
Abstract
This review identifies the factors influencing the occupational adaptation of people living with FM and highlights the importance of considering those factors while caring for people with FM.
Fibromyalgia (FM) is a common chronic pain disorder that affects as much as 6.6% of the world’s population (Marques et al., 2017). Pain is the main symptom, but fatigue and nonrestorative sleep are also common (Clauw, 2014; Fitzcharles et al., 2013; Mease et al., 2009). People with FM commonly present with a range of problems, including neurocognitive disorders, such as difficulties related to memory and mood disorders (mainly depression or anxiety); pain-related symptoms (e.g., migraine or irritable bowel); and other non–pain-related symptoms (e.g., sexual dysfunction and vulnerability to posttraumatic stress disorder; Clauw, 2014; Fitzcharles et al., 2013; Orellana et al., 2008). FM can have a negative impact on people’s lives, affecting their capacity to perform various occupations (Arnold et al., 2008; Wuytack & Miller, 2011). Living with FM disrupts occupations including work, studies, social relationships, leisure, and domestic chores (Arnold et al., 2008). Some people quit their job or modify it to fit their symptoms (Arnold et al., 2008; Briones-Vozmediano, 2017; Sallinen & Mengshoel, 2019; Wuytack & Miller, 2011).
Kielhofner’s (2008) Model of Human Occupation (MOHO) can be used to understand the interaction between FM and occupation. MOHO is an occupation-focused framework that aims to explain aspects of engaging in occupations and how illness- and disability-related problems arise. MOHO is client centered, evidence based, and holistic in nature. It conceptualizes factors related to being, acting, and becoming that influence occupational adaptation and guides occupational therapy practice. Occupational adaptation occurs when people adapt to a situation (such as living with FM) and build a positive response according to what they are and want to be (occupational identity) and what they want to realize (occupational competence; Kielhofner, 2008).
To our knowledge, only two studies have explored the concepts of identity and occupational adaptation. Briones-Vozmediano (2017) conducted qualitative interviews in a sample of 13 women and 3 men (ages 24–61 yr) to study their social construction of FM and reported that people with FM try to keep up their daily routine to maintain their identity. In a qualitative study using a narrative approach, Sallinen and Mengshoel (2019) explored the impact of FM on daily life with a sample of 5 men, with a specific interest in the ability to work. Every participant’s experience was different; 4 participants adapted their life to the illness, and 1 felt imprisoned by it.
Although some studies have explored certain components of occupational adaptation, there is, to our knowledge, no existing literature review describing the complex phenomenon of occupational adaptation among people with FM. Having a complete picture of this phenomenon would enable better identification of the characteristics that facilitate the emergence of positive occupational adaptation. The aim of this systematic review was to understand the occupational adaptation process of people living with FM. Specifically, the objectives of the review were to understand how the occupational adaptation of people with FM is influenced by (1) personal characteristics, (2) environmental characteristics, and (3) occupational identity and occupational competence.
Method
Study Design
A systematic review of the literature was performed following the recommendations in the Joanna Briggs Institute Reviewers’ Manual 2014 (Peters et al., 2015). The systematic review with thematic synthesis was conducted using the specific method developed by Thomas and Harden (2008). This method is used to gather and integrate the qualitative results of multiple studies (Thomas & Harden, 2008). This systematic review complies with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Moher et al., 2009).
Eligibility Criteria
French and English qualitative studies were included if they documented occupational aspects of the lives of people with FM. Qualitative results of mixed-method studies were also included. Studies were excluded if they reported (1) only the effect of an intervention and not the specific characteristics that influence occupational adaptation and (2) results related to several medical conditions without clearly presenting the FM-related results.
Sources and Search Strategy
English or French articles published before September 2020 were searched in the AMED, CINAHL, MEDLINE, OTseeker, OTDBASE, and PsycINFO databases using a search strategy developed with two librarians. The strategy contained keywords and synonyms related to FM and occupation ([occupational OR OT] OR [“activit* N3 daily”] AND [fibromyalgia* OR fibromyiositis] search in title or abstract). Dissertations and theses were searched in the Sherbrooke University’s discovery tool, on the website Portail Thèses Canada, and in ProQuest Dissertations and Theses. We also searched Google with the keywords fibromyalgia and occupation. Authors of the articles included in the database search were contacted to obtain unpublished work or other articles on the subject. The reference lists of the relevant studies were also searched for additional studies.
Study Selection
The references were imported into Zotero (https://www.zotero.org/download/), and duplicates were removed. Two authors (Andréa Dépelteau and Émilie Lagueux) first screened titles and abstracts to remove clearly ineligible articles. They then assessed the full text of the articles for inclusion criteria and reached consensus on any disagreements. A third reviewer (Catherine Hudon) was consulted in case of disagreement.
Data Collection Process and Study Appraisal
Dépelteau collected descriptive data on authors, year of publication, country, aim of the study, sampling procedure, data collection strategy, and main results. Article quality was assessed by Dépelteau and Raphaël Pagé using the Critical Appraisal Skills Programme (2018) checklist for qualitative research, and all the “yes” scores were tallied. We considered articles meeting one to three criteria to be of low quality; three to six criteria, medium quality; and seven to nine criteria, high quality. To consider the relative contribution of each individual study according to defined criteria, we performed a sensitivity analysis to assess the impact of lower quality articles on the results (Carroll & Booth, 2015). After the synthesis, we examined each of the themes mentioned in the lower quality articles to evaluate their impact on the results.
Synthesis of Results
After data extraction, two authors (Dépelteau and Pagé) independently coded all study result sections line by line using Microsoft Office Word 2007. The initial coding was done on the basis of the MOHO (deductive coding; Kielhofner, 2008), and new codes were also added (inductive coding; Fereday & Muir-Cochrane, 2006). The authors discussed their coding afterward to build a final coding list. The final coding list was presented and discussed in a team meeting by all authors. A group of experts was consulted to discuss the results of the analysis. The analysis process was iterative; the research team went back and forth between the data and the results. We wrote memos regarding our feelings, judgments, or ideas during the analysis process to consider our role and potential bias.
Results
Study Selection
Of the 560 identified articles, 347 remained after duplicates were removed. Titles and abstracts were screened, and 303 articles were excluded because they did not meet the selection criteria. The full text of the 44 remaining articles was assessed; 12 articles matched the selection criteria and were included in the review (Figure 1).
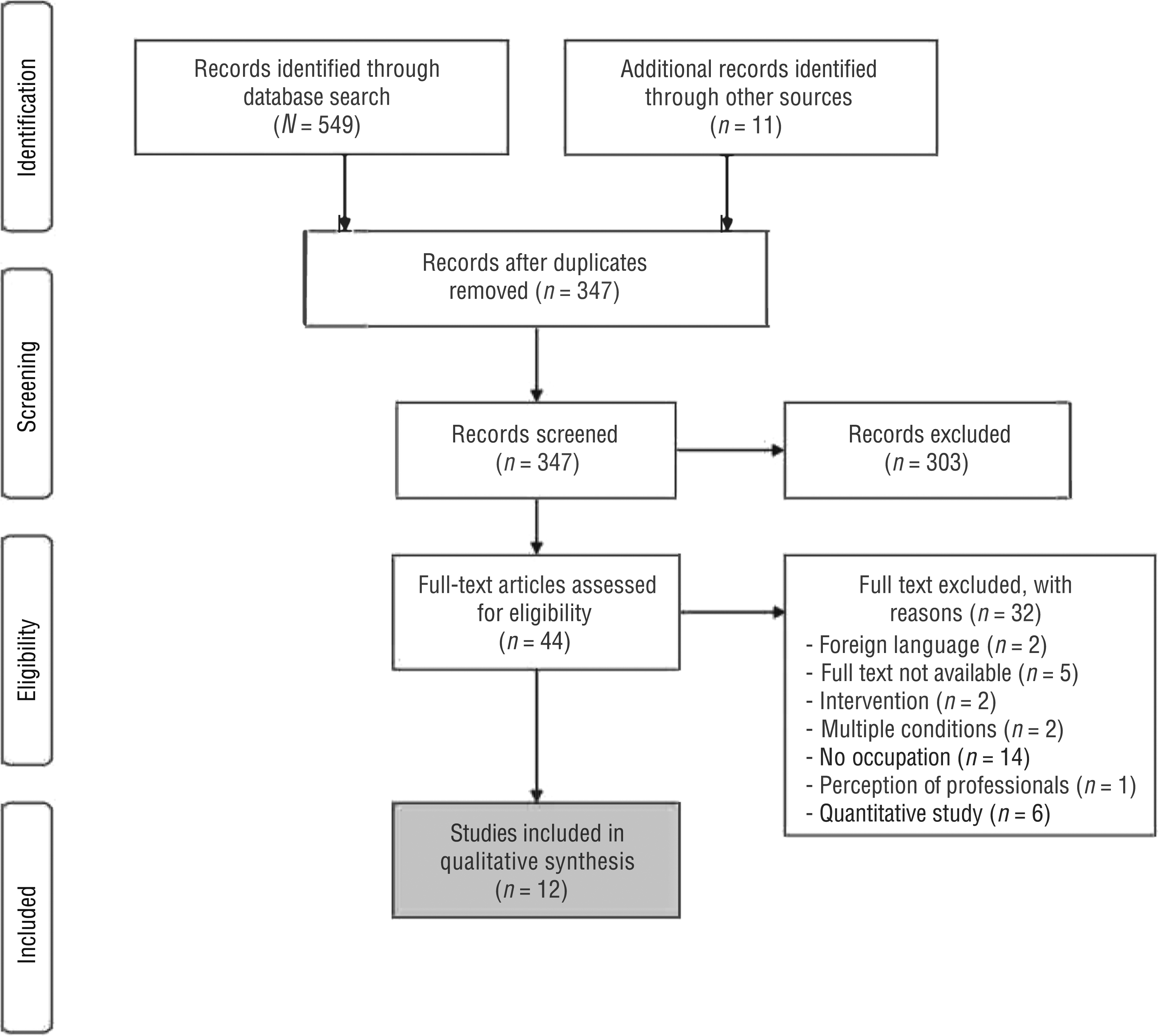
Flow of articles through the systematic review process.
Characteristics of Included Studies
The characteristics of the included studies are presented in Table A.1 in the Appendix. Two studies were conducted in Sweden (Liedberg & Henriksson, 2002; Liedberg et al., 2004) 1 in Sweden and the United States (Liedberg et al., 2006), 2 in Spain (Briones-Vozmediano, 2017; Briones-Vozmediano et al., 2016), 2 in the United States (Arnold et al., 2008; Zdravecky, 2003), 1 in Canada (Busch, 2005), 1 in the United Kingdom (Wuytack & Miller, 2011), and 3 in multiple countries (Sallinen & Mengshoel, 2019; Stamm et al., 2014; Theadom & Cropley, 2010). Total sample size varied from 3 to 94 participants. The study samples of Briones-Vozmediano et al. (2016) and Briones-Vozmediano (2017) cross over. The mean age of the participants ranged from 32 to 54 yr. One study focused on men, and the other studies recruited 81% to 100% women. Two used a phenomenological approach (Theadom & Cropley, 2010; Wuytack & Miller, 2011), and 1 used a grounded theory approach (Busch, 2005). The 9 other studies did not specify the design of the qualitative research (Arnold et al., 2008; Briones-Vozmediano, 2017; Briones-Vozmediano et al., 2016; Liedberg & Henriksson, 2002; Liedberg et al., 2004, 2006; Sallinen & Mengshoel, 2019; Stamm et al., 2014; Zdravecky, 2003).
The quality assessment conducted using the Critical Appraisal Skills Programme (2018) checklist is presented in Table A.2. Ten articles were deemed to be of high quality (Arnold et al., 2008; Briones-Vozmediano, 2017; Briones-Vozmediano et al., 2016; Busch, 2005; Liedberg & Henriksson, 2002; Liedberg et al., 2004, 2006; Sallinen & Mengshoel, 2019; Theadom & Cropley, 2010; Wuytack & Miller, 2011), and 2 were deemed to be of medium quality (Stamm et al., 2014; Zdravecky, 2003).
Synthesis of Results
The results are divided into four broad themes: (1) personal characteristics influencing participation and occupational adaptation, (2) environmental characteristics influencing occupational adaptation, (3) occupational identity and occupational competence influencing occupational adaptation, and (4) occupational adaptation: a dynamic process.
Personal Characteristics Influencing Participation and Occupational Adaptation
A person’s characteristics and occupations are closely linked because an action depends on the person to do it. Motivation is a prerequisite as well as a guide to take part in and choose occupations. However, FM symptoms affect motivation: “Participants found it difficult to become motivated to begin tasks because the constant presence of pain disrupted patients’ concentration and depleted them of energy” (Arnold et al., 2008, p. 118). Individual interests guide the choice of an occupation, but FM can also lead to a loss of interest for some people. For instance, 1 article explained that a participant “experienced a decrease in her interests and described no longer being as social as she used to be” (Zdravecky, 2003, p. 56). Finally, the importance that a person gives to an occupation also influences its practice.
Time-consuming activities, such as work, are associated with having an organized routine. Maintaining a routine seems important for people with FM: “Maintaining routines and habits that structure everyday life was regarded as important by the women. Work is an important part of this organized structure” (Liedberg & Henriksson, 2002, p. 268). Routines are made up of different roles, such as worker, parent, and lover. Experiencing FM affects these roles: “The men expressed their disappointment for not being able to be the father or husband; they wanted to be or had been before the onset of symptoms” (Sallinen & Mengshoel, 2019, p. 425).
The studies report a lot of negative feelings, often naming frustration, shame, the perception of being useless, and guilt. These feelings were most often related to the inability to take part in daily activities, to not having a diagnosis, and to the social environment’s lack of understanding. For instance, an article about the social construction of FM by people living with FM said, “Not to carry out these duties [caring for family members and doing housework] brings on feelings of guilt only in the case of the women” (Briones-Vozmediano, 2017, p. 8). Some studies highlighted the benefits of certain positive character traits that lead to more positive feelings; for example, “Key factors said to be responsible for a progress to more satisfactory but modified future hopes were personal strength and perseverance” (Wuytack & Miller, 2011, p. 6).
The onset of FM symptoms can directly affect the skills and performance of daily activities, which reduces participation. FM impairs work, studies, social relationships, leisure, and domestic chores: “Patients reported disrupted relationships with family and friends, social isolation, reduced activities of daily living and leisure activities, avoidance of physical activity, and loss of career or inability to advance in careers or education” (Arnold et al., 2008, p. 114). It takes more time to carry out an activity, and performance is reduced compared with the past. For instance, a participant said, “I need so much time for brushing my teeth, for dressing myself, there are the fingers, the feet and everything else [the other body parts]” (Stamm et al., 2014, p. 30). The unpredictability of symptoms makes it difficult for people with FM to plan activities. The need to focus on one day at a time came out in one study: “The women in this study said that the unpredictability of their symptoms obliged them to live on a day-to-day basis[,] making it difficult to plan” (Wuytack & Miller, 2011, p. 6).
Environmental Characteristics Influencing Occupational Adaptation
Most of the studies reported the negative influence of FM on the social environment. Many people experiencing FM explained that their relatives’ attitude made them feel misunderstood: “Husbands of women with FM may criticize and blame their wives for an untidy house, or allude to the fact that they have been at home all day doing nothing, which makes women with FM feel deeply misunderstood” (Briones-Vozmediano et al., 2016, p. 844). Changes in the way a family functions seem inevitable, and the situation of the person with FM becomes a family matter. Life partners are directly involved in this process, and FM has an impact on social environment: “Husbands or partners also have to adapt to their loved one’s new situation” (Briones-Vozmediano et al., 2016, p. 845). Many studies mentioned the decrease in social support and the loss of friends. One study stated, “Both US and Swedish women said that they . . . had lost friends since their problems started, both in their private life and work” (Liedberg et al., 2006, p. 1181). Difficulties with taking part in certain activities limited the opportunities to maintain relationships. Even when there are difficulties related to social life, relatives’ support is key for people with FM: “The support and understanding expressed by the family members were seen as essential in terms of managing the daily life and coping . . . despite the illness” (Sallinen & Mengshoel, 2019, p. 425).
Work environment (both social and physical) is a key component influencing the ability to stay at work or not. Opportunities, resources, demands, and constraints of the work environment can influence the desire to stay at work. When a person perceives that adaptation of the workplace is not possible (the opportunities and resources cannot fit the demands and constraints), it is difficult to remain at work: “Despite the love for their job and the struggle to accept their leave, most participants had reconciled themselves to stop working permanently as they perceived a return to their job [to be] impossible” (Wuytack & Miller, 2011, p. 4). Therefore, having support at work is a facilitator for remaining at work. In a study of the factors influencing the work situation, a participant highlighted that the support of staff and superiors plays a big role in the decision to return to work (Liedberg & Henriksson, 2002, p. 270).
The ignorance and lack of understanding of FM in society can influence the support received by people living with the illness. Studies reported this with respect to society in general, but also with respect to health care practitioners: “The doctor–patient relationship is described by patients as unsatisfactory mainly due to the lack of empathy and understanding recognized by their healthcare providers” (Briones-Vozmediano, 2017, p. 7). A participant in a study focusing on the lived experience of FM highlighted the importance of support from other FM patients in the feeling of being understood: “That is the nice thing about meeting in a self-help group, you don’t have to explain and justify yourself all the time” (Wuytack & Miller, 2011, p. 6).
Occupational Identity and Occupational Competence Influencing Occupational Adaptation
The onset of FM may alter people’s identity because it can affect self-image. For some people, the symptom-related changes in their body do not match their vision of themselves: “It’s as if my body is not a part of myself, I have to put everything together” (Stamm et al., 2014, p. 30). Living with FM is explained as an existential breakdown. People with FM had to redefine their identity: “The women in this study communicated an existential breakdown arising from their life-sapping disabilities. . . . Restructuring their identity was considered a struggle but crucial to regain contentment in life” (Wuytack & Miller, 2011, p. 5). Another study described the identity breakdown as a conflict between being ill and carrying out activities of daily living (Briones-Vozmediano, 2017, p. 1). Time-consuming occupations such as work and family involvement are strongly related to identity. People with FM seem to have difficulty achieving occupational identity because they struggle to be who they want to be and do not recognize themselves in their current situation. Therefore, health practitioners’ recommendations should take identity into consideration.
Occupational competence also seems to be greatly affected by FM. People with FM struggle to maintain a routine with meaningful occupations. Some people feel that they cannot take part in some of their previous activities and have difficulty balancing their life: “They [the nonworking women] mention the conflict between different roles and the difficulties of managing both household activities and work” (Liedberg & Henriksson, 2002, p. 271). However, achieving some activities led to positive feelings: “The undertaking of household chores gives them [the women] a sense of satisfaction and achievement” (Briones-Vozmediano et al., 2016, p. 841). Being at work was an important part of most participants’ routine. However, in the absence of work, maintaining some structure is possible: “A few women have managed to maintain some activities and a structured day even if they no longer have a work role. One woman mentions that she cooks for others and assists lonely, older people” (Liedberg & Henriksson, 2002, p. 268). Staying active remains a key element.
Occupational Adaptation: A Dynamic Process
Occupational adaptation results from the interaction of all personal, environmental, and occupational components. It is unique and has to be assessed for each person. Most articles presented strategies used to reach occupational adaptation. Many cited the use of self-management strategies to manage pain and energy. Maintaining meaningful roles, even if adjustments were made, was found to be beneficial to people with FM: “To be able to carry on working in a job adapted to their needs is of benefit to patients, depending on the degree of handicap involved, this being the case for both the women and men who were interviewed” (Briones-Vozmediano, 2017, p. 8). Because the onset of symptoms is unpredictable, participants needed to adapt their routines to carry out these roles. Being able to constantly reevaluate and balance activities was a good way to manage life with FM: “To manage their symptoms and engage in everyday activities, participants described the need to plan and pace their activities, including rest periods throughout the day” (Theadom & Cropley, 2010, p. 1942). The article by Sallinen and Mengshoel (2019) addressed the fact that some people are able to adjust their life to match the illness, and some others seem to struggle with it. One study also mentioned that people with FM sought nonpharmacological treatments: “Each of the participants described wanting more for treatment than prescription drugs” (Zdravecky, 2003, p. 52). Occupational adaptation is a dynamic process that needs to be addressed from a patient-centered perspective.
Sensitivity Analysis
A sensitivity analysis was not required because no low-quality articles were included.
Discussion
This review explored the occupational adaptation process of people living with FM. The results highlight that support from relatives is essential to adapting to FM. Because relationships are affected by multiple causes (FM symptoms, interactions between symptoms and daily activities, social environment), social support was identified as a potentially important modifiable factor to promote occupational adaptation. FM affects occupational competence, and people with FM thus need to redefine their identity. Finally, occupational adaptation is achieved by maintaining meaningful roles and applying several management strategies. Occupational adaptation is a challenge for some people, and this dynamic phenomenon needs to be assessed specifically for each client.
Our review reveals that social environment is an important factor to consider in occupational adaptation. Support from relatives appears to be crucial to achieving positive occupational adaptation, especially considering that having positive relationships with relatives seems to be an issue for some people living with FM. In an online survey completed by 6,126 adults diagnosed with FM that explored the impact of FM on relationships with relatives (Marcus et al., 2013), half of the respondents indicated that they were not satisfied with their current partner relationship and that experiencing FM had mildly to moderately damaged their relationship with their life partner. Moreover, a minority of respondents indicated that having FM had a negative impact on their relationships with close friends and children (Marcus et al., 2013). In addition, although the survey did not ask participants about relationships with health care providers, several participants used the space allotted for open-ended responses to discuss this issue. They indicated, in accordance with the results of our review, that health care providers often lack understanding and respect, even though this relationship should be a supportive one that helps the person with FM adapt positively.
Fitzcharles et al. (2013) published guidelines for the management of FM and stated that “healthcare professionals should be educated regarding the pathogenesis of fibromyalgia, empathetic, open, honest, should not demonstrate negative attitudes, and should practice shared decision-making” (p. 15). Therefore, it seems important that health professionals reflect on their beliefs about FM and attitudes toward people with FM to establish a positive therapeutic relationship with them. Our review highlights the main social environmental barriers and facilitators that health care professionals should examine to support their clients’ adaptation to FM. Physical environment was infrequently discussed in the studies included in our review, but health care professionals should explore it with clients to obtain a complete picture of the situation.
In the MOHO, the concept of identity is mainly related to occupation. Occupational identity represents who a person is and who they want to become as an occupational being (Forsyth & Kielhofner, 2011). However, in many studies, the concept of identity went beyond the sole concept of occupation to embrace a broader perspective of self. For example, having a diagnosis was intimately linked to the development of identity (Arnold et al., 2008, Sallinen & Mengshoel, 2019; Wuytack & Miller, 2011; Zdravecky, 2003). The diagnosis makes sense of the subjective experience of FM. Poor recognition of FM often results in delays in diagnosis (Fitzcharles et al., 2013). Finally, receiving a diagnosis was often a relief after a time of uncertainty and frustration. Therefore, early diagnosis by the primary care physician is crucial to allow people with FM to develop their new identity and to help them maintain or improve their function (Fitzcharles et al., 2013).
Occupational competence was mostly related to the control of symptoms. Symptom control is achieved by applying strategies to manage energy, pain, and time use. Because the development of management strategies seems to support occupational adaptation to FM, clients should be guided in the development of effective life strategies. A manualized occupational therapy intervention that can contribute to the occupational adaptation of people with chronic pain is Lifestyle Redesign® (Uyeshiro Simon & Collins, 2017), an occupational therapy intervention that facilitates the development of healthy routines to prevent and manage chronic conditions. Lifestyle Redesign includes the use of treatment topics or modules (e.g., identifying current roles, habits, values, time management, socialization to prevent social isolation, and dealing with changing occupational identity) to promote clients’ education about their health through occupation and through the implementation of behavior changes in daily routines (Clark, 2015; Uyeshiro Simon & Collins, 2017). This intervention is an example of the type of occupational therapy services to offer people with FM to support them in positive occupational adaptation.
Estévez-López et al. (2017) recently conducted a cross-sectional study of 486 people with FM (95.1% women) that focused on adaptation to FM through physical and psychological functioning. They recognized that the experience of FM is heterogeneous and that multiple factors such as resilience and lifestyle can influence it. They identify five profiles of people with FM (adapted, fit, poor performer, positive, maladapted) and eight modifiable factors related to psychological and physical function. The psychological factors are psychological distress, resilience, catastrophizing, and declarative memory, and the physical factors are fatigue, active lifestyle, objective fitness, and subjective fitness (Estévez-López et al., 2017). The adapted profile represents a person with better adaptation to both psychological and physical factors, and the maladapted profile represents the opposite. These modifiable factors can be targeted in therapy. Our review also identified multiple factors related to occupational adaptation that should be considered as barriers or facilitators, such as negative feelings, support from the social environment, and identity breakdown. Both the Estévez-López et al. (2017) study and our review reveal factors that should be considered in working with people with FM. However, our review shows that it is important to consider more than personal characteristics; environmental characteristics, occupational identity, and occupational competence should also be considered. We believe that consideration of the barriers and facilitators identified in this review could help occupational therapy practitioners better understand the interactions among the components that influence people’s experience of FM.
Strengths and Limitations
In conducting this review, we rigorously followed the method proposed by Thomas and Harden (2008). Credibility was enhanced throughout the process by triangulation between researchers and by consideration of the researchers’ subjectivity (Laperrière, 1997). Transferability was facilitated by the in-depth description of the sample (Laperrière, 1997). However, it is important to consider the differences that may arise from the cultural context in which each study was conducted.
This study also has limitations. Although the research strategy was developed with a specialist, we may have missed some studies. We limited this by searching the gray literature and the reference lists of the included studies. Some studies did not provide detailed information about methods. The quality assessment of the included studies took this issue into consideration. Finally, it is important to note that a secondary analysis of the data was performed and that the included studies were not designed to answer the research question about occupational adaptation.
Implications for Occupational Therapy Practice
The results of this systematic review have the following implications for occupational therapy practice:
Building a positive occupational identity allows people with FM to identify which occupations define them rather than being defined only by FM.
Regaining control over FM by learning strategies to manage energy, pain, and time use can increase occupational competence.
Support from the people in one’s social environment is essential to enable occupational adaptation, and occupational therapists should consider this support in the intervention process. With their holistic approach, occupational therapy practitioners can integrate the social environment into their interventions because they address multiple components of people’s lives.
Occupational adaptation is a dynamic process; to enable occupational adaptation, occupational therapists should develop and use evidence-based interventions that address all components of the process.
Conclusion
The results of this systematic review demonstrate the importance of considering the components of occupational adaptation in caring for people with FM, especially in assessing the impact of FM on identity and occupational competence. Future studies could identify key interventions to apply in practice to minimize the barriers identified in this review and maximize the facilitators. An interesting approach could be to develop an algorithm to guide practitioners on what to do when clients present with a particular barrier or facilitator.
Supplemental Material
Supplementary material for Occupational Adaptation of People Living With Fibromyalgia: A Systematic Review and Thematic Synthesis
Supplementary material, sj-doc-1-aot-10.5014_ajot.2021.047134.doc for Occupational Adaptation of People Living With Fibromyalgia: A Systematic Review and Thematic Synthesis by Andréa Dépelteau, Émilie Lagueux, Raphaël Pagé and Catherine Hudon in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We acknowledge Kathy Rose for her invaluable help in developing rigorous search strategies and Bonita Van Doorn for editorial review. This project was funded by the Fonds de Recherche du Québec en Santé.
Appendix. Evidence and Risk-of-Bias Tables for the Systematic Review
Quality Assessment of the Studies Included in the Systematic Review
| Author/Year | Was There a Clear Statement of the Aims of the Research? | Is a Qualitative Methodology Appropriate? | Was the Research Design Appropriate to Address the Aims of the Research? | Was the Recruitment Strategy Appropriate to the Aims of the Research? | Was the Data Collected in a Way That Addressed the Research Issue? | Has the Relationship Between Researcher and Participants Been Adequately Considered? | Have Ethical Issues Been Taken Into Consideration? | Was the Data Analysis Sufficiently Rigorous? | Is There a Clear Statement of Findings? |
| Arnold et al. (2008) | Y | Y | CT | Y | Y | N | Y | Y | Y |
| Briones-Vozmediano (2017) | Y | Y | CT | Y | Y | N | Y | Y | Y |
| Briones-Vozmediano et al. (2016) | Y | Y | CT | Y | Y | N | Y | Y | Y |
| Busch (2005) | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Liedberg et al. (2006) | Y | Y | CT | Y | Y | N | Y | Y | Y |
| Liedberg & Henriksson (2002) | Y | Y | CT | Y | Y | N | Y | Y | Y |
| Liedberg et al. (2004) | Y | Y | Y | Y | Y | N | Y | Y | Y |
| Sallinen & Mengshoel (2019) | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Stamm et al. (2014) | Y | Y | CT | Y | Y | N | Y | Y | N |
| Theadom & Cropley (2010) | Y | Y | Y | Y | Y | N | Y | Y | Y |
| Wuytack and Miller (2011) | Y | Y | Y | Y | Y | N | Y | Y | Y |
| Zdravecky (2003) | Y | Y | CT | N | Y | CT | Y | Y | Y |
Note. CT = can’t tell; N = no; Y = yes. Quality assessment tool adapted from CASP Qualitative Checklist, by Critical Appraisal Skills Programme, 2018. https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf
Suggested citation: Dépelteau, A., Lagueux, E., Pagé, R., & Hudon, C. (2021). Occupational adaptation of people living with fibromyalgia: A systematic review and thematic synthesis (Table A.2). American Journal of Occupational Therapy, 75, 7504190040. https://doi.org/10.5014.ajot.2021.047134
*
Indicates article included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.