
Abstract
This review of research on participants’ experience of falls and fall prevention programs used in spinal cord rehabilitation highlights gaps in the available evidence.
Falls have long been an area of focus in the health literature because of the considerable impact they have on the economy and on individuals, including people with spinal cord injury (SCI; Stevens et al., 2006). People with SCI experience temporary or permanent changes in sensation and motor functioning; these changes put them at risk for falls (Amatachaya et al., 2015). Known intrinsic risk factors for falls include impaired balance, multiple medications, depression, hypotension, affected gait and muscle strength, and sensory problems, which all exist in the SCI population (American Geriatrics Society et al., 2001).
The SCI population is mostly male (Norton, 2010; Wyndaele & Wyndaele, 2006), often has intact cognition (Jørgensen & Roaldsen, 2017; Wannapakhe et al., 2014), and has a mean age of injury of 33 yr (Wyndaele & Wyndaele, 2006); these characteristics make them different from older adults and people with other neurological conditions. Exposure to fall risk is compounded by the active nature of the usual occupations of people with SCI, which may include work, family responsibilities, and sporting activities (Saverino et al., 2014). People who sustain a traumatic SCI may be impulsive and take more risks (Woodbury & Trieschmann, 1978) and may be susceptible to injuries because of mishaps, including falls (Krause, 2004). People with SCI have a considerable risk of osteoporosis, which is associated with a greater risk of fractures (Jiang et al., 2006). Injuries such as fractures may lead to hospitalization or extended bed rest and associated loss of strength and functional ability (Gavin-Dreschnack et al., 2005). Therefore, it is important that fall prevention be addressed as part of SCI rehabilitation.
Despite the potential consequences of falls, limited evidence exists on ways to reduce or manage falls after SCI (Finlayson & Peterson, 2010; Saverino et al., 2014). In a systematic review and meta-analysis of research on falls and factors associated with falls in a population with SCI, Khan et al. (2019) found that 78% of ambulatory patients and 69% of wheelchair users fell at least once over 12 mo. Contributing factors included biological, behavioral, and environmental factors. The specific search criteria used in the systematic review may not have captured the full breadth of evidence published on the topic, however (McKinstry et al., 2014). There is scope to expand this knowledge by exploring all levels of research evidence, including the perspective of people with SCI, to contribute to the development of falls prevention programs.
Occupational therapy practitioners working with people with SCI underpin their practice with conceptual practice models, such as the Canadian Model of Occupational Performance and Engagement (CMOP–E; Townsend & Polatajko, 2013). Because of their understanding of the influence of occupational performance on falls, occupational therapy practitioners are equipped with the knowledge and skills to lead the prevention of falls across age and diagnostic groups (Leland et al., 2012; Peterson et al., 2012). Occupational therapy practice in fall prevention may include identifying needed home modifications, ensuring patients’ functional ability to take medication and don appropriate footwear, and—as a member of the interprofessional team—providing fall education and prevention during engagement in occupations (Leland et al., 2012). With falls currently in the spotlight (Khan & Sadiq, 2017), an appraisal of the available literature through an occupational lens can support the development of an occupation-centered approach to fall prevention. Therefore, the aim of this study was to determine what is known from the existing literature about falls after SCI and to apply the CMOP–E to better understand elements to be addressed in fall education and prevention with this population.
Method
A scoping review was chosen to assess the potential size and scope of the available research literature (Grant & Booth, 2009). Scoping reviews extract a limited amount of information from published studies (Arksey & O’Malley, 2005) to inform practice, policy making, and research (Daudt et al., 2013) and to identify gaps and limitations in the existing body of knowledge to guide future research (McKinstry et al., 2014). In this scoping review, we followed the protocol outlined by Arksey and O’Malley (2005) with enhancements provided by Levac et al. (2010). Arksey and O’Malley described five stages for scoping reviews: (1) identifying the research question; (2) identifying relevant studies; (3) selecting studies; (4) charting the data; and (5) collating, summarizing, and reporting the results.
Stage 1: Identifying the Research Question
In the first stage, as recommended by Levac et al. (2010), we considered the overall outcome of the review when determining the research question, which was “What is known from the existing literature about falls after SCI?” For this scoping review, a fall was defined as “an unexpected event in which the participants come to rest on the ground, floor, or lower level” (Lamb et al., 2005, p. 1619). To clarify the focus of the scoping review, we considered the concept, target population, and health outcomes (Levac et al., 2010). The focus was narrowed to any studies that included adults with SCI and one or more of the following: incidence of falls, consequences of falls, contributing factors for falls, the person’s experience of falls, or interventions to prevent falls for people with an existing SCI.
Stage 2: Identifying Relevant Studies
In the second stage, we identified all possible relevant studies by searching databases using a systematic search strategy (Arksey & O’Malley, 2005). We searched the databases with the assistance of a librarian on September 23, 2019, using the terms “SCI” and “falls” with MeSH terms and truncations. Databases searched included PubMed, CINAHL, EMBASE, OTseeker, PEDro, PsycINFO, Cochrane, and Scopus, with no limits set on date or language. Search strategies for PubMed and PsycINFO can be found in Table 1. Additional articles were identified from reference lists. A summary of the results of searches and reasons for exclusion of full-text articles are outlined in Figure 1.
Search Strategies for PubMed and PsycINFO
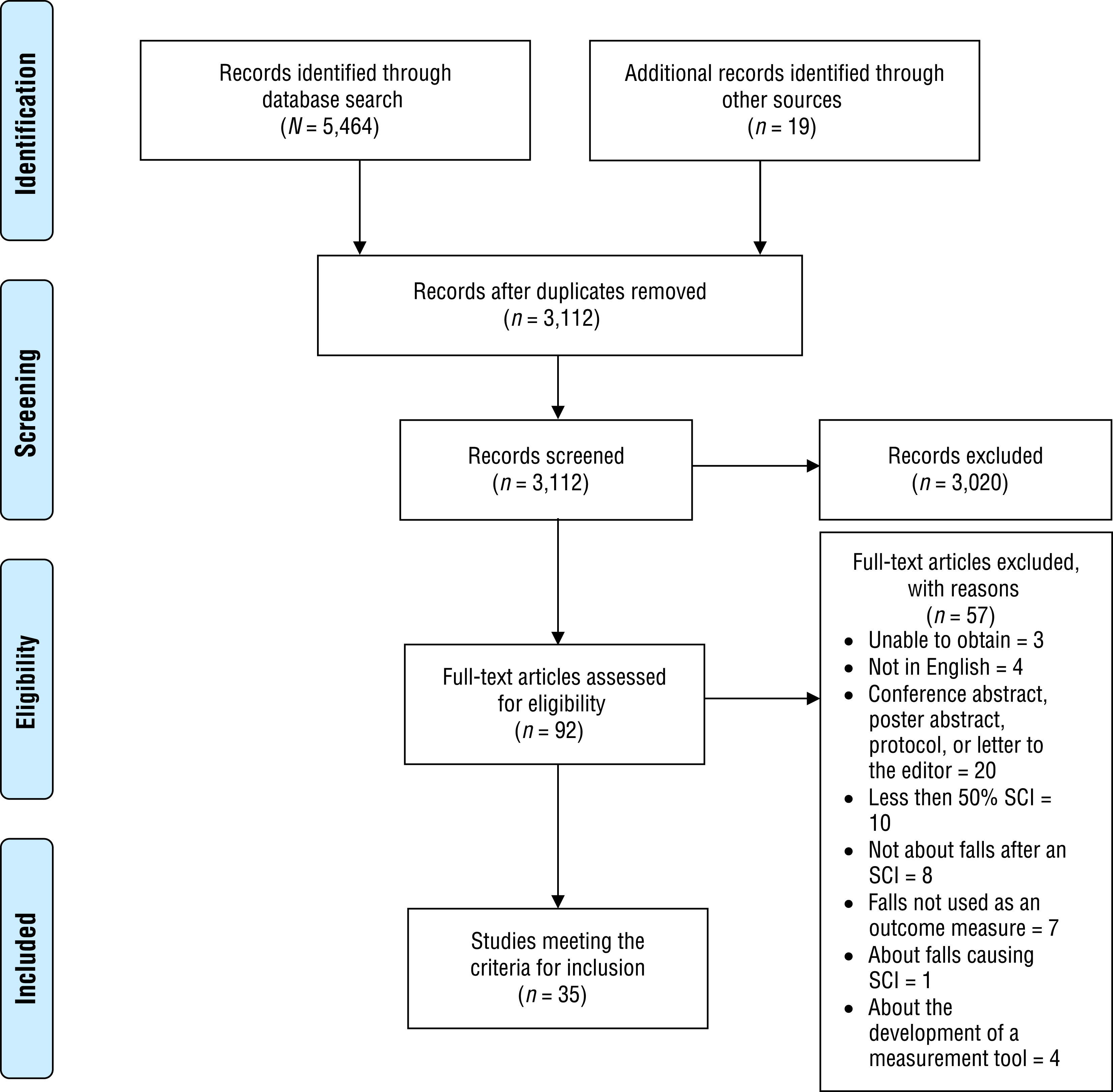
Flow diagram for inclusion and exclusion of peer-reviewed studies in the scoping review.
Stage 3: Selecting Studies
The next stage involved selecting articles that were eligible for inclusion using predetermined criteria. Kathryn Marshall reviewed titles and abstracts in EndNote (Clarivate Analytics, Philadelphia) against inclusion and exclusion criteria set with the team. Details of inclusion and exclusion criteria can be found in Table 2. The full text was obtained for all articles that met the inclusion criteria and for articles that did not have an abstract and could not be excluded by title only. Full texts were reviewed by two authors (Kathryn Marshall and Andrea McKittrick); poster abstracts, conference abstracts, protocols, and letters to the editor were excluded because more than half of these documents had also been published as articles included in the full-text review. The two reviewers met to discuss any articles for which the decision about inclusion was different (n = 17) and reached consensus. When disagreement continued (n = 7), the third author, Louise Gustafsson, helped them reach a decision (Levac et al., 2010).
Inclusion and Exclusion Criteria
Stage 4: Charting the Data
The authors obtained key information from the articles by sifting, charting, and sorting information into a data charting form (Arksey & O’Malley, 2005). Each included article was read multiple times, and data were charted in an Excel (Microsoft Corp., Redmond, WA) spreadsheet. The spreadsheet was continually updated as information was deemed relevant and worth reporting on (Levac et al., 2010). Data extracted included the study aims, country of publication, study design, participant demographics, and key findings. Findings were organized into the categories of incidence of falls, consequences, contributing factors, comparison with other diagnoses, patient experience, and fall prevention strategies.
Stage 5: Collating, Summarizing, and Reporting the Results
The final stage involved presenting an overview of all the information reviewed with the extent, nature, and distribution of the articles summarized (Levac et al., 2010). An occupational therapy model, the CMOP–E, was chosen to organize the contributing factors. Typically, a critical appraisal of each article is not a required step in a scoping review and therefore was not completed as part of this review (McKinstry et al., 2014). However, we classified the quantitative studies using the National Health and Medical Research Council evidence hierarchy for etiology studies (National Institute of Clinical Studies, 2009). This hierarchy provided useful information for considering the gaps in evidence and determining whether the evidence could be used to guide practice (Grant & Booth, 2009). Studies were classified as Level I (systematic review), Level II (prospective cohort study), Level III-1 (all or none), Level III-2 (retrospective cohort study), Level III-3 (case control study), and Level IV (cross-sectional study or case series) by Marshall in consultation with Jennifer Fleming.
Results
Thirty-five articles met the inclusion and exclusion criteria. These articles were published between 1993 and 2019 and were largely quantitative studies (n = 33; 94%). A summary of the included articles can be found in Table A.1 in the Appendix. The quantitative studies included mixed method design studies (n = 2), prospective cohort studies (n = 9), cross-sectional studies (n = 8), case series (n = 8), case–control studies (n = 5), and retrospective cohort studies (n = 3). Studies were conducted by research groups in the United States (n = 13), Thailand (n = 9), Sweden and Norway (n = 5), Switzerland (n = 2), Taiwan (n = 2), Canada (n = 2), Australia (n = 1), and France (n = 1). All studies were conducted in the community, with the exception of 2 studies conducted in inpatient settings and 1 study that included a mix of inpatients and outpatients. In 29 studies, only people with SCI were recruited; the remaining 6 studies recruited participants with a mix of diagnoses that included, but were not isolated to, stroke, amputation, multiple sclerosis (MS), muscular dystrophy (MD), arthritis, cerebral palsy, brain injury, polio, Guillain-Barré syndrome, and a mix of other acute medical conditions.
The studies were largely observational, with only 2 articles reporting on whether an implemented intervention was effective in reducing falls. Of the 35 articles, 22 collected at least some data retrospectively (e.g., recall or review of falls in the previous 6 mo). Methods for collecting data retrospectively included questionnaire (n = 8), interview and assessment (n = 7), chart review (n = 3), a mix of chart review and interview or questionnaire (n = 3), and incidence report (n = 1). When data were collected prospectively, it was largely to gather information on fall rates. Methods of collecting fall data prospectively included phone call (n = 4), falls diary with follow-up phone call (n = 4), text message with follow-up phone call (n = 3), calendar returned via mail with follow-up phone call (n = 1), and a falls diary returned via mail (n = 1). In 4 of the studies, fall information was confirmed with caregivers.
Incidence of Falls
Twenty-eight (80%) articles reported on the incidence of falls, accidents, or fall-related injuries. Fall rates in people with SCI were reported in only 20 articles (57%). From the data available for people in a wheelchair, rates at 6 mo were 36% and at 1 yr ranged from 31% to 73% (see Table A.1). For people who were ambulatory, rates at 6 mo ranged from 17% to 54% and at 1 yr from 75% to 82% (see Table A.1). Two of the articles did not separate rates for wheelchair users and ambulatory participants. Twelve of the 20 articles discussed the circumstances surrounding falls, including time of day (n = 7), location (n = 10), and what the participant was doing at the time of the fall (n = 9). Falls for wheelchair users and ambulatory participants were dispersed throughout the day, with some authors finding that falls happened in the morning to early evening (Forslund et al., 2017; Jørgensen et al., 2017; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013; Wannapakhe et al., 2014) and others finding that falls happened in the afternoon or evening (Amatachaya et al., 2011, 2019; Brotherton et al., 2007a).
Eight studies reported that participants fell indoors (Amatachaya et al., 2011, 2015, 2019; Brotherton et al., 2007a; Forslund et al., 2017; Jørgensen et al., 2017; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013; Wannapakhe et al., 2014). Kirby et al. (1994) reported on a mixed population who used a wheelchair and found that more than twice the amount of falls occurred outdoors as indoors. Participants who were ambulatory reported that the circumstance of the fall was stumbling over an obstacle (Amatachaya et al., 2015, 2019; Wannapakhe et al., 2014), lower limb weakness (Amatachaya et al., 2019), changing posture (Phonthee, Saengsuwan, & Amatachaya, 2013; Wannapakhe et al., 2014), completing a transfer (Jørgensen et al., 2017), and walking on uneven or slippery surfaces (Jørgensen et al., 2017). Participants who used a wheelchair reported that the circumstance of the fall was completing a transfer (Forslund et al., 2017) and pushing the wheelchair on flat ground (Forslund et al., 2017). For participants in a mixed caseload, the circumstance of the fall included negotiating ramps, curbs, and doorways in a wheelchair (Kirby et al., 1994).
Consequences of Falls
The specific consequences of falls were reported in 26 of the 35 articles. Physical consequences were listed most often, with 9 articles reporting injuries as a consequence of falls. The rate of injurious falls for people with SCI who were ambulatory was 30% at 6 mo and ranged from 20% to 65% at 12 mo (see Table A.1). The rate of injurious falls for participants with SCI who used a wheelchair over a 1-yr period ranged from 14% to 34% (see Table A.1).
Minor or moderate injuries occurred most frequently and were not specific to wheelchair users or ambulatory patients. For people with SCI, such injuries included bruises (Amatachaya et al., 2011, 2019; Brotherton et al., 2007a; Nelson et al., 2010; Wannapakhe et al., 2015), skin abrasions (Brotherton et al., 2007a; Nelson et al., 2010; Wannapakhe et al., 2014), and pain (Amatachaya et al., 2011; Nelson et al., 2010; Phonthee, Saengsuwan, & Amatachaya, 2013; Wannapakhe et al., 2014, 2015).
Serious injuries resulting from falls occurred less frequently, ranging from 1% to 18% of the total number of participants with SCI who experienced a fall (Amatachaya et al., 2011, 2019; Brotherton et al., 2007a; Phonthee, Saengsuwan, & Amatachaya, 2013; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013; Srisim et al., 2015; Wannapakhe et al., 2015). When studies considered all injurious falls in people with SCI, 4% of people who were ambulatory had serious consequences, and 10% to 14% of people who used a wheelchair had serious consequences (Forslund et al., 2017; Jørgensen et al., 2017; Nelson et al., 2010). Fractures were the most frequent serious injury for both wheelchair users and ambulatory patients (Amatachaya et al., 2011; Brotherton et al., 2007a; Forslund et al., 2017; Jørgensen et al., 2017; Nelson et al., 2010; Phonthee, Saengsuwan, & Amatachaya, 2013; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013; Srisim et al., 2015). Three articles included only people who had an SCI and a fracture and used a wheelchair; of these participants, 26% to 86% had fractures caused by a fall (Fattal et al., 2011; Jannings, 2017; Nelson et al., 2003).
Psychological consequences of falls were documented in fewer studies. Fear of falling was reported in 2 studies specific to people with SCI (Wannapakhe et al., 2014, 2015). Sung et al. (2019) found that 73% of a mixed sample of people with SCI and MS reported a fear of falling. Other psychological consequences included feeling unsafe using a shower commode (Nelson et al., 1993) and, in a mixed caseload, injury to pride or ego (Kirby et al., 1994).
Personal costs of falls and fall-related injuries for people with SCI who were ambulatory included restricted ability to engage in the community (Brotherton et al., 2007a; Phonthee, Saengsuwan, & Amatachaya, 2013), limitations to daily activities (Saunders & Krause, 2015), and reduced mobility and social communication (Wannapakhe et al., 2014, 2015). For both wheelchair users and ambulatory patients, the personal costs included prolonged bed rest (Fattal et al., 2011; Jannings, 2017; Wannapakhe et al., 2015) and hospitalization (Amatachaya et al., 2011; Fattal et al., 2011; Nelson et al., 1993; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013; Saunders & Krause, 2015). Fractures in people with SCI had an impact on discharge destination (Akhigbe et al., 2015) and caused an increase in the amount of care required (Akhigbe et al., 2015; Jannings, 2017). Extra care and community services required because of immobilization and skin conditions caused by devices to manage the fracture created additional financial costs (Jannings, 2017). Modified or new equipment was required by 83% of patients who sustained a fracture (Akhigbe et al., 2015).
Patients’ Experience of Falls
Two articles examined falls from the perspective of the person with SCI using face-to-face interviews (Jørgensen & Roaldsen, 2017; Musselman et al., 2018) and photographs to guide the interview (Musselman et al., 2018). A common theme in the two studies was that participants identified the threat of falling but were willing to accept increased risk of falls to participate in activities that they wanted to do and that maintained their self-image. Participants wanted to maintain independence and appear “normal” in society.
Fall Prevention Strategies
Two studies (Forrest et al., 2012; Rice et al., 2020) reported on the implementation of a fall prevention program. Forrest et al. (2012) completed a study on a nonspecific inpatient rehabilitation ward and reported a fall rate of 12.5% specific to participants with SCI (27 of 216) over 4 yr after the introduction of a fall prevention program. The SCI group was a “high-falling” group, but it is unclear whether the intervention reduced the number of falls over the 4 yr of intervention because no control group was included.
Rice et al. (2020) conducted a pilot study with the primary goal of reducing fall rates and concerns about falling in patients with SCI who used a manual wheelchair. Secondary outcomes were to improve quality of life and community participation. The intervention provided education on transfers using a video, practice of transfers, core strengthening, and discussions with participants about problems they identified in their own environment and assistance provided to problem solve these issues. The incidence of falls decreased significantly in the 3 mo of intervention, and fall concerns decreased, but not significantly. Improvements were noted in postural control and in quality of life in the Physical and Psychological Well-Being domains but not in the Social Relationships and Environment domains.
Further insight into factors that could contribute to fall intervention programs were gained from participant reports in other studies included in Table A.1. For example, Musselman et al. (2018) found that ambulatory participants reported greater satisfaction with fall prevention education offered in rehabilitation compared with wheelchair users, who were disappointed in the amount of wheelchair training skills and felt they received minimal fall prevention training.
Contributing Factors for Falls
The contributing factors for falls, wheelchair accidents, fractures, and injuries were discussed in 28 articles. Table A.2 summarizes the contributing factors identified from the scoping review using the core domains of the CMOP–E. The Person domain was the most prevalent, contributing to falls in 22 of 30 studies, followed by Environment in 13 of 30 studies and Occupation in 11 of 30 studies.
Person
Impaired balance was associated with fall risk or risk of fall-related injuries in 9 studies (see Table A.2). Reduced muscle power was also noted to increase risk of falls and fractures, as well as spasticity and pain. Multiple authors focused on assessments of physical function to predict falls for people who were ambulatory, including the 10-Meter Walk Test, the 6-Minute Walk Test, the Timed Up and Go test, the Berg Balance Scale, the Functional Reach Test, the Choice Response Test, and the Five Times Sit to Stand Test. Nine studies found that aspects of mobility were associated with fall risk, fall-related injuries, and wheelchair accidents. These aspects included mobility status, use of an assistive device, and experience. The affective and cognitive components were less represented, with only 5 studies reporting fear of falling, depression, and distraction as contributing factors for falls. No spiritual factors were identified.
Environment
Twelve studies reported factors related to the physical environment such as obstacles, uneven surfaces, and poor access that were largely self-reported (see Table A.2). Studies that focused on equipment were mostly related to wheelchairs and seatbelts. Institutional, cultural, and social aspects were not widely represented, with only 5 studies identifying related contributing factors.
Occupation
The domains of Self-Care, Productivity, and Leisure were evenly represented among contributing factors (see Table A.2). Four studies focused on linking participants’ fall risk to level of functional ability as measured by the FIM® (Uniform Data System for Medical Rehabilitation, 1997; FIM® is a trademark of the Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc.) and the Spinal Cord Independence Measure (SCIM; Catz et al., 1997). Exercise was reported as both a negative and a positive factor for falls in 3 of the studies.
Other Factors
Several other factors that did not fit into the CMOP–E domains were mentioned in the literature (see Table A.2). Several authors found that being younger and male contributed to an increased risk of falls. Being categorized as at high risk of falls on the Downton Falls Risk Index was associated with an increased risk of falls.
Of the 28 articles that reported on contributing factors, 13 included only people who were ambulatory, 7 included only people in a wheelchair, 6 included both, and 2 did not report mobility status. Of the 6 articles that included participants with both forms of mobility, 2 articles made clear distinctions between factors for wheelchair users and factors for ambulatory participants. For both types of participant, poor balance, a cluttered environment with obstacles, poor quality of life, and a history falls were identified as contributing factors. For wheelchair users, pain, spasticity, depression, higher scores on the SCIM and FIM, and fewer years with SCI were significant contributing factors, whereas for ambulatory participants, being ambulant and having a fear of falling were significant factors.
Comparison With Other Diagnoses
Six studies included participants with a mix of diagnoses, and 4 of these studies made comparisons between participants with SCI and those with other diagnoses (see Table A.2). Having a diagnosis of SCI was reported to increase participants’ risk of falls and accidents (Forrest et al., 2012; Kirby et al., 1994). Contributing factors for falls differed for participants with SCI compared with participants with MS, MD, and post-polio syndrome.
Discussion
The aim of this scoping review was to determine what is known from the existing literature about falls after SCI and to apply the CMOP–E to inform fall prevention intervention. A wealth of research exists on the incidence of falls, consequences of falls, and contributing factors for falls, which occupational therapy practitioners could use implementing fall prevention strategies. The CMOP–E provides an appropriate structure to organize the contributing factors for falls to both highlight research gaps and aid development of fall prevention intervention. This scoping review highlighted that research on the patients’ experience of falls and fall prevention programs in spinal cord rehabilitation is extremely limited and that a considerable research gap exists.
The consequences of falls for people with SCI were clearly demonstrated. The serious physical and personal cost of fractures on a person’s life is well documented, and education is recommended on fracture risks, ways to control osteoporosis, appropriate equipment, and promotion of physical activity (Akhigbe et al., 2015; Fattal et al., 2011; Jannings, 2017). In contrast, it is unclear whether minor injuries have a cumulative effect on a person’s life and whether they should also be addressed in fall education. This area requires further research in the SCI population.
The psychological impact of falls on the person was reported in only 5 of the studies. With falls being one of the most prevalent reasons for SCI, patients may have a fear of falling during the rehabilitation process (John et al., 2010), interfering with the rehabilitation progress (Boswell-Ruys et al., 2010). Jørgensen et al. (2017) anticipated that the effects of fear of falling on functional decline in older adults may apply to the SCI population. Therefore, further exploration is needed to understand the psychological impact of falls on people’s occupations and rehabilitation.
Studies of fall prevention programs have shown them to be effective in reducing falls in older adults (Hill et al., 2015). However, because of different contributing factors and characteristics of the populations, this research is not suitable to be generalized to people with SCI. Although many studies in this scoping review show that researchers have started to consider the when, what, where, and who of fall prevention and to make recommendations for what is required from a fall prevention program, only 1 published study attempted a fall prevention program.
Study authors agreed that screening and assessment across the continuum of care are an important part of fall prevention, starting at the onset of SCI and extending over life-long follow-up, including when changes are made to equipment or functional status (Brotherton et al., 2007a, 2007b; Forslund et al., 2017; Jørgensen et al., 2017; Nelson et al., 2010). Personal factors such as falls history, functional ability, balance, equipment and environment, and skills and assessment of other researched contributing factors should be explored further (Brotherton et al., 2007a, 2007b; Nelson et al., 2010). Multiple authors identified contributing factors for falls and made recommendations that could be used in a clinical setting. The application of the CMOP–E enables conceptualization of these factors within an occupational therapy framework.
With rehabilitation often completed in predictable and uncluttered environments, emphasis has been placed on the need to replicate a real-world environment for therapy and to consider intrinsic and extrinsic factors (Amatachaya et al., 2015; Phonthee, Saengsuwan, & Amatachaya, 2013; Srisim et al., 2015; Wannapakhe et al., 2014). Nelson et al. (2010) suggested that people using a wheelchair may fall because of difficulty translating skills learned in therapy to real-life situations and environments and delay in obtaining equipment to allow adequate practice before discharge. Occupational therapy practitioners therefore may need to consider what is the best environment for falls rehabilitation.
This scoping review highlighted that although people who are ambulant and those who use a wheelchair share some contributing factors for falls, they also have differing contributing factors. Therefore, fall prevention strategies need to target these groups differently (Jørgensen et al., 2016). With ambulation remaining a goal for a majority of people, the need to balance the increased risk of falls is essential (Saunders et al., 2013) for both wheelchair users and ambulatory people (Sung et al., 2019). In addition, contributing factors vary across diagnosis groups, further emphasizing the need for fall prevention for people with SCI to be targeted (Matsuda et al., 2015).
Currently, little is known about the patient experience of falls, with only 2 studies having explored this topic (Jørgensen & Roaldsen, 2017; Musselman et al., 2018). To provide evidence-based intervention, clinicians are required to consider the combination of “best research evidence, clinical expertise, and the client’s values and circumstances” (Hoffmann et al., 2009, p. 3). Therefore, clinicians providing fall education would benefit from a greater understanding of patient perceptions, including their values and circumstances, to inform program development and delivery.
Munce et al. (2016) recommended that self-management programs incorporate the knowledge and beliefs held by people with SCI to empower them and improve their overall quality of life. Fall prevention needs to acknowledge that patients can take responsibility for and contribute their expertise to their care (Child et al., 2012). This scoping review has highlighted that little is known about the beliefs of patients regarding fall prevention, which is a considerable barrier to increasing the acceptance of fall prevention.
Limitations
A scoping review is, by nature, broad in its search. The results of our search led to presentations of varied topic areas with information that is difficult to compare because of differing study designs. To mitigate this difficulty, we categorized the information to show clinicians the breadth of evidence for each topic area to aid their decision making. Additionally, because the inclusion criteria allowed studies on mixed populations, the information presented in this review includes some research on conditions other than SCI. However, the inclusion criteria did specify that the study had to include at least 50% of participants with SCI or to report data for these participants separately, giving some confidence that the conclusions are relevant for the SCI population.
Implications for Occupational Therapy Practice
This scoping review adds to existing work on falls after SCI and has the following implications for occupational therapy practice:
The CMOP–E has demonstrated usefulness as a framework for occupational therapy practitioners to consider fall prevention across multiple domains.
Occupational therapy practitioners and researchers can use the results of this scoping review to recognize the importance of this issue, consider potential areas of focus for fall prevention, and identify gaps in the research evidence.
Conclusion
In this scoping review we aimed to provide a broad overview of the current literature on falls after SCI. It is clear that people with SCI fall, and they often incur some detrimental consequence for falling. People with SCI need to be able to independently decide whether the benefit of taking risks outweighs the possible consequences. Although health professionals’ knowledge often is dominant in rehabilitation, the lived experience adds intrinsic value and may be given more value in patients’ decision making (Stuifbergen et al., 2010; Yoshida et al., 2015). Further research examining the lived experience of falls is needed to inform fall prevention programs in SCI rehabilitation.
Footnotes
Acknowledgments
This research was supported by a research support grant from the University of Queensland Spinal Injury Research Fund.
*
Indicates studies included in the scoping review.
Appendix. Supplemental Tables
Summary of Contributing Factors for Falls, Fall-Related Injuries, Fractures, and Accidents
| Domain | Mobility Status | Contributing Factors |
|
|
||
| Physical | ||
| Balance | Ambulatory, wheelchair | Poor balance was self-reported as a contributor to falls (Brotherton et al., 2007a; Matsuda et al., 2015 a ; Nelson et al., 2003; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013; Saunders & Krause, 2015; Sung et al., 2019 a ). |
| Wheelchair | Poor balance contributed to falls that caused fracture (Nelson et al., 2003). | |
| Ambulatory | Poor balance increased risk of fall-related injuries (Saunders et al., 2013). | |
| Ambulatory | No association was found between number of falls and BBS scores (Wirz et al., 2010). | |
| Unknown | Rapid reach and grasp balance reaction prevented falls (Lin et al., 2008). | |
| Muscle power | Ambulatory, wheelchair | Muscle weakness contributed to falls (Brotherton et al., 2007a; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013; Srisim et al., 2015; Sung et al., 2019 a ). |
| Spasticity | Wheelchair | Spasticity was associated with increased risk of falls (Sung et al., 2019 a ). |
| Wheelchair | Muscle spasm contributed to falls causing fracture (Nelson et al., 2003). | |
| Mobility | Ambulatory | Ambulation increased fall risk (Jørgensen et al., 2016; Wannapakhe et al., 2015). |
| Ambulatory, wheelchair | Spending equal time walking and wheeling resulted in a higher risk for falls and fall-related injuries compared with using solely a wheelchair (Saunders et al., 2013; Saunders & Krause, 2015). | |
| Ambulatory | Use of an assistive device was a negative and positive factor for falls (Matsuda et al., 2015 a ; Phonthee, Saengsuwan, & Amatachaya, 2013). | |
| Ambulatory | Use of a walker was associated with decreased risk of falls (Brotherton et al., 2007b; Phonthee, Saengsuwan, & Amatachaya, 2013). | |
| Ambulatory | Use of a cane or crutch was associated with an increased risk of fall-related injuries (Saunders et al., 2013). | |
| Wheelchair | Inexperience was associated with an increased risk of wheelchair accidents (Chen et al., 2011 a ). | |
| Ambulatory | Walking asymmetrically was associated with an increased risk of falls (Kumprou et al., 2018). | |
| Pain | Wheelchair | Increased pain in the previous 2 mo was associated with an increased risk of falls and fall-related injuries (Nelson et al., 2010). |
| Functional ability | Ambulatory | Increased time to perform the 10MWT was associated with increased risk of falls (Forslund et al., 2019; Jørgensen et al., 2017). |
| Ambulatory | Both higher and lower levels of functioning on the 6MWT and TUG were associated with increased risk of falls (Phonthee, Saengsuwan, & Amatachaya, 2013; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013). | |
| Ambulatory | No difference between fallers and nonfallers on the TUG, 10MWT, 6MWT, and BBS were found at 6 mo postdischarge (Wannapakhe et al., 2014). | |
| Ambulatory | The FRT best predicted multiple falls compared with other tests of functional ability (Srisim et al., 2015). | |
| Wheelchair | Independence in transfers was associated with increased risk of wheelchair accidents (Kirby et al., 1994 a ). | |
| Ambulatory | Needing assistance with walking was associated with increased risk of fall-related injuries (Saunders et al., 2013). | |
| Ambulatory, wheelchair | Ability to get up off the ground was associated with 2.2 times increased risk of falls (Jørgensen et al., 2016). | |
| Ambulatory | No association was found between choice response time and falls (Labruyère & van Hedel, 2011). | |
| Affective | Ambulatory | Fear of falling was associated with 4.0 to 6.1 times increased risk of falls (Brotherton et al., 2007b; Jørgensen et al., 2017; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013). |
| Ambulatory | Fear of falling was associated with 4.3 times increased fall-related injuries (Jørgensen et al., 2017). | |
| Wheelchair | Symptoms of depression were associated with higher risk of falls (Forslund et al., 2019). | |
| Cognitive | Ambulatory, wheelchair | Distraction was associated with increased risk of falls (Chen et al., 2011 a ; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013; Sung et al., 2019 a ). |
| Spiritual | Not addressed in articles | |
|
|
||
| Physical | ||
| Wheelchair | Wheelchair | Shorter length (Nelson et al., 2010), light weight, rear wheelchair chamber, and adjustable real axle position were associated with increased risk of falls (Kirby et al., 1994 a ). |
| Wheelchair | Not using a prescribed wheelchair and not completing regular maintenance were associated with increased risk of wheelchair accidents (Chen et al., 2011 a ). | |
| Wheelchair | Using a wheelchair daily and propelling with both hands were associated with increased risk of wheelchair accidents (Kirby et al., 1994 a ). | |
| Wheelchair | Equipment failure was associated with increased risk of falls (Sung et al., 2019 a ) and fractures (Nelson et al., 2003). | |
| Seatbelt | Wheelchair | In 5 of 7 falls that resulted in a fracture, participants were not wearing a seat belt (Jannings, 2017). |
| Wheelchair | Not wearing a seat belt contributed to falls that caused fractures (Nelson et al., 2003). | |
|
|
||
| Physical | Ambulatory, wheelchair | Obstacles and a hazardous and cluttered environment were associated with increased risk of falls (Brotherton et al., 2007a; Chen et al., 2011 a ; Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013; Srisim et al., 2015; Sung et al., 2019 a ). |
| Ambulatory | Inability to cross obstacles was associated (Amatachaya et al., 2019) and not associated (Amatachaya et al., 2015) with falls. | |
| Wheelchair | Uneven surfaces contributed to fractures (Nelson et al., 2003). | |
| Wheelchair | Poor access to the home entrance was associated with increased risk of fall-related injuries (Nelson et al., 2010). | |
| Institutional | Unknown | A Posey restraint order was associated with increased risk of falls in a mixed caseload (Aisen et al., 1994 a ). |
| Cultural | Unknown | Being non-White was associated with increased risk of fall-related injuries (Saunders & Krause, 2015). |
| Wheelchair | Greater risk of wheelchair accidents was found if participants were not in the habit of wearing a seat belt (Chen et al., 2011 a ). | |
| Social | Wheelchair | Caregiver error was associated with falls in 4 of the 7 participants (Jannings, 2017). |
| Wheelchair | Wheelchair repairs completed by a dealer or unknown person were associated with increased risk of accidents compared with wheelchair repairs completed by a family member or friend (Kirby et al., 1994 a ). | |
|
|
||
| Self-care | Unknown | Prescription medication use was associated with increased risk of fall-related injuries (Saunders & Krause, 2015). |
| Ambulatory | Misuse of medications increased the risk of fall-related injuries by 2.53 (Saunders et al., 2013). | |
| Wheelchair | Higher scores on the SCIM were associated with increased risk of falls (Forslund et al., 2017, 2019; Jørgensen et al., 2016). | |
| Unknown | Lower scores on the FIM® were associated with increased risk of falls (Forrest et al., 2012 a ). | |
| Wheelchair | Higher scores on the FIM were associated with increased risk of falls and fall-related injuries (Nelson et al., 2010). | |
| Ambulatory | FIM Locomotion scores of 6 and 7 were associated with falls (Phonthee, Saengsuwan, & Amatachaya, 2013). | |
| Productivity | Ambulatory | High school completion was associated with increased risk of falls compared with primary school completion (Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013). |
| Leisure | Ambulatory, wheelchair | Exercise b was associated with reduced risk of falls (Brotherton et al., 2007b) and increased risk of falls (Jørgensen et al., 2016; Matsuda et al., 2015 a ). |
| Ambulatory | Less exercise was associated with increased risk of fall-related injuries (Saunders et al., 2013). | |
| Wheelchair | Using a wheelchair for recreation was associated with increased risk of accidents (Kirby et al., 1994 a ). | |
| Wheelchair | Alcohol abuse was associated with increased risk of falls (Nelson et al., 2010; Sung et al., 2019 a ). | |
|
|
||
| Comorbid conditions | Ambulatory, unknown (wheelchair) | Higher number of comorbidities was associated with increased risk of falls (Brotherton et al., 2007b; Matsuda et al., 2015 a ). |
| Ambulatory | Dizziness and arthritis were associated with increased risk of falls (Brotherton et al., 2007b). | |
| Wheelchair | Narcolepsy contributed to falls that caused fracture (Nelson et al., 2003). | |
| Diagnosis of SCI | Wheelchair, unknown (ambulatory) | Diagnosis of SCI was associated with increased risk of falls compared with other diagnoses (Forrest et al., 2012 a ; Kirby et al., 1994 a ). |
| Wheelchair | Fewer years with SCI were associated with increased risk of falls (Nelson et al., 2010). | |
| Ambulatory | AIS C-level of injury increased risks of falls compared with AIS D-level of injury (Phonthee, Saengsuwan, Siritaratiwat, & Amatachaya, 2013). | |
| Ambulatory | Higher level of injury and high degree of lesion severity were associated with increased risk of falls (Amatachaya et al., 2019). | |
| Age | Ambulatory, wheelchair | Being younger was associated with increased risk of falls (Amatachaya et al., 2015; Kirby et al., 1994 a ), with falls decreasing by 3% per year of age (Jørgensen et al., 2016). |
| Sex | Wheelchair | Being male was associated with increased risk of falls (Jørgensen et al., 2016, Kirby et al., 1994 a ). |
| Quality of life | Ambulatory, wheelchair | Increased quality of life was associated with reduced risk of falls (Jørgensen et al., 2016) and fall-related injuries in wheelchair users (Forslund et al., 2017). |
| History of falls | Ambulatory, wheelchair | History of falls was associated with increased risk of falls (Forslund et al., 2017, 2019; Jørgensen et al., 2017; Nelson et al., 2010) and fall-related injuries (Jørgensen et al., 2017; Nelson et al., 2010). |
| Fall-risk screen | Ambulatory, wheelchair | Being categorized as “high risk of falls” on the Downton Falls Risk Index was associated with increased risk of falls (Forslund et al., 2019). |
| Other | Wheelchair | Excessive wheelchair speed contributed to falls that caused fractures (Nelson et al., 2003). |
Note. AIS = Association Impairment Scale; BBS = Berg Balance Scale; CMOP–E = Canadian Model of Occupational Performance and Engagement; FRT = Functional Reach Test; SCI = spinal cord injury; SCIM = Spinal Cord Independence Measure; 6MWT = 6-Minute Walk Test; 10MWT = 10-Meter Walk Test; TUG = Timed Up and Go test.
Study included a mixed caseload.
Exercise may also be classified as self-care or leisure, depending on the reason for the exercise.