
Abstract
Structured occupational reflection can enhance the recovery of adults living with SMI in inpatient psychiatry units.
Occupational therapy practitioners have been facilitating occupational reflection among their clients for decades (Jackson et al., 1998). These practices help clients understand the importance of their occupational choices and occupational patterns in relation to their health (Jackson et al., 1998). They are a useful strategy to communicate the power of harnessing occupation to effect positive health and well-being (Atler, 2015). We define occupational reflection as a structured reflective process during which a person carefully analyzes the impact of their daily occupational patterns and routines on their health and well-being.
In mental health settings, assessing patterns of engagement in occupation can be a vital step in the intervention process because patterns of occupational participation are intimately related to the recovery and health of adults living with serious mental illness (SMI; Leufstadius et al., 2008). This process can be used as a stand-alone intervention or in combination with other interventions to promote recovery. In inpatient settings, occupational reflection presents a unique opportunity for clients to engage in therapist-assisted daily reflections regarding their new activity patterns on the unit and to identify positive changes that can contribute to health and well-being after discharge. Despite this potential, little research has explored the utility of incorporating systematic occupational reflection into standard occupational therapy practice in inpatient mental health settings.
In community-based psychiatry, research has demonstrated that occupational self-analysis can assist clients in making meaningful changes to their activity patterns to promote health and recovery (Erlandsson, 2013). For example, in the Redesigning Daily Occupations program, self-analysis of occupational patterns is the critical first step in supporting women with stress disorders in their return to work (Erlandsson, 2013). In inpatient psychiatry, researchers have shown that analyzing occupational engagement through a narrative approach can help clients create meaning from their everyday occupations (Ulfseth et al., 2015).
The literature supports the incorporation of self-analyses of occupational patterns to facilitate positive behavioral change in occupational therapy (Atler, 2015; Erlandsson, 2013; Jackson et al., 1998); however, a gap in the literature exists regarding how the use of structured reflective processes as an intervention in psychiatry affects the recovery of adults living with SMI. The purpose of this study was to explore how engaging in structured occupational reflection on an inpatient psychiatric unit can be used as an intervention to support the recovery of adults living with SMI.
Method
Design
We adopted a phenomenological qualitative design using semistructured interviews to explore how reflecting on the subjective experience of participation in daily occupations on an inpatient psychiatric unit affects experiences of recovery for patients on the unit (Figure 1). Occupational reflection was provided as a stand-alone occupational therapy intervention. To systematize the process of occupational reflection, we administered the Occupational Experience Profile (OEP; Atler & Berg, 2018). The OEP is a time-use diary that uses a 6-point scale to capture respondents’ subjective experiences of pleasure, productivity, restoration, and connection in relation to their participation in occupations over 24 hr (Atler & Berg, 2018). The OEP also records the duration, category (e.g., caring for self, socializing, meeting obligations), sociality (e.g., with others or alone), and location (e.g., home or away, indoors or outdoors) of each identified occupation.
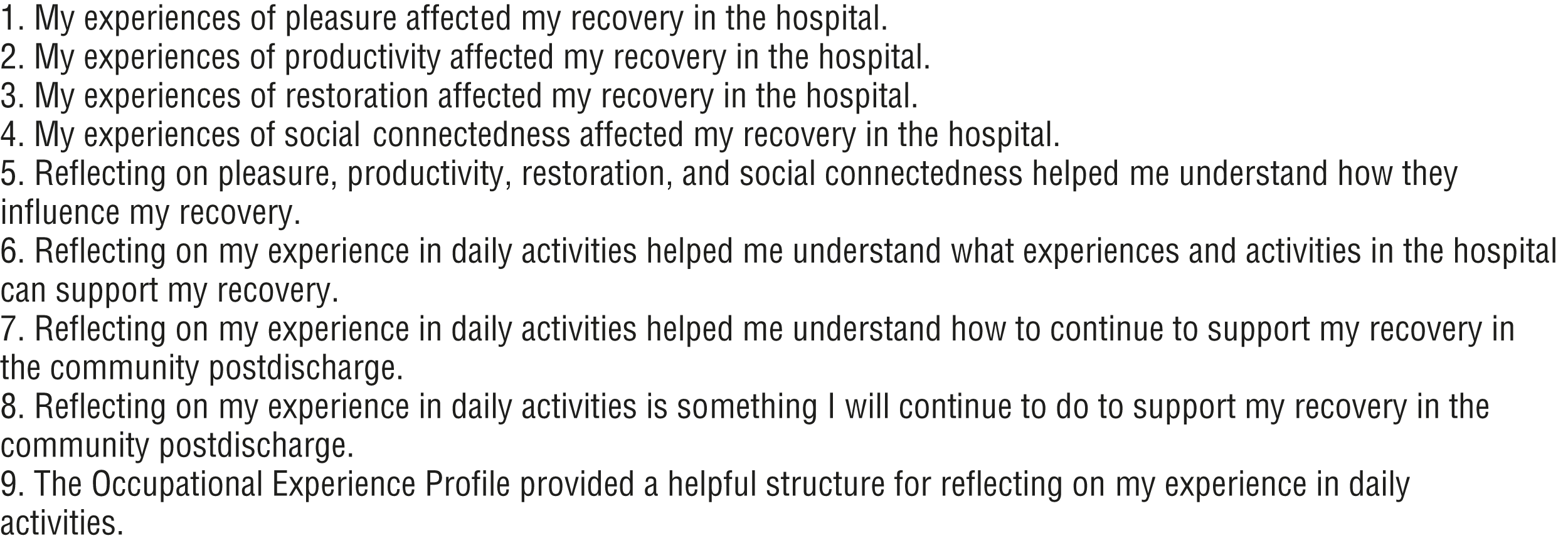
Semistructured interview prompts.
Data from the OEP itself were not analyzed for the purposes of this study. Study aims were met through analyses of semistructured interviews. We obtained ethical approval through the University of North Carolina at Chapel Hill institutional review board (19-0629) to conduct study procedures on the Crisis Stabilization Unit at the University of North Carolina at Chapel Hill Medical Center.
Participants
Recruitment and data collection were conducted by the second author, Zachary Shafer, an occupational therapist who performs routine occupational therapy interventions on the Crisis Stabilization Unit. Through purposive sampling, study participants were recruited from the caseload of other occupational therapists on the unit. Participants were required to be between ages 18 and 65 yr and fluent in English. Exclusion criteria were a diagnosis of cognitive disability, acute psychosis, pregnancy, or precautions other than standard psychiatric safety precautions. Treatment teams were also consulted regarding whether it was clinically appropriate for eligible participants to enroll in the study.
Data Collection
For each participant, study data consisted of responses to a semistructured interview. After obtaining informed consent, the second author trained participants in using the OEP and subsequently completed the tool with participants to reflect on their previous 24 hr (i.e., yesterday format) of participation on the inpatient unit. Together, the second author and participants interpreted the OEP results with fidelity to the user manual. Within a 3-day period, participants engaged in occupational reflection for a second time through completion of another OEP, and they were given the option to complete the tool independently or with the second author. Per the OEP manual, the tool can be administered as a self-report or in a yesterday interview format.
In accordance with the manual, participants requiring assistance were supported through the use of verbal and visual cuing to engage in the yesterday interview format. After completing the second OEP, participants met with the second author to interpret results collaboratively. Participants then scheduled a semistructured interview with the second author to assess how engaging in occupational reflection affected their experiences of recovery while on the unit.
Analysis
Interview transcripts were analyzed independently by each of the three authors using open coding. After the initial round of coding, all the authors met to compare and discuss their independent codings to achieve consensus. Subsequently, each author independently engaged in a second round of analyses to collapse codes into broader thematic units. The research team met again to compare and discuss their thematic units to achieve consensus and develop the themes that constitute the findings described in the Results section. No disagreements occurred regarding the codes or the resulting thematic findings.
Results
A total of 10 participants were recruited (6 men and 4 women). The mean age was 38 yr. Participant diagnoses were bipolar disorder (n = 5), major depressive disorder (n = 3), unspecified depressive disorder (n = 1), and substance-induced mood disorder (n = 1). Thematic analyses yielded the following three themes: (1) occupational reflection promotes insight into and awareness of how occupations affect mental health, (2) occupational reflection encourages positive reframing of occupational experience, and (3) occupational reflection facilitates identification of strategies to support recovery and meaningful participation after discharge.
Insight Into and Awareness of How Occupations Affect Mental Health
Study participants reported that engaging in occupational reflection enabled them to understand how their participation in specific occupations affected their subjective experiences of their stay on the inpatient unit and associated mental health. Users noted that the tool helped them clarify their interests and how they wanted to spend time in the future. For participants, the process clarified which occupations were experienced positively versus those that were experienced negatively, providing valuable information to maximize positive experiences.
Participants were unaccustomed to taking the time to reflect on their experiences: “I can say that I really never thought about what I was doing and how it affected me and just kind of went along with what was going on” (Participant 2). Engaging in structured occupational reflection encouraged participants to analyze themselves and their situation and to consider how their everyday doings affected their quality of life:
Reflecting on things like this, it helps you understand yourself, understand others, understand everything that’s going on around you so you learn your surroundings a lot better. And really you understand what makes you feel good, what makes you feel bad, what makes you feel kind of renewed and more energized, and what drains you. (Participant 5)
By understanding the relationship between their everyday occupations and mental health, participants were more aware of how to harness those relationships to effect positive change, “because I feel like when I’m doing something, I feel like I’m in a better mood” (Participant 10).
Participants also reported that engaging in a structured reflection regarding their experiences enabled them to discover that they enjoyed and benefited from some occupations to a greater extent than previously believed. For example, several study participants realized that social occupations had a positive impact:
It gives you an insight into . . . where you really need to be. Like with me, when I’m with people, I’m a lot better, I feel a lot better, I had more pleasure. But when I’m by myself, I don’t have pleasure. I don’t enjoy life or enjoy things. (Participant 8)
In addition to becoming more aware of their social needs, participants also reported becoming more aware of their surroundings and the needs of others in their social environment: “It’ll make you stop and think about what you did, how it affected you, how it could affect others, and it made me realize that being social is actually a good thing” (Participant 3). Acknowledging the importance of social experiences in their everyday occupations also encouraged participants to reflect on the benefits of social participation while on the inpatient unit: “I mean, having social connectedness is very helpful. And being around others, not necessarily in the same situation, but y’all have a same something in common, is very helpful. You realize you’re not there by yourself” (Participant 3).
The opportunity to reflect on occupational experiences raised awareness regarding the therapeutic benefits of the unit’s social milieu. For Participant 3, the OEP was a prompt for him to situate his experiences among his peers to recognize that he was not alone and that others shared his challenges.
All participants recognized the value of understanding the relationship of their occupational participation to health and well-being so that they could make positive changes in their lives. They also acknowledged the importance of having a structured method to guide their analysis to evoke those understandings:
Because if I don’t really talk about it, or see it myself, then it might not be brought up. And if it’s not brought up, I don’t see what’s making my day good, what’s making my day bad. I could probably get back to using drugs because I won’t see it. I’ll be kind of blinded and just kind of caught up in the everyday. (Participant 1)
Indeed, participants recognized that they would not engage in reflections without a systematic method for analyzing their participation. Engaging in systematic occupational reflection created the necessary temporal structure for participants to think and be proactive regarding how to care for themselves:
It was an eye-opening experience to reflect on my day . . . because it seems like I was losing time in here not thinking about what I was doing. The day would go by just so quick, and I couldn’t remember what I did or what I didn’t do. So, I think it was very good that I reviewed my day in general. (Participant 8)
In addition to highlighting the relationship between occupations and mental health, reflecting on occupational participation in a structured milieu setting provided insight regarding the importance of occupational routines. Before taking the OEP, participants were not reflecting on their routines or the routine structure of the inpatient unit. Consequently, they were not aware of the importance of routine and how it could affect their daily well-being. For Participant 6, this revelation was significant: “I didn’t realize that before, but it [a structured routine] is quite important.” Engaging in occupational reflection while on the inpatient unit also provided participants with the opportunity to craft new routines that targeted positive mental health: “I’m starting to figure out a good routine while I’m in here that’s healthy for me” (Participant 9).
After this revelation, all 10 participants indicated that they wanted to continue regular reflections on their routine after discharge to further consider how they could adjust their daily patterns to promote their recovery in the community. One participant requested a copy of the OEP, and another discussed creating a chart to keep track of similar data. Reflecting on their occupations across time allowed participants to step back and consider the “big picture” (Participant 6) to imagine new ways of doing and being.
Positive Reframing of Occupational Experience
Engaging in a structured reflective process prompted participants to reevaluate their occupational experiences on the inpatient unit, including the values they placed on different forms of occupation. For example, Participant 9 came to the realization that he could reframe restorative and restful occupations as productive occupations for recovery:
The first day, I had a lot of “read—take a nap—read—take a nap,” and I felt almost bad about that. Like I’m just sitting around. I’m not being productive. But . . . I had a different take on that the second day . . . I went ahead and put 5 for productive on that because I just had a different view of it. Like it’s actually productive for me to rest because I need rest, and it’s okay to take time out and chill.
Adding nuance to their understandings of occupation, participants discovered that their occupational experiences were multidimensional and could be simultaneously restorative and productive. Other participants found that pleasure could be experienced through productive occupations and not just occupations that are typically considered as leisure. Occupational reflection challenged participants’ assumptions regarding how they experienced their occupations and provided them with concrete data regarding the benefits and detriments of their everyday participation. For example, some participants noticed that social participation was renewing and beneficial despite often experiencing it as draining or anxiety provoking. Participants reported that reflecting on the subjective benefits they experienced during social participation encouraged them to reevaluate their social occupations in a positive manner and to understand them as an important factor in their health and well-being. This discovery would have been unlikely through psychoeducation alone.
Occupational reflection allowed participants to engage in a more granular and informative evaluation of their participation than was previously possible. For example, before using the OEP to analyze his occupations, one participant admitted, “I would probably say ‘I had a good day or bad day.’ Probably nothing about pleasure, productivity, restoration, or social connectedness. It’d probably just be ‘good or bad’” (Participant 3). Occupational reflection enabled participants to be more attuned to the multidimensional impact of their occupations on their mental health, which enabled them to discover positive experiences among events that were initially viewed as negative. Occupational reflection also guided participants in focusing on aspects of their daily occupations that were pleasurable despite being unaccustomed to thinking about pleasurable experiences in their lives: “Reflecting on the pleasure was nice because there’s not been a lot of pleasure in my life in the past 3 years” (Participant 8).
Systematically focusing on daily occurrences of pleasure can help clients of occupational therapy reframe their daily experiences to identify positive contributions to their mental health and recovery. The opportunity to reframe occupational experiences was enlightening to participants and also altered their perception of the interventions that they encountered on the inpatient unit:
I got to look back on what actually made me happy, what actually brought me joy, or what about it aggravated me. Like . . . the one today with the schedule [occupational therapy group intervention]. It was a great class but any other time I would have walked out there and been like, “that was a crappy class” and probably said something like “[Occupational therapy] sucks” and threw the papers away. Where at this point, because I did it [the OEP] and put it on the paper and I looked back at it, it was like, “Okay, it was a really good class.” I was just feeling some kind of way because my scheduling was off. Because I was disappointed in myself. (Participant 4)
With reflection and distance from their immediate occupational experiences, OEP users saw progress and hope for a changed future. Rating experiences of pleasure along a graded continuum (i.e., 1 = strong sense of displeasure; 6 = strong sense of pleasure) encouraged users to see value in mundane, everyday activities such as resting, showering, and brushing one’s teeth. In this way, the OEP propelled a shift from focusing on one’s overall negative experience of living with mental illness to focusing on positive aspects of everyday occupational participation. Many participants reported that the reflection process also helped them reframe their hospital stay to understand it as an experience that included participation in a community of peers with a shared experience of mental illness, thereby contributing to decreased self-stigma and sense of isolation.
The ability to reevaluate and reframe past experiences had a powerful impact on participants and empowered them to take control of their recovery and well-being: “If I can make myself enjoy some things, then I can make myself be able to deal with the things that are wrong with me” (Participant 10). Reflecting on how mundane, everyday occupations could bring pleasure was a powerful lesson in teaching participants how to manage their mental health through everyday occupational participation while on the inpatient unit:
If that’s bringing me joy without medication, then what am I complaining about, you know? If I could find joy in brushing my teeth or making a salad, or eating a salad, then do I really need those strong antidepressants? (Participant 4)
Indeed, the OEP inspired participants to leverage their occupations to stimulate positive mental health and well-being. This endeavor prompted participants to enact changes while in the hospital and also highlighted lessons they could implement in the community.
Identification of Strategies to Support Recovery and Meaningful Participation After Discharge
Having discovered the power of their occupations in relation to their mental health, participants were then able to identify changes they could make to their occupational participation to enhance their recovery after discharge. Participants who discovered that social occupations had a positive impact on their well-being by inducing positive subjective states were encouraged to seek social experiences after discharge. Although these participants would likely benefit from therapeutic interventions in the community to facilitate this process, their recognition of the importance of social participation was an important step in effecting a change in the level of their social participation. Moreover, these participants also recognized that the hospital was a safe place for them to begin experimenting with increasing their social interactions.
By systematically relating leisure activities on the inpatient unit to positive or negative subjective experiences, some participants were able to identify new occupational interests and new patterns of engagement. For Participant 2, this change consisted of realizing the difference between what others wanted her to do and what she wanted to do for her well-being. For Participant 5, reflecting on her interests was about “learning how to be by myself and enjoy my own company”—a potentially powerful tool in improving resilience in community living.
For most participants, engaging in the reflective process helped them understand what they needed to do to enhance their recovery and manage their mental illness. For example, Participant 10 reported that analyzing her patterns of engagement before and during a panic attack enabled her to achieve a deeper understanding of how she experienced her panic attack and, most important, to assess how effective her coping strategies were in managing the attack. Such insight would not have occurred without occupational reflection.
Without analyzing the occupational context of her panic attack, Participant 10 may not have been able to learn from her lived experience as she reportedly did by using the OEP. As a result of her occupational reflection, Participant 10 left the inpatient unit with a greater understanding of how to manage her anxiety. All participants recognized the value of using the OEP and indicated that they wanted to continue regular occupational reflections after discharge. Developing habits of occupational reflection in the community could be an important tool in facilitating long-term recovery.
Discussion
Findings from this study support incorporating occupational reflection regarding one’s subjective experiences during everyday occupational participation as standard practice for occupational therapy practitioners in inpatient psychiatry. Participants in this study reported several benefits from engaging in reflective processes as a part of their occupational therapy treatment: They acquired an understanding of themselves as occupational beings, discovered a relationship between their participation in occupation and their subjective mental states, identified occupations that supported positive and negative mental states, discovered the importance of social occupations, and recognized the importance of healthy structured routines. With these understandings, participants were able to begin to problem solve and implement changes in their occupational patterns to support their recovery. Ultimately, participants were able to reframe their inpatient experience in more positive terms while recognizing the lessons they had learned that could be used to support their mental health and recovery in the community.
The power of occupational therapy lies in its use of occupation-centered and occupation-based practices to support meaningful participation (American Occupational Therapy Association, 2016). We believe that best practice in occupational therapy deploys occupation as a means and ends in therapy and that such practices are critical to effecting meaningful real-world change. The findings of this study support using structured reflective processes, such as the OEP, as an occupational therapy intervention to guide clients in evaluating the impact of their occupational participation on their well-being. Engaging in a cognitive appraisal of one’s daily engagement in occupations, including shifts in participation as a result of intervention, could facilitate meaningful gains in occupational therapy in mental health settings by raising clients’ awareness of how their participation in occupations can be leveraged to enhance their recovery and well-being.
Although this study explored the impact of using occupational reflection as an intervention on an inpatient psychiatric unit, we believe that incorporating such reflective practices in community-based mental health interventions would also be beneficial. Community-dwelling adults living with SMI would likely benefit from a structured analysis of how their routine participation in occupations affects their recovery and well-being. Identifying which occupations engender positive experiences and those that do not is a critical first step to develop insight regarding how to establish daily habits and routines that have a salubrious impact on recovery.
This study supports the tradition in occupational therapy of facilitating occupational reflection among clients (Atler, 2015; Jackson et al., 1998). Studies have previously demonstrated the utility of incorporating self-analyses of occupational patterns to facilitate positive behavior change (Atler, 2015; Erlandsson, 2013; Jackson et al., 1998; Ulfseth et al., 2015). This study demonstrates that structured occupational reflection is a useful intervention for occupational therapy to support the recovery of clients in inpatient psychiatry. We believe this study contributes to a growing body of research that supports the standard adoption of occupational reflection interventions in mental health settings. Systematically raising clients’ awareness of how their habits, routines, and lifestyle contribute to their health is an important step in the client–therapist partnership to help collaboratively identify meaningful steps toward recovery (American Occupational Therapy Association, 2016).
Strengths and Limitations
Our sample size of 10 participants was sufficient to lead to data saturation (i.e., no new information or themes were emerging from the data). However, because the sample was not representative of the greater population, results cannot be generalized. Moreover, this small-scale study relied on participant self-report to assess the impact of the occupational reflection intervention on recovery. Future research should recruit a larger sample and use standardized assessments to measure the impact of the intervention on recovery.
Another limitation of this study is that both the occupational reflection intervention and the follow-up interviews were conducted by the second author. It is possible that participants would be more candid with their assessment of the intervention had another researcher conducted the follow-up interview. Although our study did not triangulate findings with other sources of data, we enhanced the credibility of our analyses by engaging in independent full coding of all transcripts by three separate researchers followed by group meetings to achieve a consensus among the research team.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Engaging in structured reflection regarding one’s subjective experiences of occupation while on an inpatient psychiatric unit can serve as a powerful occupational therapy intervention.
Engaging clients in a structured occupational reflection raises their awareness of the impact of occupation on mental health and empowers clients to independently manage their mental health through their occupational participation.
Reflecting on daily experiences while on an inpatient unit helps clients reinforce lessons they have learned for enhancing their recovery and well-being while hospitalized. Highlighting these lessons through structured reflections facilitates understanding of how to incorporate them into community living after discharge.
Conclusion
Engaging in structured occupational reflection can enhance the recovery of adults living with SMI in inpatient psychiatric units. Study participants who engaged in a structured occupational reflection intervention using the OEP reported that the intervention promoted insight into and awareness of how their occupations affect their mental health, encouraged positive reframing of occupational experience, and facilitated identification of strategies to support recovery and meaningful participation after discharge. Study findings support integrating structured occupational reflection as a routine intervention for occupational therapy practitioners in psychiatry.