
Abstract
Occupational therapy programs have an important role to play in intervening with students’ assumptions about disability
Occupational therapy is defined in the Occupational Therapy Practice Framework: Domain and Process (4th ed.; American Occupational Therapy Association [AOTA], 2020b, p. 1) as “the therapeutic use of everyday life occupations with persons, groups, or populations (i.e., the client) for the purpose of enhancing or enabling participation.” Occupational therapy often works with biomedical and rehabilitative models (Cole & Tufano, 2008) to address client factors stemming from impairments during person-level direct service delivery. These approaches view disability as located within the person, requiring the practitioner to fix or cure the person. However, over the last 2 decades, the field of occupational therapy has acknowledged critiques from the disability community of the negative impact of interventions driven by locating disability solely within the person (Kielhofner, 2005; Phelan et al., 2014).
Literature from disability studies, often seen as the academic arm of the disability rights movement, provides a counterpoint to the medicalized perspectives on disabilities emanating from the applied fields, such as rehabilitative medicine (Linton, 1998). Occupational therapy practitioners’ commitment to client-centered practice and increasing attention to the profession’s social justice roots (Frank, 2012) align well with concepts from the Social Model of Disability, a prominent model within the field of disability studies. This model locates the creation of disability in the presence of social barriers that affect occupational participation and performance (Kielhofner, 2005; Magasi & Hammel, 2009).
Practitioners and educators are challenged to focus on optimizing individual capacity and independence while evaluating the “larger world in which the person lives” (Magasi, 2008, p. 613), which may demand embracing social interdependence as a valued outcome of clinical intervention (AOTA, 2020b). This outlook exposes the dualistic influences of the medical and social approaches to disability within occupational therapy. Although this viewpoint reflects the foundation that has been laid since the beginning of the century and the need for continued growth, the strongly embedded medical approaches also drive reimbursement in hospitals and clinical settings where a majority of occupational therapy practitioners work (AOTA, 2015; Howard, 1991). As a result, discourses that permeate much of the classic occupational therapy literature and that are found in curriculum syllabi perpetuate the more medical model view of disability (Phelan et al., 2014).
Disability Attitudes and Occupational Therapy Education
Occupational therapy curricula can influence attitudes and behaviors that inform how students think about disability, interactions with clients, and the focus of the interventions. People’s attitudes operate on two different levels: explicit and implicit (Amodio & Mendoza, 2011). Explicit attitudes are conscious attitudes, whereas implicit attitudes are unconscious attitudes. Explicit measures do not capture all attitudes because people may be unaware that they hold biased attitudes, or they may feel pressure to conceal their biases because of social desirability (Amodio & Mendoza, 2011). In contrast, implicit attitudes can be useful to examine learned associations and internalization of society’s prejudice (Amodio & Mendoza, 2011). Because of the differences in how they operate and because of response bias (regardless of whether it is intentional), it is common for people’s explicit and implicit attitudes to not align.
Despite the differences between explicit and implicit biases, most research about occupational therapy students’ disability attitudes has focused exclusively on explicit attitudes. In fact, there is a dearth of research on occupational therapy and other allied health professional measures of implicit bias across disenfranchised groups. The research on explicit bias that does exist has also often resulted in conflicting findings. For example, Sullivan and Mendonca (2017) found that Level II fieldwork, compared with 2 yr of coursework, significantly improved students’ explicit attitudes toward people with intellectual disability. In another study, Penny et al. (2001) found that coursework lowered occupational therapy students’ explicit bias toward people with mental illness; however, after Level I fieldwork, students’ negative attitudes toward mental illness significantly increased. Conversely, Lee et al. (1994) found that participation in professional education across years in a curriculum had a positive impact on reducing students’ biased disability attitudes that were maintained during fieldwork experience.
In a systematic review of the literature on attitudes of health care students, including occupational therapy students, toward people with disabilities (PWDs), student attitudes became more favorable from Year 1 to Year 4 of professional education (Satchidanand et al., 2012). Lee et al. (1994), Tervo et al. (2004), White and Olson (1998), and Satchidanand et al. (2012) found that occupational therapy students’ explicit biases were lower than those in other professional programs; however, Lyons (1991) found that occupational therapy students’ explicit biases did not significantly differ from business students’ disability attitudes. Taken together, the findings from these studies offer conflicting evidence on how professional education affects explicit bias of students, and the findings offer even less evidence regarding implicit bias.
Exploring occupational therapy education programs’ influence on attitudes provides invaluable information to the profession during a paradigm shift from traditional deficit-based models to biopsychosocial models and strengths-based methods of interventions for clients and changes in educational standards (Accreditation Council for Occupational Therapy Education [ACOTE®], 2018). A gap exists in the literature, with little research exploring occupational therapy students’ implicit disability bias. For this reason, the aim of this study was to explore the impact of occupational therapy graduate education on occupational therapy students’ disability attitudes, specifically how occupational therapy students’ disability attitudes change throughout their graduate education.
We had two research questions:
How do occupational therapy students’ explicit disability attitudes change throughout their graduate occupational therapy education?
How do occupational therapy students’ implicit disability attitudes change throughout their graduate occupational therapy education?
To explore these research questions, we conducted a longitudinal analysis of occupational therapy students’ (N = 67) disability attitudes just before beginning and throughout their occupational therapy graduate education. Answering these questions will help the profession better understand whether, and how, occupational therapy curricula affect students’ implicit bias as they move through their professional education.
Method
Participants
After study approval by the institutional review board (IRB), participants were recruited from three entry-level graduate occupational therapy programs in the Midwest. All three programs were accredited by the Accreditation Council for Occupational Therapy Education (2018) and attended to core professional educational standards, including Level I and Level II fieldwork and credit requirements for the degree being attained. Program A was an occupational therapy doctorate (OTD) program (160 credits), Program B was a master of science (72 credits) and OTD (68 credits) program, and Program C was an OTD program (110 credits).
Data collection occurred over 4 yr: from August 2017 to June 2020. Students volunteered to participate; it was a convenience sample. Sixty-seven students participated in this study (Program A, 28 students; Program B, 23 students; Program C, 16 students). Slight attrition occurred over the years of the study; 67 students participated in the initial data collection (before they began their graduate program), 59 (88.06%) participated after the 1st yr of their graduate program, 48 (71.64%) participated after the 2nd yr of their graduate program, and 53 (79.10%) participated at their graduation. The mean age of participants when they entered their graduate program was 24.79 yr, and it was 27.34 yr after graduation (Table 1). The majority of participants were White, straight, nondisabled, and female. Most participants had at least one significant relationship (e.g., family, partner, friend) with a PWD. Family socioeconomic status was relatively evenly distributed. The mean political orientation (self-report; measured on a scale from 1 = very liberal to 100 = very conservative) of students when they entered their graduate program was 31.57, and it was 24.64 after graduation.
Demographic Characteristics of the Sample
Participants could choose more than one race.
Measures
We used the Symbolic Ableism Scale (Friedman & Awsumb, 2019) to measure participants’ explicit disability attitudes. The Symbolic Ableism Scale presents statements about disability on a Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). For example, one item is “discrimination against disabled people is no longer a problem in the United States.” The Symbolic Ableism Scale, which has been administered to a variety of populations—including undergraduate and graduate students, professionals from health services and other fields, and siblings of PWDs—is a valid and reliable tool (Friedman & Awsumb, 2019).
We used the Disability Attitude Implicit Association Test (DA–IAT) to measure participants’ implicit disability attitudes (Greenwald et al., 1998). The DA–IAT presents participants with “disabled persons” and “abled persons” categories and requires them to sort word and symbol stimuli in ways that are congruent and incongruent with stereotypes (e.g., disability and good, disability and bad). The DA–IAT examines differences in participants’ reaction times when items are congruent and incongruent with stereotypes: the quicker the reaction time, the stronger the association. Participants’ response latencies are measured throughout the rounds. Implicit Association Tests (IATs), including the DA–IAT, have been administered to millions of people from the general public; they have also been used to test the attitudes of health care professionals and undergraduate and graduate students from health care and other fields. Much literature has noted that the IAT is internally consistent and valid; it also has high test–retest reliability (Greenwald & Nosek, 2001). In addition, studies have shown the DA–IAT in particular has construct validity, discriminant validity, and reliability (Aaberg, 2012; Thomas et al., 2013; White et al., 2006).
Procedure
Before beginning their occupational therapy programs, incoming students from all three programs were forwarded recruitment emails from the research team. (No data were shared with department administrators.) The recruitment emails, which were approved by the IRB, described the longitudinal study and directed those who wanted to participate to access the study website (hosted by Inquisit Web, Version 5; Millisecond Software, Seattle, WA). After they accessed the website, students completed the informed consent and eligibility criteria. Participants were then presented with instructions and completed the DA–IAT, Symbolic Ableism Scale, and demographic questions, including their email address so that we could contact them about future years of the study and provide them with compensation ($25 gift card per year). In Year 2 through Year 4 of the study, when their spring semesters had finished, participants were emailed a new hyperlink and asked to again complete the DA–IAT, Symbolic Ableism Scale, and demographic questions.
Analysis
Raw data from the Inquisit Web 5 platform were imported into IBM SPSS Statistics (Version 27; IBM Corp., Armonk, NY). To determine participants’ scores on the Symbolic Ableism Scale, we first reverse keyed applicable items, and then we recoded participants’ answers to each item on a scale ranging from 0 to 1. Next, participants’ answers were aggregated to represent their explicit disability attitude. Scores <0.24 indicate no explicit preference, scores of 0.24 to 0.31 indicate slight explicit preference for people without disabilities, scores of 0.32 to 0.40 indicate moderate explicit preference for people without disabilities, and scores ≥0.41 indicate strong explicit preference for people without disabilities (Friedman & Awsumb, 2019).
To calculate participants’ scores on the DA–IAT, we used Greenwald et al.’s (2003) updated IAT scoring protocol; we then used Inquisit Web 5 to apply the protocol to convert participants’ response latencies into an aggregate D score for each participant. Scores of −0.14 to 0.14 indicate no preference for people without disabilities (no implicit bias), scores of 0.15 to 0.34 indicate a slight implicit preference for people without disabilities, scores of 0.35 to 0.64 indicate a moderate implicit preference for people without disabilities, and scores ≥0.65 indicate a strong implicit preference for people without disabilities (Greenwald et al., 2003). Negative values of the same ranges reveal preferences for PWDs.
We analyzed descriptive statistics and then explored our research questions. Our first research question was, “How do occupational therapy students’ explicit disability attitudes change throughout their graduate occupational therapy education?” To explore this research question, we used a repeated-measures analysis of variance (ANOVA) to examine difference in explicit attitudes at four time points: (1) before they began their graduate program, (2) after they completed the 1st yr of their graduate program, (3) after they completed the 2nd yr of their graduate program, and (4) after graduation from their occupational therapy program. Mauchly’s (1940) test of sphericity, which tests the assumption that variances of differences are equal, indicated that the assumption of sphericity was met. A post hoc analysis with Bonferroni correction (p = .02) was then conducted.
Our second research question was “How do occupational therapy students’ implicit disability attitudes change throughout their graduate occupational therapy education?” To explore this research question, we used a repeated-measures ANOVA to examine differences in implicit attitudes at the four time points mentioned earlier. Mauchly’s test of sphericity indicated that the assumption of sphericity was met.
Results
Across the years of the study, participants’ explicit disability attitudes ranged from 0.05 (no explicit bias) to 0.58 (strong explicit preference for people without disabilities). Participants’ implicit disability attitudes across the years ranged from −0.91 (strong implicit preference for PWDs) to 1.39 (strong implicit preference for people without disabilities). Table 2 outlines the students’ explicit and implicit attitudes at the four time points of their education.
Descriptive Statistics for Students’ Disability Attitudes
One participant did not complete the explicit and implicit measures.
Explicit Attitudes
A repeated-measures ANOVA was conducted to determine whether a difference occurred in students’ explicit disability attitudes throughout their education. Mauchly’s test of sphericity indicated that the assumption of sphericity was met, χ2(5) = 3.24, p = .66. The analysis revealed statistically significant differences in the students’ explicit attitudes at the four time points, F(3, 108) = 7.27, p < .001, ηp 2 = .17 (large effect). Post hoc analyses (Bonferroni correction, p = .02) revealed a reduction in explicit disability attitudes from when students began their occupational therapy program (M = 0.35, SD = 0.08, moderate explicit bias) to when students graduated from their program (M = 0.29, SD = 0.09, slight explicit bias; p < .001; Table 3 and Figure 1).
Repeated-Measures ANOVA: Post Hoc
Note. ANOVA = analysis of variance.
p < .001.
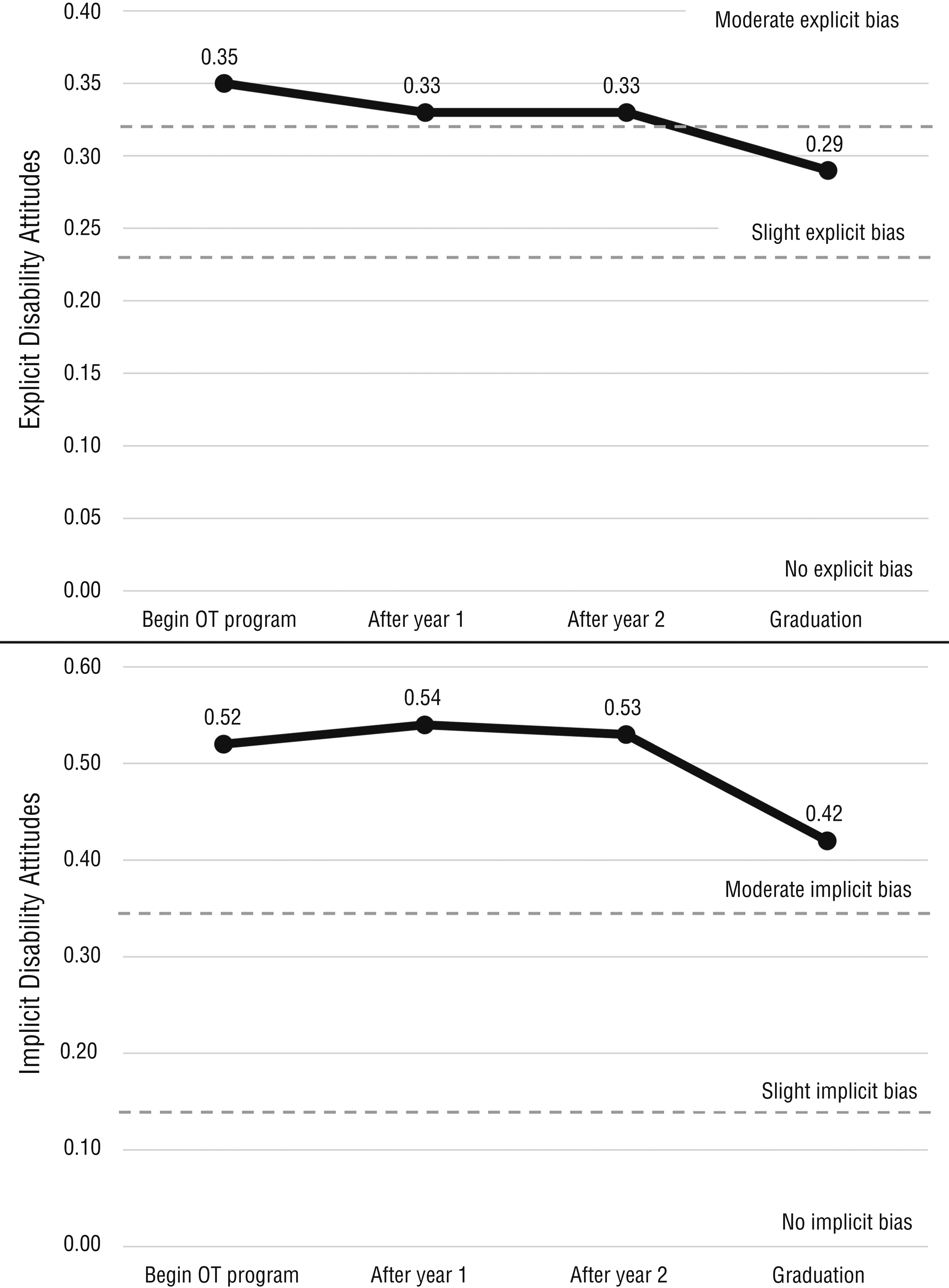
Occupational therapy (OT) students’ explicit and implicit disability attitudes during their occupational therapy education.
Implicit Attitudes
A repeated-measures ANOVA was conducted to determine whether a difference occurred in students’ implicit disability attitudes throughout their education. Mauchly’s test of sphericity indicated that the assumption of sphericity was met, χ2(5) = 1.05, p = .96. The analysis did not find statistically significant differences in the students’ implicit attitudes at the four time points, F(3, 108) = 0.90, p = .45, ηp 2 = .02 (small effect; see Table 3 and Figure 1).
Discussion
AOTA (2020a) recently acknowledged that discrimination, stigma, and implicit biases can negatively affect the provision of occupational therapy services. To reduce biases among occupational therapy practitioners, it is necessary to assess how organizational policies and procedures might reinforce or reduce prejudices, including appraisal of occupational therapy educational programs’ impact on their students’ attitudes. In response to concerns regarding bias, occupational therapy education programs are being called on by professional organizations to incorporate cultural competence and humility into educational curricula as a means to reduce bias and a means to develop empathetic, client-centered practitioners (Agner, 2020; Tyminski et al., 2019). For this reason, and to better understand the attitudes of occupational therapy students, the aim of this study was to explore students’ explicit and implicit attitudes throughout their graduate education.
Our findings revealed that occupational therapy students’ explicit disability attitudes significantly decreased between entering their occupational therapy program and their graduation, becoming more positive overall. Because responses to explicit measures may be motivated by concerns with the consequences of being seen as prejudiced, the students’ reduction in explicit attitudes may be a result of students becoming more aware of socially and politically appropriate concepts during their educational program or becoming culturally competent on issues pertaining to disability (Suarez-Balcazar et al., 2009).
Despite students’ explicit prejudice decreasing, their implicit disability attitudes did not significantly change throughout their education. In fact, 68% of students were implicitly biased at graduation, 40% of whom had strong implicit prejudices. The students’ mean implicit score at graduation was 0.42. (For contrast, Nosek et al.’s, 2007, study of 39,000 people from the general public found a mean DA–IAT score of 0.45; moreover, VanPuymbrouck et al.’s, 2020, study of 25,000 health care providers found a mean DA–IAT score of 0.54.) Our findings suggest that occupational therapy programs may fail to intervene with students’ ableist attitudes and may actually reinforce ableist attitudes. As a result of the prevalence of ableism in society (Friedman, 2019), occupational therapy students likely enter the profession with preconceived attitudes that disability is negative, which is similar to the attitudes of larger society (Daruwalla & Darcy, 2005). These concepts may be strengthened as a result of medical or impairment-based models of intervention being entrenched in practice frameworks, educational standards, and reimbursement mechanisms (Gupta & Taff, 2015). Biased ideas about disability problematically affect clinical decision making and lead to reduced health care access for PWDs (Harrington et al., 2009).
Although many of the students in our study had low levels of explicit prejudice, they were likely still participating in prejudice as a result of their implicit attitudes. Although implicit prejudice often is more subtle, it can be just as harmful as overt forms, resulting in maintenance of unjust social, political, and economic structures as well as restriction of opportunities for PWDs (Dovidio & Gaertner, 2008). Implicit attitudes may also result in biased people trivializing the experiences of PWDs and the discrimination that they face (Keller & Galgay, 2010). The mismatch between occupational therapy students’ explicit and implicit disability attitudes may be particularly challenging, because they are likely to believe they feel positively about PWDs and that they are not prejudiced; yet, they still participate in prejudiced thought and behavior without realizing it.
Limitations
Several limitations should be considered when interpreting our findings. Participants came from three different occupational therapy graduate programs in the Midwest that do not necessarily reflect occupational therapy education as a whole. Although they were compensated for their time, occupational therapy students volunteered to participate in this study; thus, self-selection bias is a possibility. In addition, the slight attrition that occurred over the years may have affected the findings.
Implications for Occupational Therapy Education
Occupational therapy education programs have an important role to play in terms of intervening to minimize prejudicial attitudes and assumptions about disability and, in the process, address students’ ableist thinking. Although occupational therapy education continues to attend to client factors such as body structures and body functions (focus on impairment) as targets for intervention design (AOTA, 2020b), recognition of the interactional role of environments in disability is growing. Additionally, there is growing discourse that the unique value that occupational therapy practitioners contribute to interdisciplinary rehabilitation teams is a holistic approach to achieving meaningful engagement in client-identified occupations (Cohn, 2019). In fact, there have been criticisms, including from within the profession, that occupational therapy students often enter practice with little understanding of how to develop interventions targeting the social barriers that prohibit PWDs from participating in occupation (Fisher, 2018).
To reduce occupational therapy students’ (future practitioners’) ableism, and to also give them a richer and more accurate understanding of the lived experiences of PWDs, occupational therapy education programs should work to better align with social and occupational justice (Aldrich et al., 2017). In particular, disability studies concepts that reframe traditional occupational therapy understandings of disability and impairment—particularly in relation to social–political environmental barriers, interdependence, and lived experience—have been increasingly incorporated into occupational therapy literature, research, and education (Magasi, 2008; McCormack & Collins, 2010). Thus, our findings have the following implications for occupational therapy education:
To reduce bias, educators should introduce key concepts that support disability as a social construction (Oliver, 2013) early and reinforce them throughout students’ education.
Evidence exists that specific holistic occupational therapy models of practice have a mediating impact on students’ biases (e.g., individualizing disability was associated with higher implicit ableism; VanPuymbrouck & Friedman, 2020). Moreover, students who identified with the Canadian Model of Occupational Performance and Model of Human Occupation frameworks had less anti-fat bias (Friedman & VanPuymbrouck, 2019). Therefore, these models should be embraced by education programs.
The differences between explicit and implicit outcomes point to the need for future occupational therapy appraisals of bias to include, if not exclusively use, implicit assessments.
This study can be used to lay the groundwork for future research to explore other biases to inform the development of methods for mitigating prejudice in future occupational therapy clinicians.
Conclusion
Research indicates that a lack of practitioner knowledge about working with PWDs results in disparities in health care access and outcomes for PWDs (Peacock et al., 2015). When we examined the explicit and implicit disability attitudes of occupational therapy students throughout their education, we found that whereas their explicit attitudes decreased (i.e., became more favorable), their implicit attitudes did not; in fact, the majority of students were implicitly ableist at graduation. These findings have problematic implications for practice and clinical decision making; they show that more emphasis is needed on developing educational standards (ACOTE, 2018) to produce clinicians who are empathetic and nonbiased, because the majority of occupational therapy clients are PWDs.
Supplemental Material
Supplementary material for Impact of Occupational Therapy Education on Students’ Disability Attitudes: A Longitudinal Study
Supplementary material, sj-docx-1-aot-10.5014_ajot.2021.047423.docx for Impact of Occupational Therapy Education on Students’ Disability Attitudes: A Longitudinal Study by Carli Friedman and Laura VanPuymbrouck in The American Journal of Occupational Therapy
Footnotes
Acknowledgment
This study was funded by Spencer Foundation Grant 201700112.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.