
Abstract
The findings provide insight into the need to assist clients in developing skills to recognize normalization of disability discrimination and strategies to access equitable health care.
A person’s ability to use health care services in the United States depends on the ability to navigate access barriers such as affordability, accommodation, availability, accessibility, and acceptability (Levesque et al., 2013). These barriers are well known and well documented in racial and ethnic communities (Gaston-Johansson et al., 2007), and they are linked to disparate health outcomes compared with people who identify as White (Phelan & Link, 2015). Barriers include the noted complexity and fragmentation of health plans along socioeconomic lines and distrust of providers (Nelson, 2002).
Literature supplies evidence that identifies people with physical disabilities (PWPDs) as a marginalized population susceptible to the same access barriers as other minority groups (Winters & Story, 2007). However, PWPDs face distinct and complex barriers that further inhibit access to care (Singer et al., 2017), including physical and process barriers that may go unnoticed by providers and those receiving care (Kroll et al., 2006; VanPuymbrouck, 2018).
Although physical entry barriers exist (Singer et al., 2017), the most difficult physical barriers to overcome are caused not by lack of access to health providers’ offices but by lack of access to medical diagnostic equipment, exam tables, and exam rooms (Winters & Story, 2007). Process barriers include providers’ lack of knowledge about working with PWPDs, preconceived assumptions about what kind of care and medical information PWPDs need, and unsafe transfer methods used during appointments by staff unfamiliar with working with PWPDs, which directly affect quality of care (Kroll et al., 2006). VanPuymbrouck et al. (2020) found that although the majority of providers self-reported not being biased against people with disabilities, the overwhelming majority of providers were implicitly negatively biased. The combined influence of providers’ limited knowledge and negative biases arguably contribute to disparities in health care access and health outcomes for PWPDs.
Rights to accommodations and equitable health care supported by the Americans With Disabilities Act of 1990 (Pub. L. 101-336) rely on the assumption that PWPDs will both recognize and self-advocate when disparate care is offered. PWPDs are routinely expected to request accommodations to receive care readily available to people without physical disability (Singer et al., 2017). However, PWPDs may not know whether accessible equipment is available, be knowledgeable about their rights, or know how to enforce those rights (Winters & Story, 2007). These experiences can be defined as normalization of disability discrimination (NODD) in health care. VanPuymbrouck (2018) found that NODD occurs when discriminatory policies, practices, protocols, and behaviors are acceptable and routine; they are the status quo. NODD is expected to occur and influences how people view their right to advocate for and access accommodations (VanPuymbrouck, 2018). As a result, PWPDs continue to experience inequitable access to health care.
Personal health literacy is “the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others” (Office of Disease Prevention and Health Promotion, 2020, The New Definitions section, para. 2); moreover, it is a critical component to success in performing health-related activities of daily living (American Occupational Therapy Association, 2020). To receive appropriate accommodations, a PWPD may need to develop a level of health literacy that exceeds that needed by a health consumer without disabilities. PWPDs must develop a unique set of health literacy skills that involves understanding objective information on health risks. These skills assist with both recognizing and addressing disparate care when it occurs as a precursor to initiating the receipt of accommodations, which may be the initial step to receiving equitable care.
Research examining the experiences of PWPDs with strong advocacy skills has found that they share the capacity to identify NODD and to implement common strategies for navigating barriers to health care access (e.g., VanPuymbrouck, 2018). These advocates use this knowledge—disability health literacy—to improve access to and receipt of equitable care. However, understanding is limited regarding whether or how disability health literacy is learned or how strategies develop among successful self-advocates. Given the gap in the current literature, in this study we aimed to explore whether PWPDs recognize disparate care when it occurs, how those experiences contribute to strategy and skill development to overcome barriers, and how this capability functions to inform advocacy behaviors in the context of health care.
Method
In this qualitative research study, we used the Social Model of Disability (Oliver, 1996) and a Critical Disability Theory lens to explore the perspectives of PWPDs on experiences of health care across three focus groups. The Social Model of Disability exposes socially constructed barriers to participation, such as NODD, and can inform the analysis of health care access for PWPDs (Oliver, 1996). Critical Disability Theory can be used to delve into issues of power and examine contexts of inequity based on disability (Pothier & Devlin, 2006).
Participant Selection and Recruitment
To recruit participants, we distributed a flyer, approved by the Rush University institutional review board, throughout a large medical center campus. To facilitate recruitment, we also used snowball sampling, asking enrolled participants to distribute the flyer to people they knew (Etikan & Bala, 2017). Twenty-four people contacted the primary researcher (Laura VanPuymbrouck) across a 6-mo period and were screened to determine their eligibility to participate in this study. To better generalize our findings to disability community members who may not be experienced in advocacy (Baldridge & Veiga, 2001), we excluded any person who belonged to a disability advocacy group or who responded “yes” to the following question: “Do you feel you have a strong knowledge of disability rights or the Americans With Disabilities Act?”
Inclusion criteria required that participants be age 18 yr or older and English speakers who identified as a PWPD in need of a mobility aid; they also had to have attended a primary health care visit in the past year. Four men and 6 women met the inclusion criteria. Table 1 outlines participants’ demographic characteristics. All participants provided informed consent before data collection and received $25 for their time and travel. This study was approved by the Rush University institutional review board.
Participant Demographic Characteristics (N = 10)
Grounded theory methods are used to describe poorly understood phenomena, examine relationships among data, and provide an opportunity for theory development when none exist (Glaser & Strauss, 2017). The dearth of knowledge on how disability health literacy is learned by PWPDs points to using grounded theory to better understand this process. During data collection and analysis, we used constant comparative methods of grounded theory in iterative cycles (Glaser & Strauss, 2017) to explore PWPDs’ experiences of seeking primary health care services and their perceptions of disparate care (Figure 1).
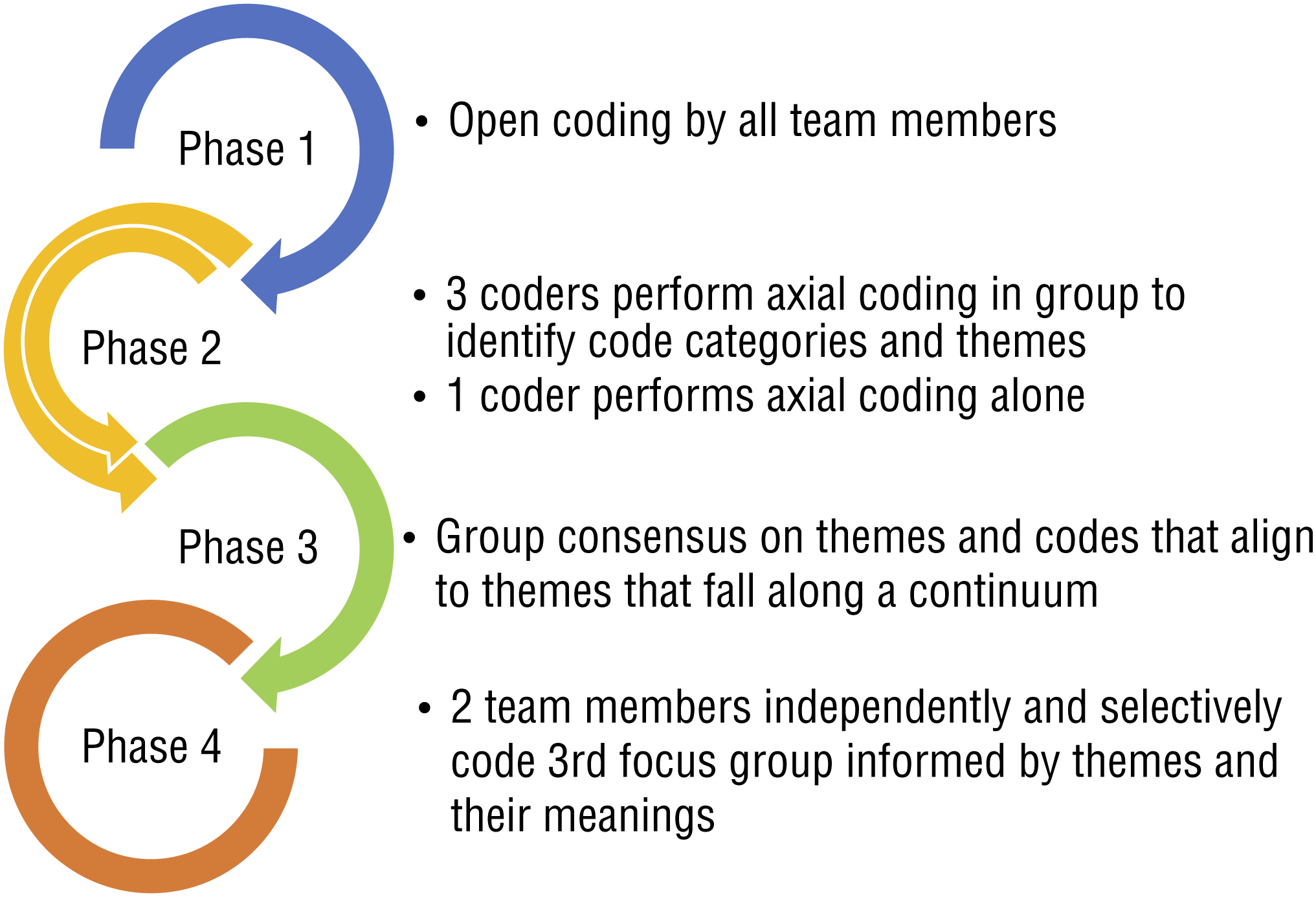
Phases of data analysis.
Reflexivity
The lead author of this article has an established record in qualitative research and functioned as both the principal investigator (PI) and the research advisor to students (the coauthors) as part of their doctorate of occupational therapy curriculum during this project. Throughout the research process, we used critical reflection to uphold the credibility of qualitative results and the emphasis on participants’ lived experience (Creswell & Creswell, 2017). As a team of three students and one faculty member in the field of occupational therapy, we acknowledge that our experiences in this field inform our thought processes and our interpretation of transcripts through coding. From the beginning of the project, we used field notes and audit trails of all decisions dealing with data collection and analysis and then examined them for the existence and influence of bias. In addition, we recognize that we represent nondisabled perspectives, although one team member identifies as having a chronic disease requiring frequent health care visits and potentially shares similar lived experiences with health care access barriers as those experienced by the study participants.
In the formation of our focus group question guide, we piloted questions with people from the disability community and included their recommendations for change. Also, in the process of combining codes into thematic groups, one member of the research team performed this task independently and compared their results with those identified by the other three team members in a group analysis. A different person performed this task for the coding of themes from Focus Groups 1 and 2. These processes increased the rigor of the resulting themes by working to reduce biases that may have been derived from group discussion (Creswell & Creswell, 2017).
Data Collection
Three semistructured focus groups were conducted at a large urban medical campus using a question guide informed by grounded theory methods (Glaser & Strauss, 2017). Researchers used an open-ended question guide consisting of four broad questions to seek information about the participants’ most recent primary care visits. For example, the first question was “Please describe a recent health care experience.” The questions prompted participants to describe their health care visits, how they interacted with the staff and providers, whether they had specific needs or requests, how they felt about the care they received, and how providers responded to requests. The focus group discussions were audio recorded, transcribed verbatim by members of the research team, and deidentified.
The interview location was chosen because it is the PI’s place of employment and is easily accessible by PWPDs. Participants were assigned to a group on the basis of their availability to attend one of the three prescheduled interviews. All focus group interviews were facilitated by the PI, lasted 1 hr, and included 3 to 4 participants.
Data Analysis
All members of the research team coded the transcripts from Focus Groups 1 and 2 using a grounded theory systematic design, including open, axial, and selective phases of coding (Creswell & Creswell, 2017; Figure 1). In the initial phase, we independently completed open coding using descriptive codes to identify phenomena, process codes to identify actions occurring, and in vivo codes to highlight direct comments from participants’ lived experiences.
The second phase of the analysis process included intensive group discussion of code meaning and group consensus to refine codes. We used constant comparison of code meanings in a process of axial coding, inductively working to reveal thematic groups and subgroups for all codes (Saldaña, 2016).
During the third phase of coding, we used a selective coding process to narrow code categories of emergent themes with corresponding subthemes (Creswell & Creswell, 2017), which revealed that participants’ experiences fell along a continuum of evolving stages for recognizing disparate care and strategies to overcome barriers. Final themes were defined by codes aligned to them using consensus agreement among group members. These themes were deductively informed by each team member’s a priori concepts of occupational therapy, health care access barriers of PWPDs, and health literacy.
In the final phase of coding, we then used these themes to ground independent analysis of the third focus group transcript by two team members, followed by a consensus meeting to confirm aligned themes to text.
Results
Seven thematic categories emerged in data analysis that represent a continuum of stages for recognizing health care as disparate and strategies for receiving equitable health care for PWPDs. These stages taken together are referred to as the physical disability health literacy continuum (PDHLC; Figure 2). The seven stages of the PDHLC are (1) unrecognized experiences of NODD, with a subtheme of medicalization; (2) knowing what you need; (3) noticing differences; (4) emerging understanding; (5) learning to take personal action; (6) NODD is systemic; and (7) taking control.
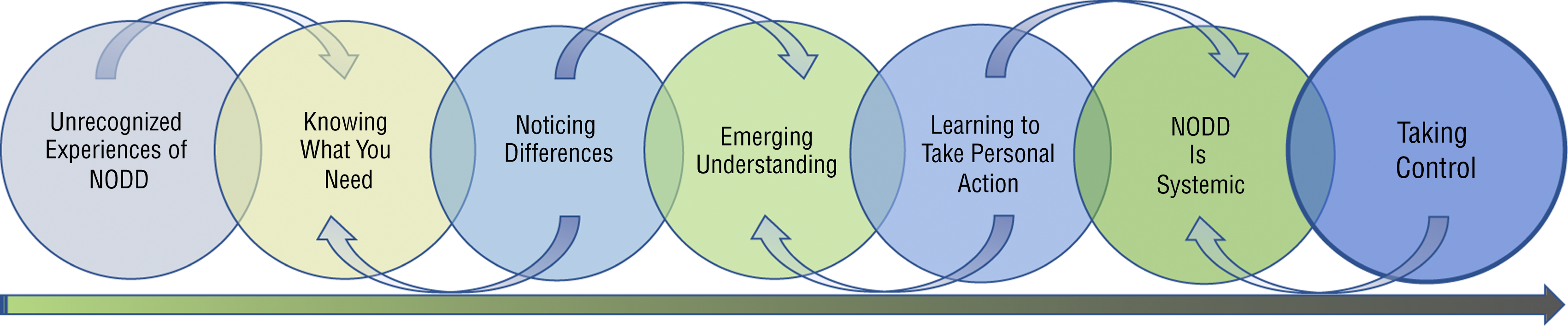
Evolution of self-advocacy.
Unrecognized Experiences of Normalization of Disability Discrimination
In Stage 1, participants’ descriptions of their health care experiences portray providers’ limited knowledge of disability rights, not recognizing acts of discrimination, and justifying acts of discrimination. Participants described experiences or interactions with providers, the system, or its policies as barriers to the care they need without attributing them to NODD. One participant epitomized this stage of the PDHLC. This participant recalled a recent visit to the dentist that illustrates the lack of recognition of discriminatory practices and internalizing an inaccessible environment as the PWPD’s responsibility to navigate on their own:
When I went to the dentist, they didn’t really have a way for me to get in the chair. I’m lucky that I can get in and out the wheelchair on my own, but like if I wasn’t prepared for it, what would have happened then? (Focus Group 2, Participant 1)
Another participant described a recent visit while justifying the inequitable care receipt: “I can’t get on the table, so she was doing the best of her ability” (Focus Group 2, Participant 3).
A subtheme that emerged from Stage 1 is the common occurrence of experiences of medicalization. We define this subtheme as a process in which health care providers and systems view disability through the lens of the medical model, leading to patient care focused solely on “fixing” the disabled body, being unable to see past a person’s disability, and treating disability as an illness rather than as a long-term social state (Oliver, 1996). These experiences were vocalized by multiple participants as a source of frustration but fell short of being aligned to discrimination or provider bias. “[Physical disability is] the first thing people see, and they stop right there, you know? I think with health care that’s a problem” (Focus Group 3, Participant 2). Another participant spoke about the conflicting agendas of doctors who focus more specifically on curing the disability:
[Other providers] were basically telling me, “Hey, besides you being in a wheelchair, you’re pretty much in perfect health” . . . but when I went to my doctor . . . he only worries about what’s wrong instead of what’s right. (Focus Group 2, Participant 1)
Knowing What You Need
The second stage of the PDHLC describes a process of transformative learning that PWPDs experience as they come to understand that there may be times when the care recommendations of providers conflict with their own lived knowledge of what works and what does not in managing their health. Knowing what you need includes learning to question medical authority and developing a sense of control over your own health care needs, possibly through trial and error. This stage goes beyond satisfaction with the receipt of basic health care to include expecting provider respect and treatment with dignity as well as rejecting NODD. Participants voiced their opinions on their individual needs and the needs of the disability community at large: “A disabled person needs to link up with a support group, you know . . . because other disabled individuals can tell you things that a doctor can’t” (Focus Group 2, Participant 3).
Noticing Differences
In the third stage, the PWPD starts to sense that something is different about the health care they receive compared with those without disabilities, going beyond the individual experience. This treatment includes describing how providers across experiences avoid answering questions about the PWPD’s health and perseverating on the disability. Participants described recognizing similar and repeated slights or microaggressions across providers and noticing differences in health care between institutions. In this stage, a PWPD may feel unsure about the quality of health care without naming it as inequitable. One participant described their realization that even a specialist might not understand health concerns of a PWPD: “I thought doctors knew everything at first. All doctors knew everything, but . . . they don’t know. They don’t know about disability” (Focus Group 3, Participant 4).
Beyond provider interactions, another participant recalled their experience at an accessible facility as something “special” versus an example of how all clinics should be: “The place for me to go and have my mammogram had a special [table] that lowered down . . . that was such a wonderful place . . . I just pushed a button and the doors opened” (Focus Group 3, Participant 4).
Although this participant described this facility as accessible, they simultaneously qualified this experience as unique in comparison with other health care visits. In addition, although this participant recognized this experience as different, they failed to equate times without accommodations as discrimination. Similar descriptions of noticing differences in care without claims of inequity were heard from multiple participants.
Emerging Understanding
In this fourth stage, a PWPD will begin to recognize differences in health care quality as a result of personal, inequitable experiences relating specifically to disability. For example, a PWPD would fall in this stage if they recognize that the level of care negatively affects their health outcomes, describe system barriers in health care relating to disability, or recognize that their health care needs are unique because of disability. In addition, they have emerging consciousness that inadequate care by individual providers is linked to a lack of understanding of disability across health care. A discussion between 2 participants illustrates this point of realization that differences in health care may be related to disability and wheelchair use: “Oh, you didn’t [get weighed]? They didn’t weigh you—the nurse? Wow!” (Focus Group 2, Participant 2). “Yeah, that is kind of weird. They didn’t weigh me . . . they just took my blood pressure” (Focus Group 2, Participant 1).
Another participant’s response to being asked what they look for in a provider illuminates a concern of many PWPDs, which is unfamiliar to a person without disability and unrecognized by people at early stages along the PDHLC:
Someone who is going to ask questions as if I wasn’t in a chair, but as a woman with questions that need to be answered. You know . . . [like] when was your last menstrual and all that kind of stuff. (Focus Group 3, Participant 2)
Learning to Take Personal Action
The fifth stage is defined by participants as recognizing the need to take proactive steps to avoid unsatisfying health care on the basis of past experience. This behavior may manifest as a PWPD researching ways to meet their own health care needs, seeking out information from others in the disability community, switching providers because of inequitable care, or knowing in advance to question providers related to care. One participant described how he circumvented limited provider time in which too much time was focused on disability instead of discussing primary health-related issues during appointments: “My friend [a PWPD] and I, we talk a lot and sometimes we make a list and then within that 5 or 7 minutes, you just plow through those questions [during the appointment]” (Focus Group 2, Participant 2).
Another participant talked about their experience of being newly diagnosed and realizing the need to take personal action to find resources and learn about their condition:
When I was diagnosed, I was lost, I couldn’t find where to go, what should I do, so what I did was go online and look up my medical condition, and found resources available. Then [I] reached out . . . now I know . . . but at the beginning, when you are first diagnosed you are lost. (Focus Group 2, Participant 4)
Critical to this narrative is the apparent failure of the provider to offer resources and support.
Normalization of Disability Discrimination Is Systemic
In the sixth stage, people synthesize experiences across contexts and providers, recognizing inequitable care as disability-based discrimination. They also realize this occurrence as a shared group experience versus an individual one. One participant described their knowledge that disability is a shared experience—one that is difficult for a person and potentially a provider without disability to understand:
Participant: You [provider] have to work within that culture . . . whether you’re Black, Muslim . . . you have a culture, and as a doctor, you have to respect that culture.
Interviewer: Do you all think that there’s a culture of disability?
Participant: Yes, I do.
Interviewer: And what is that?
Participant: It’s kind of hard to describe. Unless you’re disabled, you kind of won’t understand certain things that go on. (Focus Group 2, Participant 3)
This step might occur simultaneously with the seventh level of the continuum because learning to advocate for oneself may facilitate recognition of NODD. In this level, the person learns to be assertive when requesting the care they need, recognizes that differences in health care are a result of NODD rather than a result of personal characteristics, learns to navigate the barriers of NODD, and recognizes the need to advocate for equity in health care. One participant emphasized that experiences of discrimination are linked to group identity: “We get treated like third-class citizens, or they don’t care, you know?” (Focus Group 2, Participant 2).
Taking Control
The seventh and final stage of the PDHLC represents what we believe is the most informed stage of disability health literacy. A PWPD at this stage explicitly advocates for their rights to equitable care, often proactively, and understands how access rights apply to the context of health care and other settings. These people know they are the disability experts, and they educate providers on the needs of PWPDs, use peer supports to answer health-related questions, and encourage other PWPDs to do the same.
One participant communicated connecting with others in the disability community who aid her in learning about her health:
I learned that through socializing with other individuals . . . I tell individuals, particularly when they’re newly disabled, follow the doctor’s orders, but also link up with a group. You know—when you’re ready—because you find out different things. (Focus Group 2, Participant 3)
Two participants advocated for the training of health care providers to better accommodate PWPDs: “We have to advocate for ourselves, but in a hospital, we cannot be advocates . . . we need someone else to advocate for us” (Focus Group 2, Participant 3). “In medical school they need to have a course about the needs of people with disabilities” (Focus Group 2, Participant 2).
Across focus groups and between participants, we found a vast range of disability health literacy and discovered processes that a PWPD moves through in recognizing the need for accommodation. What also emerged is an understanding that although the PDHLC may be a linear progression, it may also be variable because each person has a unique set of experiences that may influence where they fall on the continuum. It may be that some PWPDs skip stages of the continuum, whereas others may be at multiple stages at one time.
Discussion
In this study, we explored whether PWPDs recognize disparate care when it occurs, how these experiences contribute to strategy and skill development to overcome barriers, and how this capability functions to inform advocacy behaviors in the context of health care. Taken together, the themes that emerged across participants’ experiences represent a continuum moving from limited awareness of NODD, to emerging recognition of inequities in care as a PWPD, to a raised consciousness that systemic barriers may in fact necessitate self-advocacy to access care that people without disability readily receive.
Routine and normalized experiences of limited access or disparate care (i.e., NODD) were heard in descriptions of participants’ experiences. However, these experiences were aligned to being not acts of discrimination but rather microinequities. Microinequities are defined as the “small, unjust inequalities . . . and while individual instances may seem trivial, their cumulative effects can account for differences in outcome” (Massachusetts Institute of Technology Committee on Women Faculty in the School of Science, 1999, as cited in Brennan, 2016, p. 237). Research exploring microinequities has emphasized both that they are easily overlooked by those at the delivering and receiving end of the act and that their insidiousness allows them to be seen only when resultant cumulative impact exposes harm (Brennan, 2016).
A dearth of research exists on the encounters or impact of microinequities on patients in health care. This study has added to the understanding that PWPDs encounter microinequities as part of NODD in health care. Participants described inaccessible equipment such as dental chairs, weight scales, and examination tables as routine and expected aspects of health care encounters. They also discussed the normalized expectation that providers have limited understanding of caring for a PWPD. The lack of equipment and limited provider knowledge are examples of microinequities in health care that can systematically produce disparate care for PWPDs, and their cumulative impact on health outcomes is incalculable (Neri & Kroll, 2003).
The findings describe specific strategies and skills that PWPDs have used that can inform interventions. Participants developed strategies such as seeking out information on their health and learning from peer groups. For some, holding a conversation in the focus group seemed to be eye opening. Providing forums for discussion, peer mentorship, and increasing awareness of microaggressions also are strategies suggested in the employment microinequities literature (Rowe, 1990). As an approach to increasing clients’ capacity to identify and address microinequities, occupational therapy practitioners might develop and support peer interactions as part of interventions to increase knowledge and awareness of NODD and strategies for improving health care access.
Nevertheless, few participants across groups described experiences in which they incorporated strategies of self-advocacy to take action—characteristics that align with the more advanced stages of the PDHLC (Figure 2). As described by participants, navigating the health care system puts complex burdens on PWPDs. Our findings show that without support, a PWPD may develop functional literacy (i.e., the necessary skills to understand the factual information regarding health risks) but not critical literacy (i.e., the necessary skills to be empowered and take action to access care; Nutbeam, 2008).
Previous studies have suggested intervention strategies that target consumer education in unison with developing greater advocacy and assertiveness training for PWPDs to improve health outcomes (Finlayson & Edwards, 1995; Hwang et al., 2009). These strategies might include educating a client on (1) knowledge of individual health needs, (2) knowledge on access barriers, (3) knowledge of supports within the community, and (4) knowledge of civil rights and skill development in self-advocacy. Each item provides the functional and critical knowledge that a PWPD must have to make informed health care decisions (i.e., disability health literacy).
Disability health literacy, like racial literacy (Twine, 2010), is a way of “perceiving and responding to discriminatory attitudes and structures encountered in everyday lived experiences” (p. 8), including and maybe most critically in a health care context. Depending on where they fall along the continuum, some PWPDs may need support in identifying inequities in care, whereas others may need help with developing strategies for responding. Informed by the PDHLC, occupational therapy practitioners can choose what support is needed for their client to develop disability health literacy that addresses both functional and critical literacy.
Limitations and Future Research
This study relied on a sample size of 10 participants and use of focus groups. The focus group method yielded valuable back-and-forth discussion between participants that validated their common experiences and allowed for participants to uncover disparities in their care that they may not have recognized without others’ insights. However, additional focus groups or other methods of data collection with more participants would help to further triangulate the themes on the PDHLC. Additionally, our sampling methods may limit transferability of our results to other PWPD populations in different regions or to those living in congregate settings. Basic demographic information was collected for the purposes of this study, including gender, age, and race–ethnicity. However, including background information such as insurance status and socioeconomic status could ensure maximum variation in sampling to improve transferability.
Despite these limitations, the findings of this study lay the groundwork for better understanding of how PWPDs perceive their health experiences and advocate for equitable and accessible health care. Additionally, in future studies, researchers may investigate the health literacy of PWPDs using quantitative methods and validate the PDHLC with a representative sample.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Occupational therapy practitioners work with PWPDs in many capacities, and they can advocate for change on multiple levels to promote equitable health access for this population.
On a micro level, occupational therapy practitioners can use the PDHLC to enable their clients to learn about their rights to accommodation as part of intervention designs addressing health literacy across all contexts of practice. Assisting PWPDs in developing self-advocacy skills would empower people to seek necessary accommodations in a health care setting when they are experiencing disparate care.
On a meso level, occupational therapy practitioners can educate primary care providers and clinical staff about this continuum to promote awareness of their obligations. This approach would demonstrate their need for intentional inclusion efforts because patients who attend primary care clinics may be at any level.
On a macro level, occupational therapy practitioners should use this information to advocate for universally accessible health services. Ultimately, the responsibility should not lie solely on PWPDs to educate providers about their needs for accommodations. On this larger scale, occupational therapy practitioners should also call for education and awareness of bodies governing health care in the United States to create and enforce equitable policies.
Conclusion
The PDHLC demonstrates the process of recognizing the need for accommodation for equitable care, knowing one’s rights to care, and developing strategies for requesting accommodations. This study also shows the importance of increasing health care accessibility for PWPDs to promote health and supporting health literacy interventions to empower people to take control of their health as part of an agenda to avoid inequitable health outcomes. Acknowledging that any person’s disability health literacy could be anywhere along the continuum will help inform occupational therapy practitioners, primary care providers, staff, and policymakers alike to create accessible and inclusive health care spaces.
Footnotes
Acknowledgments
We thank Lauren Little, who facilitated the early stages of this research project, and Susan Magasi, who was instrumental in foundational research on experiences of normalization of disability discrimination that informed this study.