
Abstract
A study of 5 adults with first-episode psychosis (FEP) found that health management dominated participants’ occupations immediately after FEP and hindered their social participation as they experienced a liminal space (i.e., transition space) in their life trajectory.
Health management occupations are generally considered essential to effective disease management (Gearing et al., 2014; Lam et al., 2011). Adhering to a medication schedule, attending outpatient appointments, engaging in health-promoting habits (e.g., diet, sleep, socialization), and educating oneself about an illness are important occupations to promote health and manage disability. Despite their necessity, the drawbacks of health management occupations are rarely considered.
Health management occupations require extensive time, especially in the early stages of a new illness. Organizing travel, learning about and receiving treatment, monitoring health, and managing treatment side effects require significant time and effort that contribute to overall treatment burden (Sav et al., 2015). Treatment burden encompasses the “physical, financial, temporal, and psychosocial time demands” (Sav et al., 2015, p. 316) involved in treating a disease to either change its course or ameliorate its effects. Treatment burden can contribute to the recurrence of disease, decline in health, nonadherence to treatment, reduced survival, lower treatment satisfaction, reduced employment, and diminished quality of life (Sav et al., 2015). The necessary adoption of occupations for managing illness places new demands on performance and time. Difficulty balancing these demands can contribute to disengagement from occupation after first-episode psychosis (FEP; Krupa et al., 2010), thereby exacerbating treatment burden.
Health management occupations also contribute to the assimilation of an illness into one’s identity. Shared clinical environments, routine appointments with mental health providers, and strategies for illness management instill an identity of mental illness in people who have had a recent psychotic episode (Davidson, 2007; Estroff, 1981). Opportunities for participation beyond mental health settings become limited, partly as a result of increased treatment burden during the initial stages of illness. Without these occupational opportunities, identities related to chronic impairment and illness flourish. Indeed, the stress associated with managing FEP may “predispose young people to the phenomenon of illness engulfment, whereby personal identity is lost and replaced with a sense of self defined entirely by the illness” (McCay et al., 2006, p. 105). This is particularly concerning for people with FEP because onset typically occurs during a critical developmental life stage (i.e., early adulthood) when identity is more fluid and malleable. Becoming engulfed by illness can lead to demoralization, depression, and emotionlessness as people lead progressively more restricted lives, and “all activities of daily life gradually revolve around being a psychiatric patient, with accompanying alienation from others and loss of previous social roles” (McCay et al., 2006, p. 106).
Because a goal of health management is to improve wellness and participation, occupational therapy practitioners must examine approaches and advocate for health management on the individual and population levels, including how occupation can be harnessed to support wellness. Although occupational therapy has a long history of promoting health and well-being to support participation (American Occupational Therapy Association, 2008; Arbesman & Mosley, 2012; Leland et al., 2017), the profession has not adequately considered the costs associated with health management.
This multimethod qualitative study explored the sociocultural mechanisms that affect the social participation of young adults after FEP. Study findings are discussed in Fox (2019). This article presents focused findings related to health management with the purpose of challenging conceptualizations of health management occupations as inherently good and to also acknowledge the occupational losses associated with health management.
Method
Through a collaborative ethnographic approach, this study aimed to (1) explore the sociocultural mechanisms that affect social participation for young adults after FEP and (2) explore perceived opportunities for participation for young adults after FEP. Study methods included semistructured interviews, participant observations, and discourse elicitation. Study procedures and confidentiality measures were approved by the institutional review board at the University of North Carolina at Chapel Hill.
Recruitment and Sampling
Recruitment and data collection were conducted by the first author (Valerie Fox). Study recruitment occurred through direct referral by providers and through recruitment flyers posted at local mental health settings and university campuses and in local mental health newsletters. Inclusion criteria required participants to be fluent in English, to be between ages 18 and 30 yr, and to have experienced FEP within the previous 5 yr. Five participants met the study criteria and participated in the study (see Table 1 for demographic information and pseudonyms). Informed consent was obtained from all participants before participation.
Participant Characteristics
Note. F = female; M = male.
Data Collection and Analysis
The first author engaged in two observations per month for 6 mo with each of 4 study participants. A 5th participant engaged in only six observations because of scheduling difficulties. A total of 54 observations occurred. To maximize participant comfort and engagement, participant observations occurred at a time and place chosen by participants. Participants completed two semistructured interviews to explore their experiences of social participation after FEP and to explore how local discourses affected their participation. Participants also engaged in an innovative discourse elicitation method to facilitate discussion regarding underlying sociocultural assumptions that shaped the participation of people with FEP.
To engage in discourse elicitation, participants were asked to bring a sample of local discourse (e.g., image, text, quotation) that exemplified their experiences of FEP and its impact on their participation. The first author also showed participants two images that characterized the first author’s assumptions about FEP and its impact on social participation. This provided an opportunity to explore the researcher’s personal biases with participants and to stimulate further discussion regarding sociocultural forces affecting participation after FEP.
Data collection and analyses occurred iteratively to continuously refine interview questions and explore emerging concepts with participants. Memos were maintained to trace researcher reflections and conceptualizations. Interview transcripts, field notes, and memos were analyzed with ATLAS.ti software (Version 7; https://atlasti.com/) using open and focused coding. The research team, consisting of six experts (including both authors) in the field of occupational science, psychiatry, and anthropology, convened regularly to review coding, identify patterns, and develop thematic findings. Emerging findings were discussed with study participants to check whether they accurately reflected their lived experience. Triangulation of data sources, peer debriefing, and member checking enhanced the credibility of findings.
Results
Study participants described experiencing a liminal space after their FEP. Liminality is a “state of in-between-ness and ambiguity” (Beech, 2010, p. 287). Leo (pseudonym) directly referenced liminality when describing his experience: I’m like in this place right now. This middle space. This liminal space. It’s like an in-between limbo space where I’m not committed to anything really . . . I’m kind of stuck . . . in this place and that’s how I feel. I feel stuck. I’m in the middle of the story where this stuff from my past is still going on but I’m trying to create a new story and I’m stuck in the old story. And it keeps coming up over and over. To where all I have is doctor’s appointments. And the court. . . . And I don’t know how to fix it.
Other participants echoed the notion of liminality, which encapsulated their experiences immediately after their FEP as a transitional space of uncertainty, in which it was unclear whether they could return to their previous mode of participation or achieve previously anticipated goals.
For study participants, the liminal space of FEP was dominated by a need to manage the illness. In this space, the hierarchy of occupational needs shifted as health management occupations took priority over other occupations and habits and routines emerged around an illness identity. Study analyses revealed three themes that constituted and sustained participants’ liminality: (1) hospitalization and illness engulfment, (2) fear of relapse, and (3) locus of control.
Hospitalization and Illness Engulfment
The liminal space of FEP began during participants’ first hospitalization. Four participants reported internalizing the identity of mental illness during their initial hospitalization after FEP. For example, Carly (pseudonym) reported, “Before I left the hospital, I knew something was not right with me.” Oliver (pseudonym) also mentioned that hospitalization altered his self-perception: I don’t spend a day wishing that I hadn’t spent those 2 weeks in jail where no one would drug you or speak to you like you’re a child . . . I feel like if you take people out of their appropriate context and put them in a place like where I was, then labels can get attached to you that shouldn’t be attached to you. . . . And I didn’t like the way in which I talked, the way in which I explained myself was picked apart the way it was.
Oliver referred to the tacit habits and identities that operate within hospital contexts, many of which were involuntarily absorbed before his discharge. Institutional habits included daily visits to ascertain delusional states and analyze speech patterns, 15-min room checks, and shepherding patients to scheduled events. These institutional habits galvanized the identity of “mentally ill patient” for participants, a finding similarly noted by Davidson (2007).
Although participants’ hospitalizations were brief, these experiences had a lasting impact on their adoption of stigmatized identities, how they approached health management, and how quickly they were able to move through the liminal space of FEP to reengage in social occupations. For study participants, reengagement often began with necessary health management occupations, including attending outpatient therapy, managing medication, participating in support groups, and maintaining proper sleep hygiene. The fear of relapse motivated participants to engage in these health management occupations and tended to overshadow other occupations.
Fear of Relapse
Fear of relapse supported health management; however, it also limited engagement in occupations beyond health management. For instance, Leo began to prioritize stability in his occupational choices and avoided previous occupations that he had learned to associate with his FEP: “I guess I’ve emphasized safety over growth.” Leo loved studying languages, writing pen pals, and learning about other countries. After his FEP, he and his parents became preoccupied with the possibility that his language exploration might exacerbate his symptoms and precipitate a relapse. Subsequently, one of Leo’s pen pals helped him challenge that fear and conclude, “This is a part of my personality. I have been learning languages and writing pen pals for 15 years.” Leo became frustrated with doubting himself and worrying about whether his meaningful occupations heightened the risk of relapse. Under the pretext of their illness and the fear of relapse, participants reported feeling suddenly scrutinized for their occupational choices, including their social interactions and the frequency of their participation. Fear of relapse, among both participants and their families, precluded a return to social participation until everyone felt that symptoms were manageable.
Health management occupations to prevent relapse were prioritized over other meaningful occupations during the initial recovery period and sometimes beyond. For example, Leo deferred moving to Japan to teach English so he could focus on getting his health in order. Willow (pseudonym) struggled with prioritizing her participation with friends because of the stress of managing her mental illness: “I don’t participate as much as people normally do . . . I get so overwhelmed about mental illness that I won’t even be thinking about social things. It’s not my priority anymore.” Carly also feared poor symptom management would have a negative impact on her relationships and was hesitant to reengage in social occupations: It took me a year to feel comfortable again. . . . I started going back to my campus ministry events a couple of months afterward. . . . But you have to be real slow about it. . . . When you are recovering from psychosis you don’t want to be around tons of people because you are still vulnerable and you might say weird things and freak them out. . . . I was able to slowly jump back into things and get back to my social life.
Participants’ fear of relapse supported the inclusion of health management occupations into their daily routine; however, it also contributed to the liminal space of FEP and limited their sense of control over their daily occupations.
Locus of Control
Participants’ locus of control affected their investment in health management and movement through the liminal space of FEP. Locus of control refers to how much control a person believes they have over experiences and situations that affect their lives (Harrow et al., 2009). Several participants noted a lack of control over their lives as a result of new demands for outpatient appointments, medications, and family assistance after FEP. Leo grieved his loss of control, which was worsened by his parents’ efforts to help him manage his illness: When I was diagnosed with bipolar disorder and I got labeled mentally ill, my parents spent the next few years telling me I was mentally ill and pushing it into me. And I refused to believe it. I knew I had bipolar disorder, and I took my medicine. But my mom would leave out Bipolar Magazine for me to read. And she wanted me to own this disease. She would say, “You are mentally ill.” And I’m like I didn’t want that identity. Because I wanted to be this superstar that I had been in high school. And I wanted to be excellent. And I wanted to be successful. And I wanted to be this person that was loved and accepted.
BB (pseudonym) attempted to reclaim control by directly opposing external pressures to manage his illness, such as deciding not to engage in health management occupations: “I feel like people are trying to put me in a box but I still try to get out of it a lot. . . . Sometimes I don’t take my meds or something.” Efforts to recover control by challenging external forces are a typical form of resistance for people who are forcefully positioned into the stigmatized identity of mental illness (Thoits, 2011). Although preserving his locus of control, BB’s efforts to avoid recommended health management occupations also prolonged his experience of liminality.
Discussion
As noted earlier, this study was part of a multimethod qualitative study that explored the sociocultural mechanisms that affect the social participation of young adults after FEP. In this article, we presented focused findings describing how health management occupations hindered social participation immediately after FEP. After FEP, managing the illness became a primary occupation. Engagement in this occupation detracted from participation in other social occupations. For example, Leo forewent attending evening Bible study because he believed that his symptoms would worsen if he did not go to sleep by a predetermined time. Participants often deferred the future and limited their occupational pursuits to manage their illness. They reported feeling fear when returning to particular occupations they believed might cause a relapse. Initially, they operated in comfort zones, which often involved environments focused on their mental illness (outpatient clinics, support groups, pharmacies). For some, managing the illness became a full-time endeavor and required reduced social participation in communities of practice, thereby offering fewer opportunities to experience belonging in those communities. They became stuck in this transitional space (i.e., liminal space of FEP), which had a negative impact on their social participation, inclusion, and identity.
Although treatment providers often attribute poor social outcomes (e.g., social isolation, withdrawal) to behaviors associated with having a mental illness, this study suggests that those social outcomes are related to the positional identities forced on patients as they enter the mental health system and seek to manage their illness. It is therefore important for occupational therapy practitioners to help mitigate the negative impact of these positional identities on participation in occupation.
The concept of liminality can support therapists in understanding the phenomenology of FEP, including how to support health management and social participation after FEP. To describe the experience of liminality, Turner (1967) introduced a framework that suggests that people transition among three phases: (1) separation, (2) liminality or transition, and (3) incorporation. According to Turner, the separation phase occurs at a fixed point marked by a cultural event or change in social structure. Once separated, a person assumes an ambiguous identity; this state of in-betweenness is the liminal phase. Reflection and transformation can occur during this state of detachment and uncertainty. In the third phase, incorporation, a person’s identity is reshaped and a new role in society is adopted. Turner’s three-phase framework is applicable to the experience of FEP and highlights the role of occupation in moving people through liminal spaces (Figure 1).
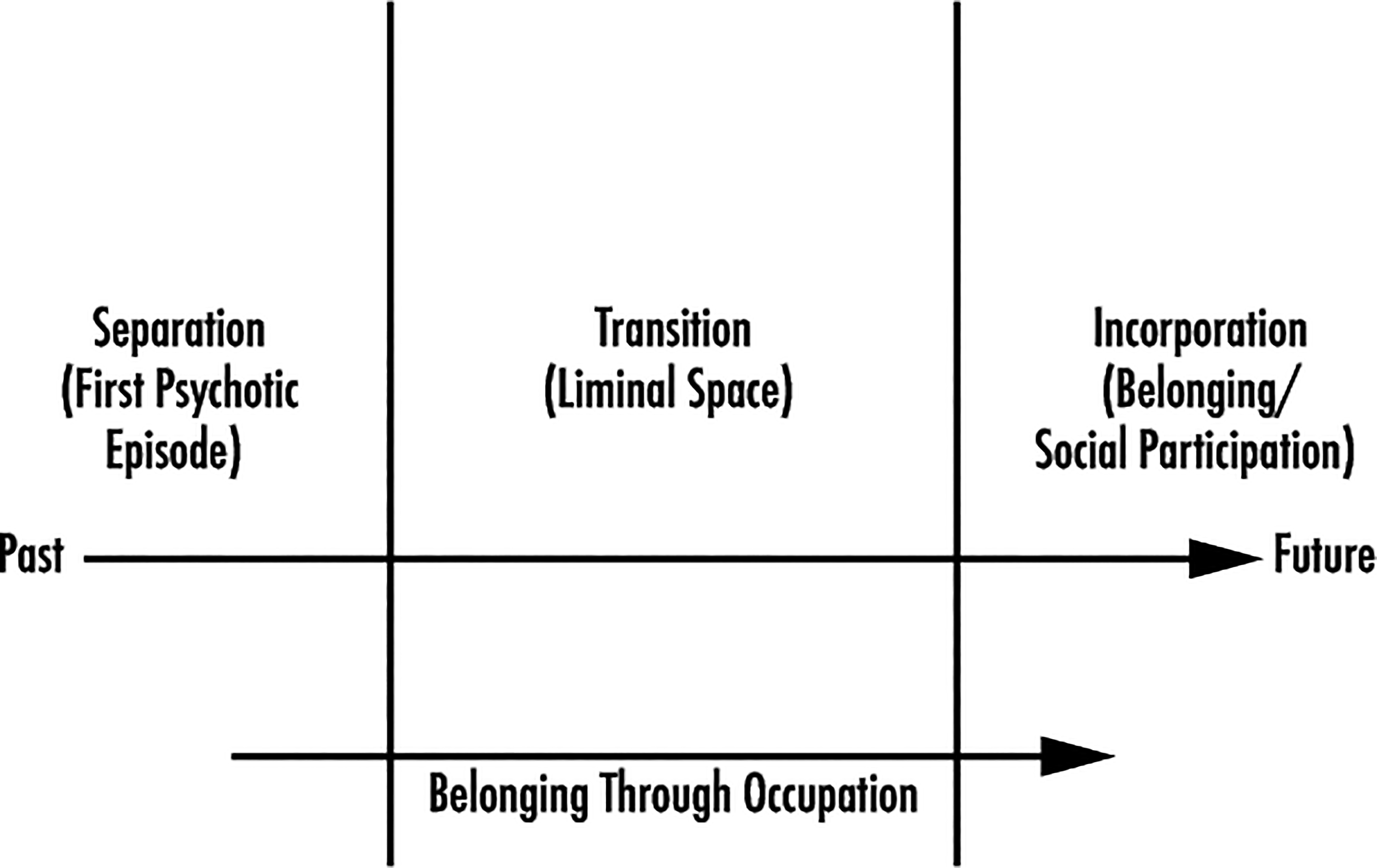
Liminal space of FEP: belonging through occupation.
The separation phase occurs when people experience FEP. At this moment, study participants experienced unfamiliar events, detached from prior identities and self-perceptions, and were unsure how to effectively integrate their experiences with their cultural and societal contexts. Participants then moved into the liminal space of FEP, marked by their initial hospitalization experience; they adopted occupations needed to manage their illness and reevaluated life trajectories. The liminal space of FEP became a sticking point for participants who were overwhelmed by the need to manage the illness. These participants deferred their future plans to devote their time and energy to health management at the expense of other occupations that may previously have contributed to mental health and well-being. During this stage, occupational therapists can assist adults with FEP in finding meaningful forms of participation that account for new health demands and help them transition out of liminality. Ensuring that clients sustain meaningful forms of participation that support a positive identity may help them to navigate their liminality to find stability and meaning beyond mental illness and health management occupations.
The third phase involved reintegration into social occupations. Participants identified alternative life trajectories that fit with their experience and personhood after FEP. Participants who were able to progress through the liminal space to Phase 3 effectively managed their illness and imagined alternative avenues for belonging. Sustained engagement in prior occupations and communities of practice during the liminal phase helped participants progress into the incorporation or belonging phase. Participation in communities outside of mental health treatment also supported movement through the liminal space of FEP. This study supports viewing occupation as a means through which people with FEP move through the liminal space of FEP. The occupations embraced during the liminal phase can have a significant impact on the incorporation stage, in which a new identity and societal role emerge. Occupational therapists working with clients after FEP can play an important role in helping them to reimagine their life trajectories to develop new identities, enhance their recovery, experience belonging, and find opportunities for meaningful participation.
Limitations
The small size and lack of diversity in the sample may limit application of the findings to broader clinical applications. The time required to engage in study procedures may have limited people’s willingness to participate and discouraged participation by those with unmanaged symptoms of FEP. Last, the researchers’ background and ongoing clinical work with clients with mental illness shaped their perspectives and may have allowed ideas and assumptions relevant to the findings to be overlooked. However, ongoing consultation occurred with the research team to recognize biases and minimize their impact on the analyses.
Implications for Occupational Therapy Practice
Health management occupations are vital to recovery and well-being, yet overemphasizing health management can hinder social participation and quality of life. Occupational therapy practitioners can support clients to transition through liminal spaces after diagnosis to envision new life trajectories while ensuring that these transitional spaces are opportunities for growth and recovery. The findings of this study suggest the following recommendations for occupational therapy practice: Explicitly acknowledge the benefits and drawbacks to health management occupations, including how they limit participation in other life domains after initial diagnosis. Use task analysis to examine health management activities and identify ways to reduce treatment burden after diagnosis. An extended period of time in a liminal space dominated by illness management can contribute to a state of chronicity in which clients feel stuck. Assist clients with FEP to envision a future life trajectory that is feasible and matches their health demands and social environments. Help clients find communities for belonging outside of a focus on their mental health.
Conclusion
This qualitative study explored the sociocultural factors that affect the social participation of young adults with FEP. Study findings revealed that the need to engage in health management hindered social participation immediately after FEP as participants’ occupational priorities shifted to managing their illness. Participants reported transitioning through liminal spaces as they negotiated new life trajectories. Although this study concerns experiences of liminality associated with FEP, concepts of liminality can help occupational therapy practitioners understand how their clients transition to new patterns of participation after a new diagnosis or health change. This study provides a framework for reflecting on participation patterns and assisting clients with incorporating health management occupations into other desired routines and occupations.
Footnotes
Acknowledgments
A special thank you to members of Valerie Fox’s dissertation committee who provided their expertise and mentorship throughout the research process. In addition, thank you to the Society for the Study of Occupation for the student grant funding used to support this study. Last, continued thanks to partners and family for their ongoing support and encouragement.