and Primary Outcomes
Note. COPM = Canadian Occupational Performance Measure; MAL = Motor Activity Log; OTTO = occupational therapy task oriented; WMFT = Wolf Motor Function Test.
The choice of the exponential prior for the variance components was to ensure that these values were positive (e.g., McElreath, 2015), and prior predictive simulation suggested that this choice of priors results in relatively plausible outcomes for the effects of interest. The posterior results for the three contrasts associated with the research questions for each primary outcome are shown in Table 2. To evaluate the research questions, we established a region of practical equivalence (ROPE) based on clinical significance previously reported in the literature. For the COPM, we used a change of 2 or more (Law et al., 2019); for performance time and function on the WMFT, we used 4.36 s and 0.37 points, respectively (Lin et al., 2009); and for MAL, we used 12% of the range (van der Lee et al., 2004), or a value of 0.72. The ROPE expresses a range of parameter values equivalent to the null value for current practical purposes. We then used a decision rule, outlined in Kruschke and Liddell (2018) and adapted for the small sample size, that if most of the 95% credible interval falls outside the ROPE, then there is a clinical difference between the conditions. If most of the 95% credible interval falls inside the ROPE, then there is no clinical difference; otherwise, it remains undecided. Figure 2 shows the ROPE and credible intervals for the three contrasts for each of the primary outcomes.
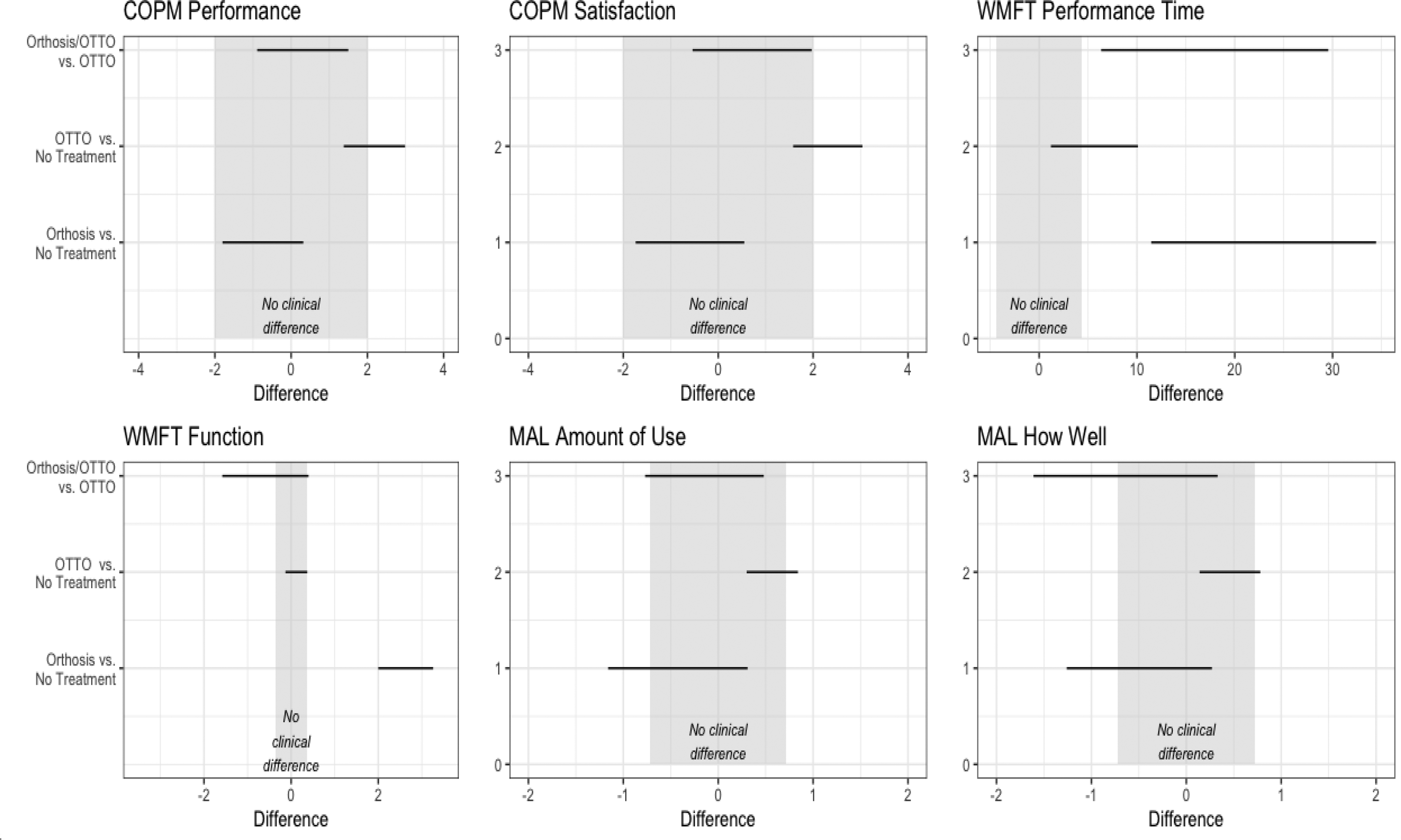
95% credible intervals for the three contrasts for each primary outcome; the ROPE (gray-shaded area) signifies differences that are not clinically significant.
Estimate of Contrast, Standard Errors, and 95% Credible Intervals for the Primary Study Outcomes
Note. COPM = Canadian Occupational Performance Measure; MAL = Motor Activity Log; OTTO = occupational therapy task oriented; WMFT = Wolf Motor Function Test.
Orthosis as Sole Intervention
There appears to be no clinical effect of the orthosis on either COPM measure. On the WMFT, the orthosis intervention seems to be associated with both an increase in performance time and in function compared with no treatment. It is unclear whether the orthosis affects either MAL measure.
OTTO as Sole Intervention
There seems to be no effect of OTTO (compared with no treatment) on WMFT function or on MAL subscales. On the two COPM subscales (Performance and Satisfaction), there is some evidence of a positive effect of OTTO, albeit with some uncertainty. There is also some evidence that the OTTO intervention is associated with higher performance times on the WFMT, although again with some uncertainty.
Orthosis + OTTO Compared With OTTO
There seems to be no additional effect of orthosis, above and beyond any effect of OTTO, on either COPM subscale or on the MAL Amount of Use subscale. The evidence points to an increase in performance time for participants receiving both orthosis and OTTO, as measured with the WMFT. There is too much uncertainty in the plots for the WMFT Function and MAL Quality of Movement measures to determine whether there is an effect.
Adherence to Orthotic Use
As a result of multiple technical issues with the wristband, it was not possible to quantify orthosis adherence.
Discussion
Efficacy of the Forearm Rotation Orthosis
Participants who received solely the orthosis did not show significantly greater improvement in functional performance than those who received no treatment. Participants who received OTTO plus the orthosis had no statistically greater improvement in functional performance compared with those who received OTTO alone. These results suggest that the forearm rotation orthosis was not an effective intervention alone and did not enhance outcomes when combined with the OTTO approach. Because we were not able to successfully monitor adherence to orthotic use, it is possible the orthosis was not worn sufficiently to produce a beneficial effect. Thus, efficacy of the forearm rotation orthosis for people with a hemiparetic arm remains uncertain.
The dynamic forearm rotation orthosis serves as an adjunct to facilitate functional performance if forearm movement is identified as the critical parameter responsible for enhancing or inhibiting functional performance. Sample heterogeneity may have weakened the detection of participants who would benefit from the orthosis. Indeed, forearm rotation movements were not identified as a critical parameter in all participants who received the orthosis. Likewise, several participants who received OTTO alone were considered good candidates who may have benefited from the orthosis. Because the OTTO intervention primarily focuses on the identified critical parameter, this lack of emphasis on forearm rotation may have lessened the beneficial effects of the orthosis for some participants.
Effects of OTTO Intervention
The results indicate that after OTTO, participants had clinically meaningful changes in self-perceived COPM task performance and satisfaction. Although there were trends indicating increased use and quality of use of the affected limb during real activities, changes on the MAL were not clinically important, and we did not find meaningful changes in WMFT UE function.
These findings are similar to those of Almhdawi et al. (2016). The OTTO approach urges therapists to partner with clients, and it emphasizes functional performance while facilitating problem-solving capabilities and generally focuses less on remediation of impairment (Mathiowetz, 2016). OTTO’s compensatory component would cause only small improvement at the impairment level (Almhdawi et al., 2016), which may account for the higher participant performance time observed on the WMFT. Consequently, one would expect participants receiving OTTO to demonstrate greater improvement in functional performance than in impairments.
One difference in the delivery of OTTO between the current study and Almhdawi et al. (2016) was the intensity of the home program. Almhdawi et al. used a logbook to track in-clinic training and home-based activities and to enhance adherence to therapy. The use of a logbook, however, is not a common clinical practice. This study aimed to use concepts of self-controlled learning. Participants took an active role in treatment and were encouraged to apply strategies or techniques learned in the clinic to their own context. For example, after working in the clinic on motor strategies for doing laundry, one participant reported increased use of the affected UE in emptying the dishwasher and in reorganizing his garage at home. Self-controlled learning strategies have been found to be valuable for motor acquisition and retention (Ste-Marie et al., 2013) and can enhance adherence to therapy (Radomski, 2011). There was evidence that the beneficial effects of OTTO lasted beyond the end of the study. When asked to provide summary feedback on the approach, several participants reported enhanced self-efficacy (“I can keep thinking about what I can do at home”; “you gave me hope; gave me confidence”).
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: OTTO is beneficial in enabling people poststroke to achieve clinically meaningful improvement in COPM performance and satisfaction. Elements of OTTO allow occupational therapists to identify critical control parameters that enhance or inhibit functional performance and use functional tasks valued by the person, provide repetitive practice of the selected tasks, and facilitate self-controlled learning. A greater emphasis in home programs on problem solving should enhance self-controlled learning and retention of therapeutic effects.
Study Limitations and Future Research
Efficacy of the forearm rotation orthosis for people poststroke was not fully tested as a result of a technical failure of the Nike+ FuelBand. A device with multiple accelerometers that automatically uploads data would be ideal. An orthosis wearing diary should be used.
This study examined only the immediate effects of OTTO by itself and in combination with the orthosis, not the retention effect. The COPM data could have been biased because it was collected by the investigator–interventionist. However, potential bias was limited because participants self-reported their level of performance and satisfaction. The sample size was small, which lessened the statistical power of the study. A more homogeneous sample of participants who could benefit from a forearm rotation orthosis would have enhanced the potential for a positive orthosis effect. Despite the small sample size, van de Schoot et al. (2015) noted that with informative prior distributions, acceptable power can be achieved with a small sample (as low as N = 8) using a Bayesian analysis. Participants with a variety of impairment difficulties, such as cognitive or psychological challenges, could be studied, and a future study could also examine whether therapeutic effects are maintained over time.
Conclusion
This study examined the efficacy of OTTO and of a forearm rotation orthosis separately and together for 14 persons poststroke. Six weeks of functional training provided evidence of clinically important benefits in self-perceived performance but mixed results in motor function. As a result of a lack of monitoring adherence, the efficacy of the forearm rotation orthosis remains uncertain.
Footnotes
1
N (0,1.5) refers to a normal distribution centered at 0 with standard deviation of 1.5.
Acknowledgments
The study was supported in part through a Care Providers of Minnesota grant and conducted at the University of Minnesota and University of Puget Sound. We thank all study participants and student evaluators Jacob Pearlman, Alison Johnson, Rachel Britton, Nicole Utt, and Leilani Sui Jones for their help in this project. This study was registered at ClinicalTrials.gov (NCT01987414). There is no conflict of interest to declare.