
Abstract
Findings suggest that multimodal mental practice increases affected arm function in stroke survivors more than mental practice only.
Most stroke survivors exhibit residual motor impairments (Cioncoloni et al., 2013; Lai et al., 2002 ; Mayo et al., 2002), and stroke survivor prevalence is increasing (Carandang et al., 2006; Virani et al., 2020), yielding a burgeoning number of survivors exhibiting motor impairments. Several interventions target upper extremity (UE) hemiparesis (e.g., Laver et al., 2015; Volpe et al., 2008; Wolf et al., 2006). However, many require extensive contact time (e.g., Wolf et al., 2006) and specialized equipment (Laver et al., 2015; Volpe et al., 2008), undermining their widespread adoption.
Both mental practice (MP) and action observation (AO) incorporate repeated cognitive rehearsal of paretic UE movements in the absence of physical movement attempts. Additionally, both techniques elicit brain activity comparable to the actual performance of the targeted task (Decety, 1996; Sale & Franceschini, 2012) and have shown promise in increasing paretic UE use and function (Franceschini et al., 2012; Page et al., 2007). Both MP and AO are portable and inexpensive; moreover, they require minimal training, equipment, and supervision. Thus, they constitute a practical alternative to interventions such as constraint-induced movement therapy (CIMT), robotics, and contemporary virtual reality (VR) approaches (e.g., Laver et al., 2015; Volpe et al., 2008; Wolf et al., 2006).
In addition to these merits, AO combined with MP produces larger corticomotor changes than when either technique is administered singularly (Nedelko et al., 2012). This finding—and the singular, high efficacy of each approach—led us to hypothesize that combining RTP with AO and a previously validated MP regimen would be more efficacious in reducing paretic UE functional limitation (the primary outcome) than the current standard of UE care: repetitive task practice (RTP; Jette et al., 2005; Latham et al., 2006). To test this hypothesis and to estimate treatment effects for a larger trial, we compared the effect of a regimen combining AO, RTP, and MP (hereafter termed multimodal mental practice [MMMP]) with the effects of an RTP-only regimen on paretic UE functional limitation (our primary study outcome). To our knowledge, this study was the first to examine the efficacy of this combined regimen and the first to compare the relative efficacy of this approach with a time-matched, standard UE rehabilitation regimen.
Method
Study Design and Participants
We performed a secondary analysis of data obtained from two MP efficacy trials approved by the local ethics board (Page et al., 2011; unpublished data). We recruited volunteers for both studies using approved study pamphlets distributed at local outpatient clinics, referrals from local clinicians, and presentations at local stroke support groups.
All participants met the following study criteria: (1) 10° of active flexion in the paretic wrist and two digits in the more affected hand; (2) one stroke, experienced >3 mo before study enrollment (>3 mo post ictus constitutes the typical period when endogenous recovery slows or ceases); (3) a score ≥24 on the Mini-Mental State Examination (Folstein et al., 1975); (4) age ≥18 yr but ≤75 yr; and (5) discharged from all forms of physical rehabilitation, including participation in other studies. Exclusion criteria included (1) excessive spasticity in the paretic UE, defined as a score of ≥2 in the paretic elbow, wrist, or fingers as determined by the Modified Ashworth Spasticity Scale (Bohannon & Smith, 1987); (2) pain in the paretic UE, as measured by a score of ≥4 on a 10-point visual analog scale; and (3) history of a parietal stroke, as identified in the medical record of each study volunteer. The third criterion was used because some literature suggests that strokes occurring in the parietal areas may diminish ability to visualize motor tasks. All criteria were initially reported by the participant and were adjudicated by the participant’s medical record.
Outcome Measures
One week after we obtained consent using approved forms and screening, we administered the following three measures to all participants: the Action Research Arm Test (ARAT; Lyle, 1981), the UE section of the Fugl-Meyer Scale (FM; Fugl-Meyer et al., 1975), and the Hand subscale of the Stroke Impact Scale (SIS; Version 3.0; Vellone et al., 2015). All of these measures have been extensively validated in the population with chronic stroke (Hsieh et al., 2009; van der Lee et al., 2001; Vellone et al., 2015).
Action Research Arm Test
The ARAT contains 19 items that quantify paretic UE grasp, grip, pinch, and gross movements on a 4-point ordinal scale (0 = can perform no part of the test; 3 = performs test normally), for a total possible score of 57.
Upper Extremity Section of the Fugl-Meyer Scale
The UE section of the FM discerns paretic UE impairment and has a total possible score of 66 points. Participants attempt movements at each paretic UE joint, requiring performances increasingly outside of synergy.
Hand Subscale of the Stroke Impact Scale
The Hand subscale of the SIS measures quality of participation of the paretic UE in community-based activities. Scoring of the subscale is described in Duncan et al., 1999.
Randomization and Intervention
Using a computer-generated random numbers table, we assigned a group of participants to receive RTP only. Separately, a second group was assigned a regimen comprising MP+RTP. From this MP+RTP group, we conducted a second randomization; the resulting subgroup was administered MP+RTP, supplemented by AO (i.e., MMMP). The current secondary analysis was situated to compare the changes exhibited by participants administered MMMP with changes exhibited by participants administered RTP only, given our aforementioned hypothesis.
Participants assigned to the RTP-only group participated in 1:1, 45-min UE training sessions occurring 3 weekdays per week for 10 wk. As described by Page and Peters (2014), participants physically practiced five common bilateral and unilateral UE activities, with tasks graded according to participants’ abilities and progress. No other concurrent intervention was provided or permitted. All therapies were administered on a 1:1 basis by a dedicated occupational therapist in a dedicated outpatient therapy space.
The time-matched MMMP regimen consisted of AO, RTP, and MP. The 15-min AO sessions were administered first; under close supervision of the treating therapist, participants watched footage of the same five UE activities the RTP-only group performed. The therapist asked participants to carefully observe the video in preparation for carrying out one of the featured movements during RTP. The video depicted a person without stroke performing the particular task of interest, from multiple angles.
Directly after RTP, participants took part in 15-min, audio-recorded MP sessions, structured in the same fashion in our previously validated MP programs (Page et al., 2011; unpublished data). The opening minutes consisted of relaxation; the audio recording asked participants to imagine themselves in a relaxing environment and to perform contraction and relaxation of all muscles. After the relaxation exercise, the audio recording provided suggestions for internal, cognitive polysensory images (Paivio, 1985) related to using the UE during the task participants had just performed during RTP and had previously observed during AO.
The audio file concluded with refocusing participants into the room.
Posttesting
One week after the intervention period had concluded, all measures were again administered by the same rater used at baseline. The rater was blinded to the group to which participants were randomized.
Results
Participant Demographic Characteristics
Using t tests for continuous variables and χ2 tests for dichotomous variables, we found that participant attributes (age, time post stroke, sex; baseline scores on the ARAT, FM, and SIS) did not significantly differ between groups at baseline. The 18 participants who were analyzed completed their assigned interventions with no concerns or adverse events; their demographic characteristics are shown in Table 1, and the study flow chart is shown in Figure 1.
Participant Demographic Characteristics
Note. MMMP = multimodal mental practice; RTP = repetitive task practice.
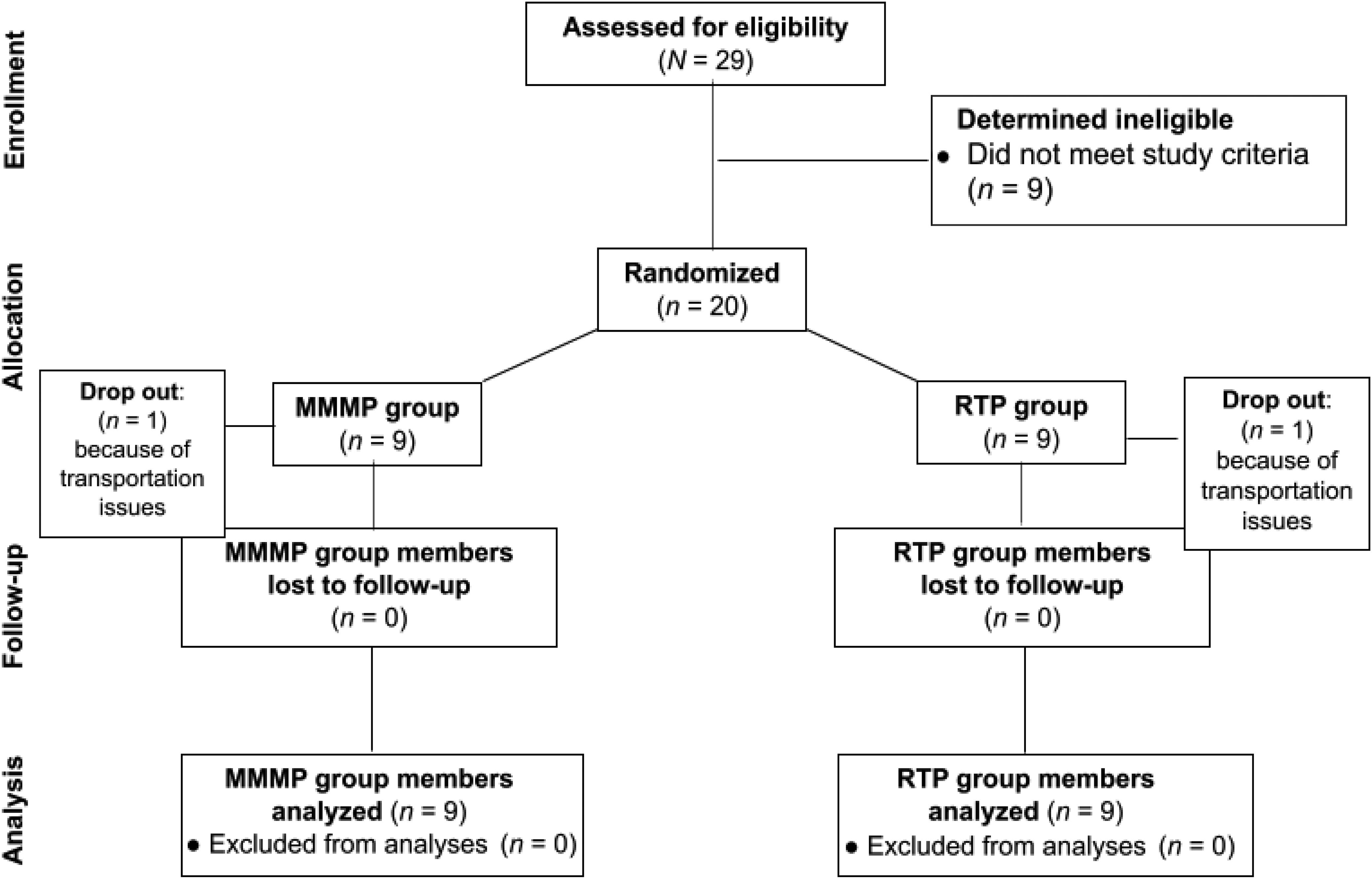
Flow of participants through the study.
Functional Outcomes
Given the heterogeneity of the population with stroke, the relatively small sample size, and the fact that the two groups were independent, a Mann–Whitney U test was conducted for each outcome measure to compare the magnitude of change between groups. As can be seen in Table 2, the magnitude of change was decidedly larger on all three measures for the MMMP group compared with the RTP group, yielding significance at the p < .01 level for the ARAT (Mann–Whitney U = 13; n 1 = 9, n 2 = 9; p < .01, two tailed), FM (Mann–Whitney U = 16; n 1 = 9, n 2 = 9; p < .05, two tailed), and SIS (Mann–Whitney U = 9; n 1 = 9, n 2 = 9; p < .05, two tailed). Effect sizes were medium (ARAT, r = .56; FM, r = .50; SIS, r = .65) when we used effect size calculation methods recommended for non–normally distributed samples (Fritz et al., 2012).
Functional Outcomes
Note. ARAT = Action Research Arm Test; MMMP = multimodal mental practice; RTP = repetitive task practice; SIS = Stroke Impact Scale; UEFM = Upper Extremity section of the Fugl-Meyer Scale.
Discussion
This study, a preparation for a larger trial, was a pilot test of the central hypothesis that combining AO, RTP, and MP would yield larger reductions in paretic UE functional limitation than a time-matched RTP-only regimen. Although the groups were closely matched on demographics and preintervention ARAT scores, participants who received MMMP exhibited substantially larger ARAT score changes, indicative of larger functional limitation reductions. These changes attained statistical significance, confirming our primary study hypothesis. Moreover, these findings were corroborated by significantly larger score increases in favor of the MMMP group on both the FM (indicative of larger UE impairment reductions) and SIS (indicative of greater participation in community-based activities). In sum, although it occupies the same amount of time as RTP, it appears that MMMP may be preferable to optimize motor outcomes, as evidenced by the consistently larger magnitude of score changes among participants administered this regimen.
The minimal clinically important difference (MCID) for the ARAT in stroke patients is 5.7 points (van der Lee et al., 2001), whereas the lead author and colleagues established the MCID for the FM as 4.25–7.25 points (Page et al., 2012). Finally, the MCID for the SIS Hand subscale is 17.8 points. At least in this pilot work, score changes exhibited by participants administered MMMP far exceeded all of these values. This finding suggests not only that MMMP is more efficacious than the current gold standard of UE therapy but, importantly, that the score changes associated with MMMP are sufficient to produce changes enabling patients to resume valued activities. Obviously, the efficacy of this approach requires further investigation with a larger, more diverse sample to confirm the magnitude and clinical significance of changes reported here.
Both AO and MP are hypothesized to have similar mechanisms of action. Briefly, when goal-directed, physical practice attempts are observed (i.e., AO) or mentally rehearsed (i.e., MP), neurological and muscular responses are generated that are similar to those that occur when the targeted movement is actually being executed. Accordingly, one would expect that these regimens could provide substantially more practice repetitions than a therapist-guided RTP session because (1) patients are not hindered by their physical impairments when mentally rehearsing tasks; (2) physical fatigue is not a concern with these cognitive-based interventions; and (3) both MP and AO require minimal warm-up, rest breaks, modalities, or change of physical environment and equipment. These factors mean that MMMP could conceivably afford more practice attempts than RTP, contributing to greater functional restitution. In future studies, researchers may wish to confirm this hypothesis by quantifying MMMP and RTP practice attempts during a fixed time duration.
The interventions in this study were duration matched with one another and were administered to medically stable participants with chronic symptoms, meaning that endogenous recovery was unlikely. Given these factors, it seems unlikely that the effects we observed were because of chance. Moreover, MMMP can be feasibly applied with minimal resources. Indeed, our study clinicians needed only (1) brief training to understand the principles of AO, RTP, and MP and (2) audio and video recordings created with software available on most computers (audio files) and tablets (video files). Additionally, MMMP session durations were 45 min, with 15 min dedicated to each component (i.e., AO, RTP, MP). This duration is feasible in outpatient clinical settings without exceeding typical reimbursement patterns. In contrast, CIMT, robotics, and VR interventions targeting the paretic UE are time and resource intensive, and they are not regularly reimbursed by insurance.
Study Limitations and Suggestions for Future Research
Although study conditions were well controlled, several limitations should be noted. First, as with any pilot study, the number of participants was purposefully low. As noted earlier, this understandable limitation should be mitigated in future studies enrolling larger and more diverse samples. Larger studies will also address a common case series limitation: that our results are only associated with the MMMP group and cannot yet be entirely attributed to MMMP participation.
This study was situated to pilot test the hypothesis that combining AO and MP with RTP renders a larger treatment effect than time-matched RTP alone. Many other examples can be found in which multicomponent regimens were compared with single-component, standard-of-care regimens of similar durations. The common goal of such comparisons (including the current study) is to ascertain the most efficacious intervention. Indeed, if finite resources can be applied more effectively using a multicomponent intervention than the current standard, then this undertaking is reasonable. That said, this study did not ascertain the relative added value of either AO or MP, and it was underpowered to do so. Such efforts will be undertaken in future studies as the intervention is refined and the relative value of its components are better understood. Additionally, the possible influence of sex on MMMP response should also be examined.
Although MMMP appears to be just as feasible to implement in the clinic as RTP, future research is needed to examine barriers and facilitators to MMMP implementation in actual practice settings. Other implementation outcomes worth assessing in follow-up studies may include MMMP adoption, fidelity, appropriateness, acceptability, and sustainability.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: More MMMP research needs to be performed to confirm the effects we observed. However, the firm scientific premises of MMMP, the current study results, and the ease with which MMMP can be clinically integrated certainly make it a promising approach that may reduce paretic UE impairment and increase UE function. If practitioners choose to implement MMMP, they should document treatment content, client responses to the treatment, and changes in client function.
Conclusion
Data from this study suggest that a multicomponent regimen composed of AO, MP, and RTP is significantly more efficacious than RTP only. Moreover, changes associated with MMMP participation were clinically significant. Easy-to-implement, inexpensive interventions that require the same contact time as the current gold standard but are more efficacious and use fewer human resources certainly deserve further study.