
Abstract
An evaluation of existing evidence for supporting caregivers of people with Parkinson’s disease highlights the need for continued research in this area.
In the United States, approximately 1 million people currently live with Parkinson’s disease (PD; Parkinson’s Foundation, 2020). By 2030, the prevalence of this neurodegenerative condition is expected to double (Bae et al., 2013). People with PD experience a wide array of motor and nonmotor symptoms that affect their ability to safely and independently participate in desired roles and occupations (Lee, S. H. Kim, et al., 2019; Lee, Y. Kim, et al., 2019; Martinez-Martin et al., 2012; Tessitore et al., 2018). Because of the progressive and debilitating nature of the disease, people with PD need increasing assistance from caregivers over a long period of time (Dissanayaka et al., 2017; Lee, S. H. Kim, et al., 2019; Lee, Y. Kim, et al., 2019; Tessitore et al., 2018; Walter et al., 2018). Caregivers often experience challenges as they navigate the new and complex role of supporting a person with PD (Lee, S. H. Kim, et al., 2019; Shah et al., 2015).
Caregivers of people with PD experience a unique and varied set of demands because of the myriad symptoms associated with the disease. The amount of time spent in this role can greatly vary; one study found that 69% of caregivers of people with PD reported spending more than 56 hr per week providing care (Yang et al., 2019). A majority of these caregivers are spouses providing assistance in their home, many of whom are experiencing their own challenges related to normal aging (Lee, S. H. Kim, et al., 2019; Martinez-Martin et al., 2012; Pomponi et al., 2016; Tessitore et al., 2018). In addition, caregivers of people with PD do not typically receive formal training and possess limited knowledge of resources (e.g., support groups, equipment) that could potentially reduce their burden (Lee, S. H. Kim, et al., 2019; Shah et al., 2015).
Caring for a person with a progressive neurological condition has a negative impact on physical and psychological well-being and quality of life (QOL; Dissanayaka et al., 2017; Lee, S. H. Kim, et al., 2019; Shah et al., 2015; Tessitore et al., 2018; Walter et al., 2018). Caregivers of people with PD may experience increased burden and stress as a result of the higher number of tasks associated with caregiving and a greater sense of responsibility (DeCaro & Constantine Brown, 2016; Dissanayaka et al., 2017). People in a caregiving role demonstrate higher rates of mood disorders (particularly depression and anxiety) and reduced physical health that are often associated with the severity and progression of the disease (Cash & Lageman, 2015; DeCaro & Constantine Brown, 2016; Lee, Y. Kim, et al., 2019; Shah et al., 2015; Tessitore et al., 2018). Similarly, caregivers have reported changes in interpersonal relationships with the person with PD, other family members, and colleagues (Lee, Y. Kim, et al., 2019; Shah et al., 2015). Studies have found that only 60% of caregivers engage in social activities and that many also forgo participation in leisure activities (Cash & Lageman, 2015; Lökk, 2009). These consequences have been shown to affect the health of caregivers, which has an impact on the type of care provided to people with PD (Dissanayaka et al., 2017).
In addition, financial stress and changes in roles can undermine the health and well-being of caregivers of people with PD. As caregivers enter this new role, they often experience a reduced or terminated professional work role. Many people providing care reduce their work hours, exit the labor force, or accept wage penalties (Van Houtven et al., 2013). One study reported that one-third of caregivers under age 65 opted for early retirement to best meet the needs of their family (Lökk, 2009; Shah et al., 2015). Similarly, Lee, S. H. Kim, et al. (2019) reported that half of their 208 participants became unemployed to assume the caregiving role for the person with PD. Therefore, many caregivers and people with PD must attempt to meet the demands of high out-of-pocket costs and intensive and long-term health care needs on fixed incomes (Van Houtven et al., 2013). Van Houtven et al. (2013) reported that caregivers of people with PD and Alzheimer’s disease spent between $500 and $600 per month on out-of-pocket costs primarily related to household assistance and paid sitters. In the United States, this amount is approximately 18% to 24% of the average monthly household income, and costs continue to increase as the disease progresses (Van Houtven et al., 2013).
Occupational therapy practitioners require access to evidence-based approaches to best serve caregivers of people with PD. This topic is worthy of timely attention because the number of people with PD is expected to rise, a majority of caregivers are themselves a part of the aging population, and the physical and psychological impacts depend on the unique contexts (e.g., social, temporal, cultural) of the caregiver and care recipient (Bae et al., 2013; Lee, S. H. Kim, et al., 2019; Pomponi et al., 2016; Walter et al., 2018). The scope of the occupational therapy profession includes the use of diverse, science-driven, and client-centered approaches to best support caregivers in their essential role and to improve their QOL and well-being (Pomponi et al., 2016; Walter et al., 2018). The purpose of this systematic review was to explore the effectiveness of interventions within the scope of occupational therapy practice to support the participation of caregivers of people with PD in the caregiver role.
Method
This systematic review is one of three PD reviews in this issue supported and funded as part of the American Occupational Therapy Association (AOTA) Evidence-Based Practice (EBP) Program (see also Doucet et al., 2021, and Foster et al., 2021, in this issue). The protocol for this review was established a priori and aligned with both the protocol established by the EBP Project for this series of PD reviews and the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidelines (Moher et al., 2015). We used the following research question for this review: What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice for caregivers of people with PD to facilitate or maintain their participation in the caregiver role?
Search and Screening Strategy
The research question and search terms (Table 1) were developed by the AOTA EBP Program team, a medical librarian, and external content experts. A medical research librarian conducted the search in CINAHL, MEDLINE, PsycINFO, and OTseeker. The AOTA research methodologist did an initial title review and removed duplicates and studies that did not meet the inclusion criteria.
Key Search Terms for the Systematic Review
The search results were then provided to the review authors, who first independently reviewed each title and abstract to determine whether full-text review was needed. The review authors then conducted a second, more thorough review of eligibility along with a review of reference lists to ensure that all pertinent articles were included. For this review, we retrieved 17 articles for full-text review. We reviewed the articles for inclusion independently, with 100% agreement on article inclusion. Six articles met the inclusion and exclusion criteria Figure 1).
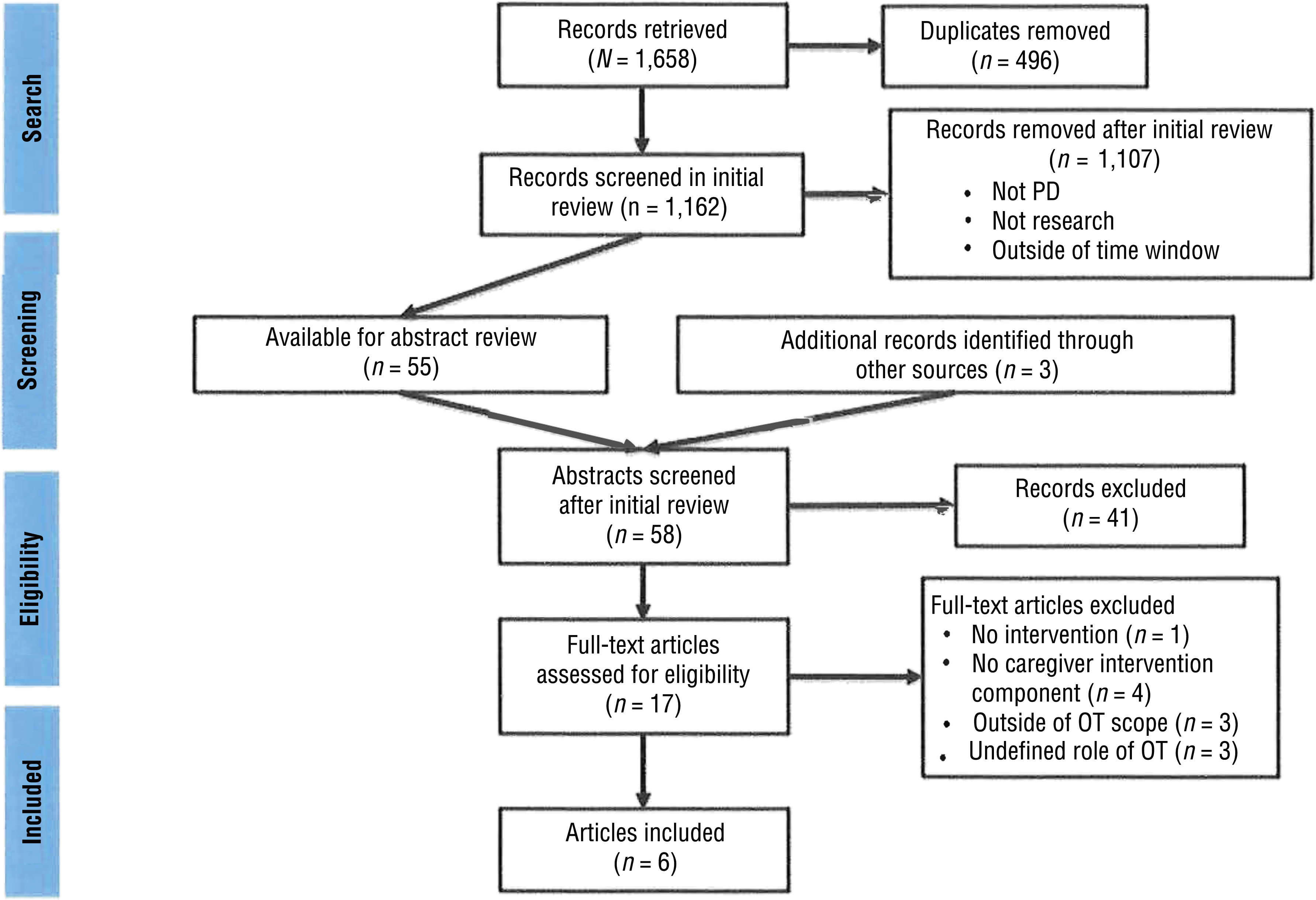
Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols flow diagram.
Inclusion and Exclusion Criteria
Articles relevant to the research question were published between January 2011 and December 2019. They met the following inclusion criteria: peer-reviewed journal article, published in English or readily translatable by the authors of the review, intervention within the scope of occupational therapy practice, Level 1a–1b through 3a–3b evidence, and adult participants (age 18+ yr) with PD.
Articles that were excluded were dissertations, theses, presentations, or conference proceedings; were published before January 2011 or after December 2019; provided Level 4 or 5 evidence; were outside the scope of occupational therapy practice; or included participants with an average age of <18 yr. The original intent of this review was to include only articles with interventions specifically for caregivers of people with PD; however, this focus was modified because of the dearth of evidence in this area. Consequently, this review includes articles examining interventions for either caregivers alone or interventions for both caregivers and people with PD. For either case, we included articles that reported individual caregiver data on at least one outcome measure that was not pooled with the data of participants with PD.
Levels of evidence were determined in accordance with recommendations by the Oxford Centre for Evidence-Based Medicine (2009):
Level 1a: Systematic review of homogeneous (e.g., similar population or intervention) randomized controlled trials (RCTs) with or without meta-analysis
Level 1b: Well-designed individual RCT (not a pilot or feasibility study with a small sample size)
Level 2a: Systematic review of cohort studies
Level 2b: Individual prospective cohort study, low-quality RCT (e.g., <80% follow-up or low number of participants, pilot or feasibility study), ecological study, two-group nonrandomized study
Level 3a: Systematic review of case–control studies
Level 3b: Individual retrospective case–control study, one-group nonrandomized pretest–posttest study, cohort study
Level 4: Case series (or low-quality cohort or case–control study)
Level 5: Expert opinion without explicit critical appraisal.
Data Extraction and Analysis
For each article included in the review, key information was extracted and entered in an evidence table (e.g., level of evidence, study design, participant inclusion criteria, intervention and control conditions; see Table A.1 in the Appendix). Anna E. Boone and Whitney Henderson conducted the evaluation and information extraction process. The AOTA EBP Project team and research methodologist reviewed the evidence table for accuracy. Articles were compared and contrasted in an attempt to develop themes, but because of the small number of studies and high variability in interventions and outcome areas, it was not possible to develop themes. Therefore, we report individual findings of each study and common themes related to the feasibility of intervention delivery with this population. Minimal to no risk of harm and no adverse events were reported in the studies included in this review.
Risk of Bias
Each author independently evaluated the risk of bias for multigroup studies using the Cochrane Risk of Bias Guidelines (Higgins et al., 2011) and for single-group studies using recommendations by the National Heart, Lung, and Blood Institute (n.d.). Findings were then collaboratively compared until a consensus was reached. Tables A.2 and A.3 contain the risk-of-bias assessment for included articles.
Overall Strength of Evidence
The strength of evidence was assessed on the basis of guidelines developed by the U.S. Preventive Services Task Force (2018). Broadly, the levels are as follows: Strong strength of evidence consists of two or more well-designed RCTs whose results are unlikely to be called into question by future studies; moderate strength of evidence is at least one high-quality RCT or multiple moderate-quality studies; and low strength of evidence consists of a limited number of flawed, low-quality studies.
Results
Of the 1,162 records screened, 17 underwent a full-text review, and 6 met the criteria and were included in the analysis (see Figure 1). Of the 6 studies, 4 were Level 3b (nonrandomized pretest–posttest design), and 2 were Level 2b (low-quality RCTs). Four studies demonstrated moderate risk of bias, 1 study met criteria for high risk of bias, and 1 met criteria for low risk of bias (see Table A.1). None of the studies included in this review were obtained from the occupational therapy literature; however, all interventions were within the scope of occupational therapy practice. Although most studies did not distinguish between primary and secondary outcomes, the numerous outcomes included caregivers’ psychosocial and cognitive outcomes measured using both standardized and unstandardized assessments. Three articles described interventions specifically for caregivers and 3 for both caregivers and people with PD. The articles all described different interventions and thus were evaluated separately. Collectively, these articles provide low strength of evidence related to the effectiveness of interventions within the scope of occupational therapy practice for caregivers of people with PD because of the limited number of low-quality studies conducted. In the sections that follow, we summarize each article by level of evidence. For more study details, see Table A.1.
Level 2b Evidence
Cash and Lageman (2015) conducted a study with low risk of bias to evaluate the use of an expressive writing intervention for caregivers (n = 14) and people with PD (n = 27). Twenty-three participants were randomized to receive three 20-min intervention sessions, and 18 were randomized to an active control group. The control group was instructed to write for the same amount of time about their daily routines. Outcome data were collected pre- and postintervention and at 4-mo and 10-mo follow-up. No significant differences between groups were noted for caregiver burden (p = .409) or salivary cortisol levels (a biological measure of stress; p = .319) from pre- to postintervention or at any follow-up time point. The high level of attrition was similar between groups. The researchers originally planned to conduct separate analyses for caregivers and people with PD for all 15 outcomes; however, this plan was modified, and only caregiver-specific data were reported for cortisol and caregiver burden.
Okai et al. (2013) conducted a small RCT with moderate risk of bias with people with PD comparing 12 sessions of cognitive–behavioral therapy (CBT; n = 28) to a wait-list control condition of standard medical care (n = 17). In addition to CBT, the researchers added to the sessions the topics of communication and interpersonal relationships with a caregiver. Although the sample included only people with PD, outcome data were collected from caregivers related to caregiver burden, neuropsychiatric disturbances, general health, and perception of marital status. Data were collected at baseline and 6 mo after the CBT intervention. Results were calculated comparing baseline to the 6-mo time point while controlling for baseline time point (i.e., whether CBT or wait list was received). Caregiver-specific outcomes demonstrated significant improvements in general health (partial η2 = .12, p = .048) but not for caregiver burden (partial η2 = .00, p = .75), distress (partial η2 = .12, p = .07), or perception of relationship quality (partial η2 = .05, p = .268).
Level 3b Evidence
Cash et al. (2016) completed a study with moderate risk of bias with caregivers (n = 10) and people with PD (n = 29) who participated in a weekly 90-min, 8-wk group mindfulness-based intervention. The researchers modeled the intervention on an evidence-based mindfulness-based stress reduction program (Kabat-Zinn, 1982) but made content and delivery changes to best meet the needs of caregivers and people with PD. Outcome measures included emotional and cognitive functioning assessments, a battery of neuropsychological tests administered preintervention and immediately postintervention, attendance data, and homework logs of time spent on mindfulness practice. Repeated measures analysis of variance showed that caregivers demonstrated a significant increase in their ability to mindfully describe internal and external experiences (p = .007, η2 = .62), but they reported no significant changes in cognition or QOL. Participants engaged in mindfulness practice 20 min/day for 6 days/wk outside of sessions and attended an average of 6 sessions; however, the researchers did not separate the data from the caregivers and people with PD data for this outcome.
Shah et al. (2015) conducted a study with moderate risk of bias with 7 female caregivers of people with PD to determine the effect of a telehealth support group on burden and mood. The researchers led a weekly 90-min session for 8 wk on four topics—caregiving, skill training, problem solving, and support—and collected data using self-report questionnaires on caregiver burden and mood pre- and postintervention. Of the 7 participants, 6 completed the postintervention outcome measures. Participants demonstrated no statistically significant changes on the Zarit Burden Interview, the American Medical Association Caregiver Self-Assessment Questionnaire, the Geriatric Depression Scale, or the Family Caregiver Assessment. Participants attended an average of 55.4% of the telehealth sessions, with a range of 3–7 sessions.
Walter and colleagues (2018) evaluated the effects of an 8-wk (60 min, 2×/wk) yoga intervention in a combined sample of caregivers (N = 4) and people with PD. This study used a retrospective pretest–posttest design and had high risk of bias (i.e., from asking participants at postintervention to reflect back on the pretest time point to complete pretest assessments). Mean change scores from the sample of 4 demonstrated improvements in depressive symptoms (M change = 3.33 on the Patient Health Questionnaire) and other psychosocial outcomes (M change = 1.67 on the Positive Aspects of Caregiving scale). Significance testing was not conducted for this study. The data from people with PD were part of a larger, unpublished study.
DeCaro and Constantine Brown (2016) completed a study with moderate risk of bias with 38 caregivers (30 women, 8 men) of people with PD. The researchers aimed to determine the impact of a single 45-min session of Laughter Yoga on caregivers’ mood and well-being using an adapted version of the Laughter Yoga “How Do You Feel (HDYF)?” questionnaire (Čokolič et al., 2013) administered before and immediately after the intervention. Using paired-sample t tests, the researchers individually analyzed each of the nine items on the HDYF self-report questionnaire. Caregivers reported significant improvement on eight items; results for the item related to stress were not significant (t = 1.23, p = .225).
Discussion
The available literature on interventions to support the participatory roles and well-being of caregivers of people with PD is narrow and highly varied at this time. Of the 6 included studies, no 2 studies developmentally evaluated the same type of intervention. As a result, research in this area is confined to early-stage feasibility studies, and no well-powered, controlled efficacy studies have been conducted. Thus, evidence-based recommendations for occupational therapy practice are challenging at this time. The gap between the demonstrated financial, social, productivity, and occupational strains of caregiving and the available evidence for interventions to support caregivers of people with PD underscores this area of research as ripe and critical.
With these limitations in mind, and the low strength of evidence available to inform and guide clinical practice, the current evidence suggests that yoga and CBT may be beneficial for facilitating participation in the caregiver role for people with PD. Specifically, as Walter et al. (2018) found, repeated yoga sessions may be beneficial for the psychosocial health (e.g., depressive symptoms), stress, and QOL of caregivers. This finding is consistent with those of other studies examining the impact of yoga on caregivers of people with chronic, progressive conditions (Danucalov et al., 2017; Lopez et al., 2018; Varambally et al., 2013; Waelde et al., 2004). Despite these consistent and positive results, occupational therapy practitioners should implement or recommend yoga interventions with caution because of methodological concerns. For example, Walter et al. asked participants to complete both the pretest and the posttest outcome measures after the yoga intervention. In other words, no pretesting was conducted until after the intervention, at which point participants were asked to reflect back to establish preintervention ratings. In addition, this study had a very small sample (n = 4), and only 3 participants completed outcome measures, limiting the ability to use significance testing to appropriately determine outcomes of intervention.
CBT provided to people with PD may also produce positive effects on caregivers’ general psychological health, but no improvements in caregiver burden or stress were found (Okai et al., 2013). Occupational therapy practitioners need to interpret these results carefully because the caregivers did not directly participate in the intervention. Limited evidence exists on the use of CBT with caregivers. A recent systematic review and meta-analysis suggested that CBT can be effective at reducing anxiety and depression in people with PD (Zhang et al., 2020); however, it may be shortsighted to assume that improvements in people with PD through engagement in CBT will automatically translate to increases in their caregivers’ health. In addition, Okai et al. (2013) recruited a specific subset of people with PD—those who demonstrated impulse control behaviors (e.g., gambling, shopping, sexual behavior). Although such behaviors can occur as a side effect of traditional dopamine replacement medications, approximately 14% of people with PD have been found to demonstrate these behaviors (Weintraub et al., 2010). Therefore, the generalizability of Okai et al.’s findings to the larger PD population and their caregivers is limited.
Although it is not possible to draw conclusions regarding the efficacy of interventions or to infer what specific components of interventions may or may not be effectual, the studies in this systematic review collectively provide important information about the feasibility of conducting these types of studies with caregivers. Practical considerations (e.g., timing, access) should be addressed in developing possible caregiver interventions based on current studies. Collectively, the studies reported low adherence rates to intervention sessions, a finding that also held true for the telehealth intervention (Shah et al., 2015), and high levels of attrition were also demonstrated. Reasons for low adherence and high attrition rates included caregiver or patient health concerns, lack of available time, and the financial demands of the caregiving role. These findings highlight the need for interventions to be flexible and feasible in terms of cost and required time commitment, potentially through modifications in format (e.g., number of sessions, method of delivery).
In addition, it is imperative to design interventions and studies that are not based on the assumption that an intervention will be equally efficacious for people with PD and their caregivers. Many of the studies of interventions targeted to people with PD measured the impact on caregiver burden. Greater depth and breadth of measurement are needed to capture improvements in caregivers beyond stress and burden to include health, well-being, and participation in life activities outside of the caregiving role. Although expanding the caregiver outcomes measured is a step in the right direction to properly acknowledge and begin to assuage their needs, researchers must design interventions that are intentionally tailored to best meet the unique needs of caregivers of people with PD.
Limitations
The findings of this review are limited by the limitations of the individual articles. As with any systematic review, articles could potentially have been missed in the search, although we made every effort to include all relevant articles. Included studies also have a risk of positive publication bias and a relatively high risk of bias. Finally, the diversity in interventions and outcomes in combination with the small sample sizes severely limits generalizability.
Implications for Occupational Therapy Practice, Research, and Education
Caregiving is an important role in all populations, including people with PD. Occupational therapy practitioners need to continue to acknowledge and address the impact of the caregiving role on caregivers’ health, QOL, participation, and contexts. Interventions that capitalize on the holistic and occupation- and evidence-driven nature of the profession are desired. This identified need will only further increase as the population continues to age and PD care advances lead to increased life expectancy. Because of the low strength of evidence, occupational therapy practitioners and educators should consider the following recommendations with caution:
A need persists for well-designed studies on interventions to support the role of caregivers for people with PD.
Occupational therapy curricula should equip students to conduct research that spans feasibility to efficacy to more adequately address the unique needs of caregivers.
Occupational therapy educators can increase emphases on the unique needs of caregivers and further educate students on the implementation of interventions within the scope of occupational therapy practice to support caregivers’ health and participation in this role.
Evidence-based practice recommendations are limited because of the low number of studies with high risk of bias; however, practitioners should acknowledge the contextual and occupational needs of this population.
Conclusion
The literature regarding interventions within the occupational therapy scope of practice to support caregivers of people with PD is in its infancy. In spite of the low strength of the available evidence, this area of research is of great importance and fits well with the skill set of occupational therapy practitioners. Future studies need to move beyond feasibility to strengthen evidence that practitioners can use. RCTs with large samples and long-term follow-up data are needed to build on existing evidence.
Footnotes
Acknowledgments
This systematic review was supported by the American Occupational Therapy Association (AOTA) and completed as part of AOTA’s Evidence-Based Practice Project. The authors declare no conflict of interest.
Appendix. Evidence and Risk-of-Bias Tables for the Systematic Review
Risk-of-Bias Table for Single-Group Studies Included in the Systematic Review
| Citation | Study Question | Eligibility Criteria | Participants | Enrollment | Sample Size | Intervention | Outcome Measures | Assessors Blinded | Loss to Follow-Up | Statistical Methods | Outcome Measures | Overall Risk |
| Cash et al. (2016) | Y | Y | Y | Y | N | Y | Y | N | N | Y | N | Moderate |
| DeCaro & Constantine Brown (2016) | Y | Y | Y | N | N | Y | N | N | Y | Y | N | Moderate |
| Shah et al. (2015) | Y | Y | N | Y | N | N | Y | N | Y | Y | N | Moderate |
| Walter et al. (2018) | Y | N | NR | NR | N | NR | N | N | N | N | N | High |
Note. N = no; NR = not reported; Y = yes. Adding Yes scores for each item and dividing by 11 yields a risk-of-bias rating: low risk = 76%–100%, moderate risk = 26%–75%, and high risk = 0%–25%. Risk-of-bias tool adapted from Quality Assessment Tool for Before–After (Pre–Post) Studies With No Control Group, by National Heart, Lung, and Blood Institute, n.d. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
Citation: Boone, A. E., Henderson, W., & Hunter, E. (2021). Role of occupational therapy in facilitating participation among caregivers of people with Parkinson’s disease: A systematic review (Table A.3). American Journal of Occupational Therapy, 75, 7503190010. https://doi.org/10.5014/ajot.2021.046284
*
Indicates studies included in the systematic review.