
Abstract
This systematic review supports the role of occupational therapy in providing self-management interventions to address ADLs and sleep for adults with diabetes and other chronic conditions.
Chronic conditions, such as diabetes, heart disease, stroke, cancer, and obesity, are the leading and most preventable causes of death and disability (Centers for Disease Control and Prevention [CDC], 2019). Chronic conditions account for 75% to 90% of total health care spending in the United States (CDC, 2020; Lewin Group, 2010; Moses et al., 2013). Depending on the type of condition or course of the illness, physical changes from a chronic condition may cause functional impairments, leading to decreased independence and self-efficacy (American Occupational Therapy Association [AOTA], 2015; Kim & Choi, 2015; Maresova et al., 2019). Occupational therapy practitioners who work with adults with chronic conditions have an important role in addressing participation in meaningful daily activities (AOTA, 2015). The focus of this review is on the occupations of activities of daily living (ADLs) and rest and sleep.
ADLs, including bathing, toileting, dressing, eating, and personal hygiene and grooming, are an important aspect of everyday life for adults. These activities are “fundamental to survival and to living in a social world” because they are deemed “necessary for good physical and mental health, and also important for group acceptance” (Christiansen et al., 2015, p. 13; see also AOTA, 2020). Decreased independence in ADLs is associated with decreased quality of life, increased health care costs, and a higher chance of mortality (Millán-Calenti et al., 2010; Ramos et al., 2001; Scott et al., 1997). In addition, impaired ADL performance is correlated with admission to nursing homes or assisted living facilities (Gaugler et al., 2007). Addressing performance in ADLs is a crucial aspect of helping people with chronic conditions maintain independence.
Like ADLs, rest and sleep are an essential part of all daily routines. The Occupational Therapy Practice Framework: Domain and Process (4th ed.; AOTA, 2020) defines rest and sleep as “activities related to obtaining restorative rest and sleep to support healthy, active engagement in other occupations” (p. 32). Adults need at least 7 hr of sleep each night; however, short sleep duration is not only common but is also associated with adverse health outcomes, including obesity, physical inactivity, and cigarette smoking (CDC, 2017). Poor sleep quality is associated with depression (Tsuno et al., 2005), work-related fatigue (Querstret & Cropley, 2012), and low quality of life (Khan-Hudson & Alessi, 2008; Lo & Lee, 2012). The diagnosis of a chronic condition is associated with poorer sleep quality (Kemple et al., 2016; McSharry et al., 2012), suggesting that sleep and chronic health conditions are intricately related. Occupational therapy practitioners should be prepared to address sleep and rest as part of an overall plan of care for adults with chronic conditions.
One approach for addressing occupational performance in ADLs and rest and sleep for adults with chronic conditions is self-management training. Interventions to improve self-management involve teaching new health-specific skills (e.g., managing medications, monitoring weight or blood sugar, increasing physical activity) and ways to incorporate these activities into daily routines (AOTA, 2015). Self-management programs have been found to be effective in improving health management and quality of life among adults with chronic conditions, suggesting that these interventions are an important tool for occupational therapy practitioners working with this population (Berger et al., 2018). The purpose of this systematic review was to assist occupational therapy practitioners in making evidence-based decisions regarding self-management interventions to improve ADLs and rest and sleep among adults with chronic conditions.
Method
This systematic review is one of four reviews of the literature on chronic conditions supported by the AOTA Evidence-Based Practice (EBP) Program. The method for the review was specified in advance by EBP Project staff in collaboration with the review authors and was documented in a protocol. The following research question guided this review: What is the evidence for the effectiveness of self-management interventions within the scope of occupational therapy practice to improve the performance of ADLs and sleep and rest among community-dwelling adults with chronic conditions?
Search Strategy
This review was carried out according to the Cochrane Collaboration methodology (Higgins et al., 2016) and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting a systematic review (Moher et al., 2009). Search terms for the review were identified by the EBP Program research methodologist and AOTA staff in consultation with the review authors. The search terms were identified to capture pertinent studies and to ensure that the terms relevant to the specific thesaurus of each database were included. Table 1 lists the search terms used in this review. A medical librarian with experience in completing systematic review searches conducted the search in the Cochrane Database of Systematic Reviews, MEDLINE, PsycINFO, CINAHL, and OTseeker databases. The research methodologist completed the initial title review of the search results, eliminating all records clearly not relevant to the scope of the review (e.g., wrong population, not research).
Key Search Terms for the Systematic Review
Note. ADLs = activities of daily living.
Inclusion and Exclusion Criteria
Several inclusion and exclusion criteria outlined the structure for the quality, type, and years of publication of the articles incorporated into the review. This review included peer-reviewed scientific literature published in English between 1995 and 2019. The intervention approaches examined were within the scope of occupational therapy practice (i.e., not requiring additional licensure or degrees) for adults with chronic conditions older than age 18. Studies with participants living in the community, including retirement homes or assisted living centers, were included; those with participants living in skilled nursing facilities were excluded. Participants’ chronic conditions included cardiovascular disease, Type 2 diabetes, heart disease, hypertension, chronic respiratory problems, and kidney disease. Studies that included participants with stroke, Alzheimer’s disease, arthritis, and cancer were excluded from this review because these studies were included in other published AOTA systematic reviews and practice guidelines. This review excluded data from presentations, conference proceedings, non–peer-reviewed research literature, dissertations, and theses. Studies with no outcomes related to ADLs or rest and sleep and those that addressed only functional mobility or quality of life were also excluded.
AOTA uses levels of evidence modeled on those developed in evidence-based medicine (Oxford Centre for Evidence-Based Medicine, 2009). Levels of evidence are as follows:
Level 1a: systematic reviews of homogeneous (e.g., similar population or intervention) randomized controlled trials (RCTs), with or without meta-analysis
Level 1b: well-designed individual RCTs (not a pilot or feasibility study with a small sample)
Level 2a: systematic reviews of cohort studies
Level 2b: individual prospective cohort studies, low-quality RCTs, ecological studies, and two-group nonrandomized studies
Level 3a: systematic reviews of case–control studies
Level 3b: individual retrospective case–control studies, one-group nonrandomized pretest–posttest studies, and cohort studies
Level 4: case series (and low-quality cohort and case–control studies)
Level 5: expert opinion without explicit critical appraisal.
Articles containing Level 1b, 2b, and 3b evidence were included in this review. Systematic reviews were excluded, because not all of the individual studies met the inclusion criteria. The systematic reviews were evaluated, and pertinent individual articles were added to the articles being reviewed. No studies providing Level 4 or 5 evidence were included in the review.
Data Extraction
The authors worked collaboratively to evaluate all studies received from the research methodologist and those gathered by hand searching the systematic reviews. Initial review of the articles was conducted individually by the three authors, who then engaged in collaborative discussion to reach consensus on inclusion or exclusion. We extracted key information from each study (level of evidence, study design, participants, intervention, interventionists, outcome measures, and results) into an evidence table (see Table A.1 in the Appendix) and then categorized the studies into themes. The EBP Project research methodologist reviewed the evidence table to ensure quality control.
Evidence Table for the Systematic Review of Self-Management Interventions to Improve ADLs and Sleep for Adults With Chronic Conditions
Note. ADLs = activities of daily living; CBT–I = cognitive–behavioral therapy for insomnia; COPD = chronic obstructive pulmonary disease; CS–PFP10 = 10-Item Continuous Scale Physical Functional Performance Test; HF = heart failure; HRQOL = health-related quality of life; LEA = lower extremity amputation; PSQI = Pittsburgh Sleep Quality Index; RCT = randomized controlled trial.
Only measures related to the outcomes of interest are listed.
This table is a product of AOTA’s Evidence-Based Practice Program and AOTA and is copyright © 2021 by the American Occupational Therapy Association. It may be freely reproduced for personal use in clinical or educational settings as long as the source is cited. All other uses require written permission from the American Occupational Therapy Association. To apply, visit http://www.copyright.com.
Citation. Smallfield, S., Fang, L., & Kyler, D. (2021). Self-management interventions to improve activities of daily living and rest and sleep for adults with chronic conditions: A systematic review (Table A.1). American Journal of Occupational Therapy, 75, 7504190010. https://doi.org/10.5014.ajot.2021.046946
Analysis
Each article was assessed for risk of bias as described in the Cochrane risk-of-bias guidelines (Higgins et al., 2016). We collaborated to reach consensus on the rating of low, moderate, or high risk for each category of bias assessed (see Table A.1). We also analyzed each theme for overall strength of evidence to assist in determining recommendations for occupational therapy education, practice, and research. Analysis of study design, findings, and risk of bias determined the strength of evidence provided by each study. The number of studies, evidence level, risk of bias, and significance and consistency of the findings were synthesized to develop the overall strength of evidence for each theme, as follows:
Strong strength of evidence: consistent results from two or more well-conducted Level 1 studies.
Moderate strength of evidence: one or more well-conducted RCTs or multiple moderate-quality studies (Level 2 or 3). The available evidence is sufficient to determine health outcomes, but confidence in the estimate is constrained by factors such as the number, size, or quality of individual studies or inconsistency in findings across individual studies.
Low strength of evidence: a small number of low-level studies, flaws in the available studies, and some inconsistency in findings across individual studies. The available evidence is insufficient to assess effects on health and other outcomes of relevance to occupational therapy because of the limited number or size of studies, important flaws in study design, or inconsistency in findings across individual studies (U.S. Preventive Services Task Force, 2012).
Results
Fifteen articles based on 14 studies met the inclusion criteria (Figure 1). We identified 6 Level 1b, 4 Level 2b, and 4 Level 3b studies for inclusion in the final qualitative synthesis. The article by Kapella et al. (2011) reported on 2 studies, a Level 3b feasibility study and a Level 2b RCT, whereas Fan et al. (2013, 2014) and Tang et al. (2010, 2012) each reported on 1 study in 2 articles. The 15 articles were categorized into two themes according to type of intervention: (1) interventions to address ADL performance (11 articles from 9 studies) and (2) interventions to address sleep (5 articles from 6 studies); 1 article (Gary et al., 2011) was included in both themes. The subthemes for ADL performance are (1) diabetic foot care and education and (2) exercise and education. The subthemes for sleep are (1) sleep education and (2) exercise interventions. The characteristics of each study are reported in Table A.1.
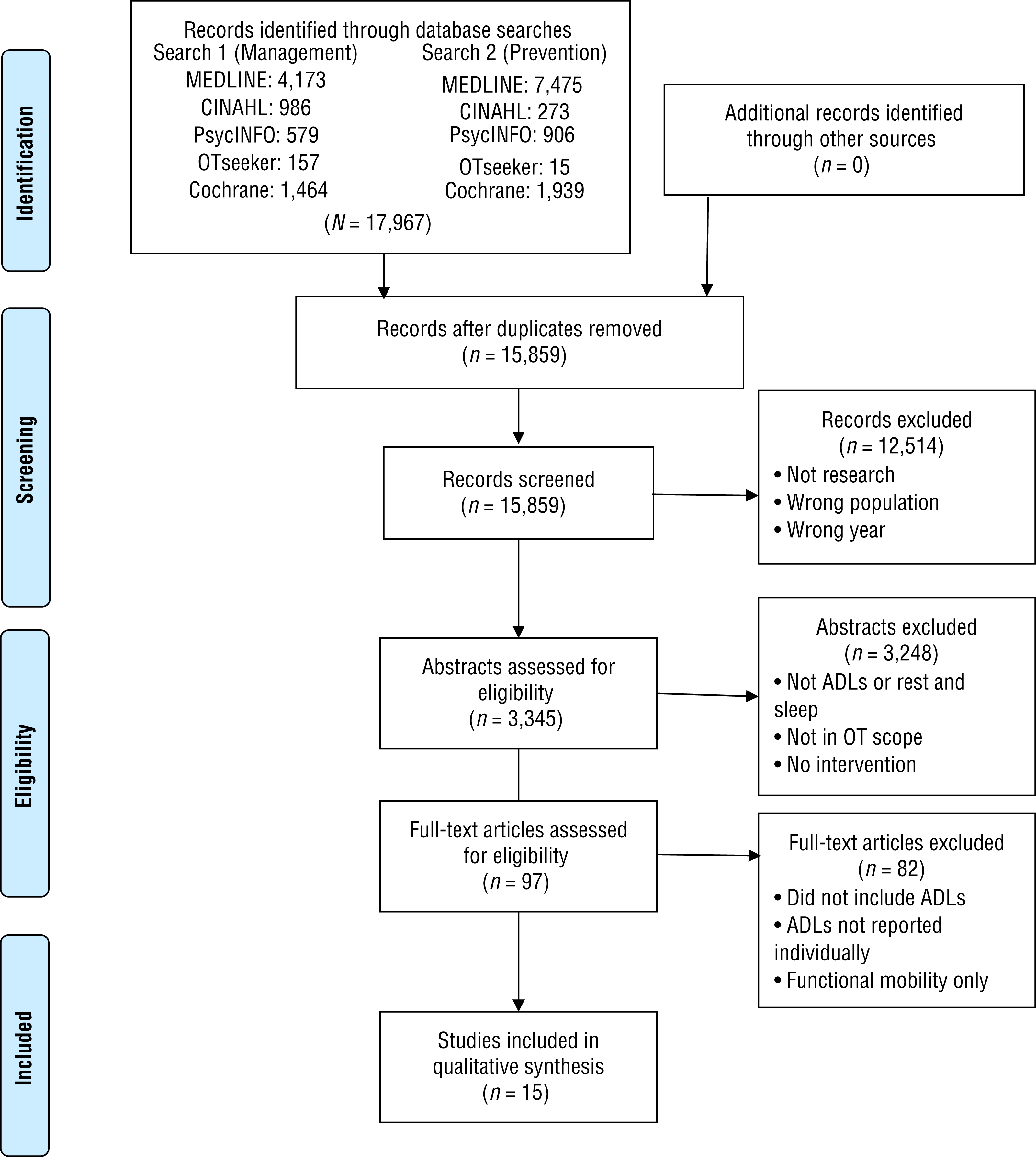
Flow diagram of studies through the systematic review.
Risk of Bias
For the theme of interventions to address ADL performance, 7 of 11 articles had moderate risk, and 4 had low risk of bias. The theme of interventions to address sleep included 5 articles, 2 with moderate risk and 3 with low risk of bias. Many of the studies included in this review did not blind the participants, personnel, or outcome assessments, which led to potential bias risks. Tables A.2 and A.3 show the risk-of-bias evaluations for all articles included in this review.
Risk-of-Bias Table for Randomized and Nonrandomized Controlled Trials
Note. Categories for risk of bias are as follows: + = low risk of bias; ? = unclear risk of bias; – = high risk of bias. Scoring for overall risk of bias assessment is as follows: L = low overall risk of bias (0–3 minuses); M = moderate overall risk of bias (4–6 minuses). Table format adapted from “A Revised Tool for Assessing Risk of Bias in Randomized Trials,” by J. P. T. Higgins, J. A. C. Sterne, J. Savović, M. J. Page, A. Hróbjartsson, I. Boutron, . . . S. Eldridge, 2016, Cochrane Database of Systematic Reviews 2016, Issue 10 (Suppl. 1), 29–31. https://doi.org//10.1002/14651858.CD201601
This table is a product of AOTA’s Evidence-Based Practice Program and AOTA and is copyright © 2021 by the American Occupational Therapy Association. It may be freely reproduced for personal use in clinical or educational settings as long as the source is cited. All other uses require written permission from the American Occupational Therapy Association. To apply, visit http://www.copyright.com.
Citation: Smallfield, S., Fang, L., & Kyler, D. (2021). Self-management interventions to improve activities of daily living and rest and sleep for adults with chronic conditions: A systematic review (Table A.2). American Journal of Occupational Therapy, 75, 7504190010. https://doi.org/10.5014.ajot.2021.046946
Risk-of-Bias Table for Before–After (Pre–Post) Studies With No Control Group
Note. Y = yes; N = no; NR = not reported. Scoring for overall risk of bias assessment is as follows: L = low risk of bias (0–3 Ns); M = moderate risk of bias (4–8 Ns). Table format adapted from Quality Assessment Tool for Before–After (Pre–Post) Studies With No Control Group, by National Heart, Lung, and Blood Institute, 2014. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
This table is a product of AOTA’s Evidence-Based Practice Program and AOTA and is copyright © 2021 by the American Occupational Therapy Association. It may be freely reproduced for personal use in clinical or educational settings as long as the source is cited. All other uses require written permission from the American Occupational Therapy Association. To apply, visit http://www.copyright.com.
Citation: Smallfield, S., Fang, L., & Kyler, D. (2021). Self-management interventions to improve activities of daily living and rest and sleep for adults with chronic conditions: A systematic review (Table A.3). American Journal of Occupational Therapy, 75, 7504190010. https://doi.org/10.5014.ajot.2021.046946
Participant Characteristics
Participants in the included studies were diagnosed with at least one chronic health condition. Specifically, 835 participants had diabetes, 186 participants had respiratory conditions, 170 participants had cardiac conditions, and 243 had unspecified chronic conditions.
Outcome Measures
The studies that addressed ADL performance for diabetic foot self-care used heterogenous measures to determine outcomes including self-efficacy, knowledge, attitudes, behaviors, and practices related to foot self-care. One common assessment used was the Summary of Diabetes Self-Care Activities (Toobert et al., 2000). There was no consistency in outcome measures used to assess ADLs in participants with conditions other than diabetes.
The five studies that addressed the outcome of sleep also used various self-report outcome measures for sleep quality, sleep attitudes, sleep difficulties, and fatigue. The Pittsburgh Sleep Quality Index (Buysse et al., 1989) was the only outcome measure used in more than one study.
Intervention to Address ADL Performance
Eleven articles described studies of interventions to address ADL performance: 3 Level 1b (Ahmad Sharoni et al., 2018; Borges & Ostwald, 2008; Dobson et al., 2018), 4 Level 2b (Bendstrup et al., 1997; Gary et al., 2011; Tang et al., 2010, 2012), and 4 Level 3b (Collins-McNeil et al., 2012; Fan et al., 2013, 2014; Swavely et al., 2014). Two subthemes related to ADL performance emerged: (1) diabetic foot care and education and (2) exercise and education.
Diabetic Foot Care and Education
Seven studies described in 9 articles involved interventions to promote diabetic foot care self-management. These interventions included discussion of risk factors and review of daily foot self-care practices and strategies.
Six studies described in seven articles demonstrated significant improvement in outcomes after the intervention. Dobson et al. (2018, Level 1b) compared a 9-mo telehealth self-management support program to usual care. The intervention group showed significant improvement in foot care behavior compared with the control group. Ahmad Sharoni et al. (2018, Level 1b) conducted a study in which participants received four sessions of a health education program plus biweekly 20-min one-on-one follow-up sessions for 12 wk. Foot self-care behavior, foot care self-efficacy, foot care outcome expectation, and knowledge of foot care significantly improved in the intervention group compared with the control group across three time points. In a three-arm RCT, Borges and Ostwald (2008, Level 1b) studied the benefit of a 15-min education intervention after participants received a 5-min assessment for amputation risk. Mixed results were found for foot self-care knowledge and behavior among the three groups; however, those who received education in addition to the risk assessment demonstrated significantly improved foot self-care behaviors.
In 1 study reported in two articles, Fan et al. (2013, 2014, both Level 3b) provided two in-person sessions followed by two 10-min telephone booster sessions to address awareness of diabetic risk factors and foot care. They found that the occurrence of foot problems was significantly reduced at 3-mo follow-up (Fan et al., 2013). They also found significantly improved foot self-care knowledge and foot self-care efficacy from baseline to intervention completion; foot self-care behavior was significantly improved at 3-mo follow-up (Fan et al., 2014). Collins-McNeil et al. (2012, Level 3b) studied a 6-wk diabetes self-management program including one session on diabetic foot care and found significant improvement in foot self-care practices from pretest to posttest. Last, Swavely et al. (2014, Level 3b) studied the effectiveness of 13 hr of individualized and group diabetes education over 12 wk. They found that patient-reported foot self-care behaviors were significantly improved at posttest.
Finally, 1 study described in two articles examined an intervention for foot self-care behaviors (Tang et al., 2010, 2012, both Level 2b). This study evaluated the effectiveness of weekly sessions of the Lifelong Management program over 6 and 24 mo and found no significant improvement.
Exercise and Education
Two Level 2b studies examined the impact of physical training and education interventions to address ADL self-management for people with chronic obstructive pulmonary disease (COPD; Bendstrup et al., 1997) and heart disease (Gary et al., 2011). Bendstrup et al. (1997) examined dressing, eating, and bathing, whereas Gary et al. (2011) studied dressing tasks and picking up items; both found significant improvement in ADL performance after the intervention.
Bendstrup et al. (1997, Level 2b) examined a 12-wk program for adults with COPD consisting of group occupational therapy training in ADL techniques, regular exercise training, and education sessions. The intervention group showed significant improvements in ADL scores compared with the control group at 12 and 24 wk. Gary et al. (2011, Level 2b) evaluated a 12-wk progressive home-based exercise program with individualized instruction and demonstration to improve physical function in adults with heart disease. They found significant improvement in the intervention group in specific ADL tasks, including donning and doffing a jacket and picking up clothing items.
Summary
Strong strength of evidence supports education interventions within the scope of occupational therapy practice to improve diabetic foot self-care. Low strength of evidence is available for exercise and education interventions to improve ADLs for people with COPD and heart disease.
Interventions to Improve Sleep
Five articles included interventions within the scope of occupational therapy practice to improve sleep. We found no articles that specifically addressed rest. Of the included studies, 3 were Level 1b RCTs (Ghavami et al., 2018; Perneger et al., 2002; Rybarczyk et al., 2001), and 2 were Level 2b RCTs (Gary et al., 2011; Kapella et al., 2011). Kapella et al. (2011) reported results from a one-group pretest–posttest Phase 1 study (Level 3b) in the same article as a Phase 2 RCT. Two studies included participants with heart conditions (Gary et al., 2011; Ghavami et al., 2018), 2 included participants with respiratory conditions (Kapella et al., 2011; Perneger et al., 2002), and 1 study included participants with multiple health conditions (Rybarczyk et al., 2001). Two subthemes, mind–body self-care education and exercise, are included in this theme.
Mind–Body Self-Care Education
Four of the 5 sleep studies evaluated interventions that included a mind–body self-care educational component, and 3 of them demonstrated significant positive outcomes for sleep. Ghavami et al. (2018, Level 1b) found that a program of self-care education (sleep hygiene, nutrition, and physical activity) over 7 wk plus individualized consultation over 3 mo resulted in a significant improvement in mean sleep quality scores compared with routine care. Kapella et al. (2011, Level 3b–2b) provided 6 weekly individual sessions of cognitive–behavioral therapy (relaxation techniques, sleep hygiene, and techniques for managing sleep loss) and found significant benefit for the outcomes of insomnia severity, sleep quality, wake after sleep onset, sleep efficiency, fatigue, and beliefs and attitudes about sleep compared with the control condition of wellness education. Rybarczyk et al. (2001, Level 1b) found that 8 sessions of a 2-hr mind–body wellness intervention resulted in significant improvement in self-reported sleep difficulties compared with the wait-list control condition; the findings were maintained at 1-yr follow-up.
Perneger et al. (2002, Level 1b) examined an intervention consisting of three weekly sessions of group self-management instruction. They found no significant differences in sleep outcomes compared with a wait-list control condition.
Exercise
Gary et al. (2011, Level 2b) studied the effectiveness of a 12-wk combined aerobic and resistance exercise program delivered at home compared with a wait-list attention control consisting of instruction on stretching and flexibility exercises in 5–6 home visits over 12 wk. They found no differences between groups in sleep outcomes.
Summary
Moderate strength of evidence supports longer term (≥6–8 wk) mind–body self-care interventions to improve sleep. Two strong Level 1b studies and 1 Level 3b–2b study found significant improvements; however, 1 short-term (3-wk) Level 1b study of a group intervention did not find significant improvement in sleep outcomes. Low strength of evidence is available from 1 small RCT for the use of a home-based aerobic and resistance exercise program to address sleep outcomes.
Discussion and Implications
The purpose of this systematic review was to examine the effectiveness of self-management interventions within the scope of occupational therapy practice to improve the performance of ADLs and sleep among community-dwelling adults with chronic conditions. Regarding ADLs, the results provide strong strength of evidence to support education interventions to improve diabetic foot self-care, and therefore education interventions should be offered routinely to improve foot care knowledge and behavior in adults with diabetes. Specific education components include a discussion of risk factors that lead to complications of diabetes and the integration of foot inspection and hygiene into daily self-care routines. The included studies showed no consensus on the appropriate dosage of diabetic foot-care education; further research is needed to explore this topic. Occupational therapy is well situated to address diabetic foot self-care in the context of enhancing both independence in ADLs and the self-management of chronic conditions. Routine diabetic foot care enables the performance of a wide variety of occupations, including social interests and leisure pursuits.
Low strength of evidence is available to support exercise and education interventions to improve ADLs for people with heart disease and COPD; exercise interventions thus should be used on a case-by-case basis. The available evidence for the effects of these interventions on ADL performance is limited by the small number and size of included studies; therefore, further research is needed before additional recommendations on application in occupational therapy practice can be made.
Regarding sleep, moderate strength of evidence indicates that mind–body self-care education is effective in enhancing sleep outcomes. Occupational therapy practitioners should routinely provide education that addresses sleep hygiene, nutrition, relaxation techniques, and physical activity when working with adults with chronic conditions to address sleep. It is important for practitioners to address sleep because of the critical role that sleep plays in the performance of daytime occupations.
Finally, we found low strength of evidence, from 1 small RCT, for exercise interventions to improve sleep in adults with chronic conditions. Not enough research on this type of intervention is available to guide clinical practice. Practitioners should use exercise interventions with caution on a case-by-case basis for adults with chronic conditions. Further research on exercise interventions to enhance sleep outcomes is needed.
Implications for Occupational Therapy Education
ADLs and sleep are essential occupations in daily life. This review adds valuable evidence to support the role of occupational therapy in addressing ADLs and sleep for adults with chronic conditions. As the prevalence of chronic conditions continues to rise, the need will increase for occupational therapy practitioners trained to address occupational performance in this population. On the basis of the results of this review, occupational therapy curricula should include knowledge and skill training in chronic disease self-management to facilitate the performance of ADLs and sleep, including the following:
Knowledge of chronic conditions affecting occupational performance, health, and well-being
Assessment of sleep quality, habits, and routines
Assessment of ADL performance, including diabetic foot care
Education in the importance of sleep hygiene, nutrition, and physical activity as part of health management
Education addressing diabetic foot self-care as part of symptom and condition management
Training in leading group self-management interventions and understanding the complexity of health behavior change
Training in the use of standardized outcome measures to demonstrate intervention effectiveness
Knowledge of the potential need for referral to other members of the interprofessional health care team.
Implications for Occupational Therapy Research
Occupational therapy has the potential to play a significant role in enhancing self-management for adults with chronic conditions. This review contributes to the existing body of research on occupational therapy interventions to improve ADLs and sleep for adults with chronic conditions. However, the studies reviewed are limited by the lack of individual reporting on ADL outcomes, inconsistent dosages, lack of consistent outcome measures enabling comparison across studies, and absence of occupational therapy practitioners as interventionists. Future research on self-management interventions within the scope of occupational therapy practice for adults with chronic conditions should include interventions that demonstrate the knowledge and skill distinct to occupational therapy. Such research should also include
Clear definitions and assessment measures of intended outcomes;
Determination of appropriate dosage, frequency, and timing of intervention;
Consistency across research in outcomes assessed and outcome measures used; and
Tailored interventions with individualized interaction.
Implications for Occupational Therapy Practice
On the basis of the results of this review, occupational therapy practitioners working with adults with chronic conditions should use the following interventions as part of routine service provision:
Education interventions to improve performance of diabetic foot self-care as part of overall condition management
Mind–body self-care education to improve sleep.
The following interventions should be used on a case-by-case basis:
Exercise interventions to improve performance of ADLs
Education interventions to improve performance of ADLs.
The following interventions should be used with caution:
Exercise interventions to improve sleep.
Limitations
All systematic reviews have the limitation of potentially missed relevant articles. In addition, although the body of evidence supporting interventions within the scope of occupational therapy practice for adults with chronic conditions is growing, further original research is needed to support interventions to improve the self-management of chronic conditions, specifically for the outcomes of ADLs and rest and sleep. This review was completed according to the terms and definitions provided in the 3rd edition of the Occupational Therapy Practice Framework: Domain and Process (AOTA, 2014); the 4th edition has since been published, in which the categorization of terms changed. In the 3rd edition, health management (of which self-management is a component) was an occupation within instrumental ADLs; in the 4th edition, it is recognized as its own category.
This review is also limited by the limitations of the included articles. Many did not distinguish ADL outcomes from instrumental ADL outcomes. Additionally, several articles we screened used outcome measures that mixed constructs and did not report individual items; these articles are not included in this review. Finally, the review may be limited by the potential for publication bias, which occurs when relevant studies are not published because of nonsignificant findings.
Conclusion
This systematic review focused on self-management interventions within the scope of occupational therapy practice to enhance ADLs and sleep and rest for adults with chronic conditions. The 15 included articles addressed the themes of ADLs and sleep. Strong strength of evidence supports diabetic foot self-care education to enhance ADL performance, and moderate strength of evidence supports mind–body self-care interventions to enhance sleep. Occupational therapy practitioners working with adults with chronic conditions should routinely offer these interventions. Future research should examine the appropriate dosage of intervention and use clear and consistent outcome measures.
Footnotes
Acknowledgments
This review was completed with support from the American Occupational Therapy Association. We thank Deborah Lieberman, Beth Hunter, and Hillary Richardson for their guidance on this project, as well as Riley Perdue, who assisted with minor editing. Darby Kyler completed this systematic review in partial completion of her doctoral capstone project.
Appendix. Evidence and Risk-of-Bias Tables for the Systematic Review
*
Indicates studies included in the systematic review.