
Abstract
This review highlights the lack of and need for interventions within the scope of occupational therapy to increase participation for adults with MS
In 2018, the National Institutes of Health (NIH) estimated that 400,000 Americans and more than 2.5 million people worldwide live with multiple sclerosis (MS). MS, an incurable neurodegenerative autoimmune disease, affects the central nervous system (Huang et al., 2017; NIH, 2018). The level of severity of MS is unique to each person and varies on the basis of the location of neurological involvement (Zurawski & Stankiewicz, 2018). Plaques located within the gray and white matter of the brain, in combination with neuronal demyelination, can result in a wide range of debilitating symptoms (Huang et al., 2017). MS can contribute to physical and physiological symptoms that affect occupational performance and social participation (Karhula et al., 2019; NIH, 2018; Yu & Mathiowetz, 2014a).
The primary symptoms of MS include fatigue, difficulty walking, spasticity, weakness, cognitive loss, vision changes, and bowel and bladder dysfunction, and less common symptoms include speech and swallowing problems, tremor, and hearing deficits (National Multiple Sclerosis Society, 2020). The complexity and variability of the disease process affect people’s ability to participate in all areas of their daily lives (Karhula et al., 2019; Yu & Mathiowetz, 2014a).
Changes in occupational performance can affect various life roles, such as work and social participation (Yu & Mathiowetz, 2014a). The American Occupational Therapy Association (AOTA, 2020) has described work as labor that contributes to society and social participation as engaging in activity that promotes social interaction. Occupational therapy interventions facilitate and enhance a person’s ability to engage and participate in meaningful occupations (Yu & Mathiowetz, 2014a). The purpose of this systematic review was to provide occupational therapy practitioners with evidence supporting the use of interventions to enhance the performance of and participation in education, work, volunteering, leisure, and social participation among adults (age ≥18 yr) with MS. The research question addressed by the systematic review was “What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve and/or maintain the performance of and participation in education, work, volunteering, leisure, and social participation among adults with MS?”
Method
This systematic review was supported by the AOTA Evidence-Based Practice (EBP) Program. It was conducted according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P; Liberati et al., 2009). The study protocol was not registered. We, along with a medical librarian, research methodologist, and AOTA staff, developed the review protocol and finalized the search terms and research question. To enhance the transparency of the review, an external advisory group of content experts with knowledge of neurodegenerative diseases and systematic reviews reviewed the research question and search terms before the review was undertaken.
Data Sources
The MEDLINE, PsycINFO, CINAHL, OTseeker, and Cochrane Database of Systematic Reviews databases were searched for articles published from January 2011 to December 2018. This review picked up from where the articles included in a previous review left off (Yu & Mathiowetz, 2014a, 2014b). The medical librarian sent the search results to the AOTA research methodologist, who then excluded studies that were duplicates or clearly did not meet the review criteria (i.e., wrong year, not MS, not research). The remaining citations were then sent to the review team. The reviewers analyzed the articles (abstract, full text) with support from the AOTA research methodologist and the director of the EBP project. See Appendix A for a sample search strategy for the study.
Inclusion and Exclusion Criteria
Inclusion criteria for this review were as follows: peer-reviewed scientific literature (Levels 1a and 1b, 2a and 2b, and 3a and 3b) published in English between January 2011 and December 2018 that addressed intervention approaches within the scope of practice of occupational therapy for adults (age ≥18 yr) with MS. We included only studies that provided evidence at Levels 1b, 2b, and 3b based on the Oxford levels of evidence, developed by the Oxford Centre for Evidence-Based Medicine (2009). Level 1b includes individual well-designed randomized controlled trials (RCTs; not pilot or feasibility studies); Level 2b includes individual prospective cohort studies, low-quality RCTs, ecological studies, and two-group nonrandomized studies; and Level 3b includes individual retrospective case-control studies, one-group nonrandomized pretest–posttest studies, and cohort studies. Exclusion criteria included Level 4 and Level 5 studies, presentations, conference proceedings, non–peer-reviewed research literature, dissertations, theses, interventions outside the scope of occupational therapy practice, research published outside the inclusion dates, and research including anyone younger than age 18 yr.
Data Extraction and Risk of Bias
Both authors independently evaluated all articles at each stage of the review and then compared their results. This process included identifying the citation, rationale for inclusion or exclusion, and level of evidence. Any disagreement was discussed until a resolution was reached. An evidence table was created for all articles included in the review (Table B.1 in Appendix B). The AOTA research methodologist and EBP director reviewed the evidence table for quality control. The methods used to assess risk of bias depended on the study design. Randomized and nonrandomized controlled trials were assessed using the Cochrane Risk of Bias Control Trials (Higgins et al., 2016), and pre–post studies with no control group were assessed using the National Heart, Lung, and Blood Institute (2014) criteria (Tables B.2 and B.3). The risk of bias for the studies included in the review ranged from low to moderate.
Analysis and Synthesis
All articles were analyzed for appropriateness related to the inclusion and exclusion criteria, level of evidence, risk of bias, and statistical significance of findings, resulting ultimately in an assigned strength of evidence as a guide for clinical practice. The U.S. Preventive Services Task Force (2018) definitions for strength of evidence (level of certainty) were used to classify the themed evidence as strong, moderate, or low. Strong evidence refers to 2 or more well-designed Level 1b studies. Moderate evidence refers to at least 1 Level 1a or 1 Level 1b high-quality study or multiple-level 2a or 2b or multiple-level 3a or 3b moderate-quality studies. Low evidence refers to a small number of low-level studies with flaws. Strength of evidence was determined for the studies included in systematic review using these definitions. Because of the limited number of articles included in the final review, only the narrative synthesis was conducted.
Results
The database search yielded 12,894 articles, of which 618 were fully screened after inappropriate articles were removed (duplicates, clearly outside the scope of occupational therapy, wrong year, not research, wrong population). Eight additional duplicate articles were removed during the screening process, yielding 610 full-text articles that were assessed for eligibility (Figure 1). Articles were removed after review if they did not meet the inclusion criteria. Ultimately, 4 articles were identified for inclusion in this systematic review. The articles included all the data needed for the review, and authors were not contacted with any follow-up questions.
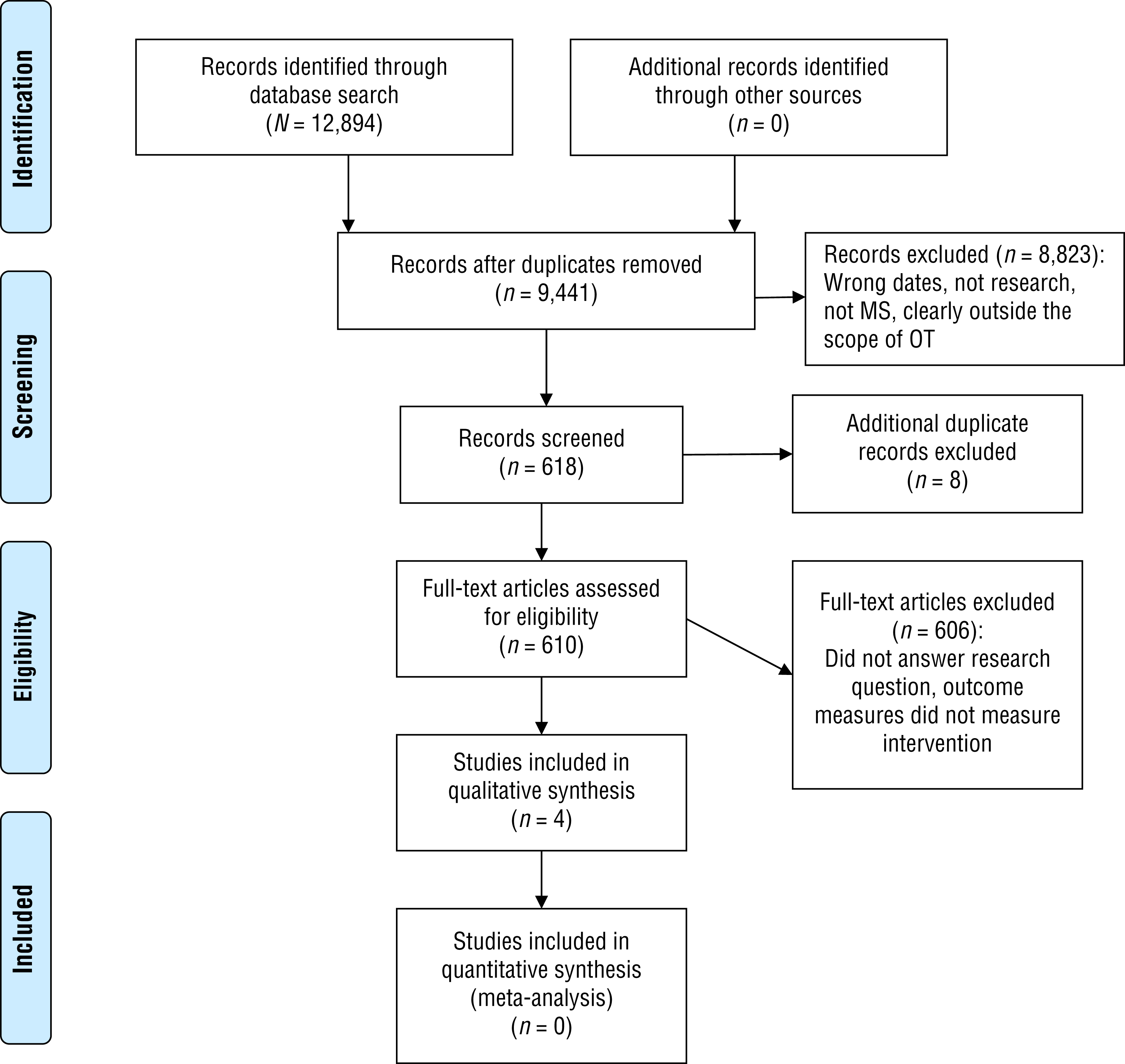
Flow of articles through the systematic review process.
Three articles in the study addressed work, 1 Level 1b (Dorstyn et al., 2018) and 2 Level 3b (Dorstyn et al., 2017; Lexell et al., 2014). These 3 studies were further grouped into two subthemes on the basis of the type of work intervention: community-based online intervention (Dorstyn et al., 2017, 2018) and hospital-based interdisciplinary rehabilitation (Lexell et al., 2014). One Level 1b article addressed social participation (Hasanpour-Dehkordi et al., 2016). None of the other outcomes of interest—education, volunteering, and leisure—were addressed by the studies that met the inclusion criteria.
Work
Community-Based Online Intervention
Moderate strength of evidence and moderate risk of bias were found for interventions addressing work. Online training modules for work provided better understanding of vocational and career goals; general improved self-esteem, work relations, and financial concerns; and gains in vocational self-efficacy, identity, and life optimism (Dorstyn et al., 2017, 2018). A total of 156 participants with a mean age of 43.88 yr participated across the three work studies.
Dorstyn et al. (2017) conducted a focus group and a single-group, pre–post pilot study of the seven Work and MS program online training modules, which consisted of an introduction, job facts, finding work, résumé writing and interview preparation, job interview dos and don’ts, maintaining work, and career development. Each module contains an interactive PowerPoint component, downloadable education materials, and a content summary. Participants received a presurvey, the Work and MS modules to complete at their own pace, and a follow-up survey approximately 6 wk later. Outcome measures included the Multiple Sclerosis Rating Scale–Revised (MSRS–R), Service Obstacles Scale (SOS), 25-item Job-Procurement Self-Efficacy Scale (JSES), My Vocational Situation Scale–My Vocational Identity (MVI), Life Orientation Test–Revised (LOT–R), Patient Health Questionnaire–9 (PHQ–9), and open-ended questions so participants could comment on the modules and structure of the intervention. Significant results included gains in vocational self-efficacy (p = .04), identity (p = .01), and life optimism (p = .04). Fewer participants met the criteria for major depression on the posttest, although this finding was nonsignificant.
Dorstyn et al. (2018) recruited 95 community-based adult participants with MS who wanted to return to work or who were currently working and desired alternative work to take part in an RCT. Participants needed to speak English and have access to a computer with internet service. An online survey was sent at enrollment, and participants in the intervention group (n = 45) then received the first three Work and MS program modules (Dorstyn et al., 2017, 2018) by email to review at their own pace. A follow-up email with the remaining four modules was sent 1 wk later, and an online survey was sent 4 wk postenrollment. Each module took approximately 20 min to complete. The control group (n = 50) received an online survey at enrollment and an online survey at 4 wk postenrollment. After completing the second survey, the control group was emailed the Work and MS modules. The primary outcome measures for this study were the MVI and the JSES. Secondary outcome measures were the Multiple Sclerosis Work Difficulties Questionnaire, LOT–R, and PHQ–9. Baseline measures included sociodemographic information, the MSRS–R, and the SOS. The researchers found statistically significant improved results immediately after participants accessed the Work and MS modules; participants reported better understanding of vocational and career goals (p = .008) and improved general self-esteem (p = .02), work relations (p = .03), and financial concerns (p = .04).
Hospital-Based Interdisciplinary Rehabilitation
There is low strength of evidence for hospital-based interdisciplinary rehabilitation because of the lack of studies. Lexell et al. (2014) conducted a Level 3b retrospective study with a pre–post design with 43 participants who received individualized goal-oriented interdisciplinary rehabilitation in a university hospital. The Canadian Occupational Performance Measure (COPM) was administered to all participants at admission and discharge. Outcome measures included the COPM, the Expanded Disability Status Scale, and the visual analog scale. No significant differences were found between three areas of the COPM on admission; the highest scores were on work and socialization, and the lowest scores were on quiet recreation and community management. A significant correlation was found between changes in performance and changes in satisfaction from admission to discharge (p < .001).
Social Participation
Interventions for social participation provided moderate strength of evidence and low risk of bias for improving or maintaining social participation and performance of and participation in work for adults with MS. Hasanpour-Dehkordi et al. (2016; Level 1b) recruited 60 participants for an RCT of yoga exercises. The intervention group (n = 30) performed 60–70 min of yoga exercises 3×/wk for 12 wk. The control group (n = 30) received no intervention. Outcome measures included demographics, Spielberger Anxiety Inventory, physiological indices, Bayer Pain Scale, Rotten Fatigue Severity Scale, and the 36-item Short Form Survey (SF–36) Quality of Life questionnaire. The researchers found that the intervention group had significantly higher mean scores on quality of life and social functioning (p < .05).
Discussion
No studies assessing education, volunteering, or leisure participation met the criteria for this review. The final review included only 4 studies, which addressed work and social participation outcomes. All 4 studies were conducted outside of the United States. The Dorstyn et al. (2017, 2018) studies were conducted in Australia, and the Hasanpour-Dehkordi et al. (2016) and Lexell et al. (2014) studies were conducted in Iran. MS affects nearly one million people in the United States (National Multiple Sclerosis Society, 2020), but no study from the United States met the inclusion criteria for this review. The void in research on the effectiveness of interventions within the scope of occupational therapy practice to improve or maintain the performance of and participation in these occupations is disadvantageous to the profession and to people with MS. Occupational therapy practitioners would benefit from more research so that they can provide evidence-based interventions for their clients. The World Health Organization and Multiple Sclerosis International Federation (2008) reported the global median estimated prevalence of MS to be 30 per 100,000. The number of people living with MS warrants research on the effectiveness of interventions provided by occupational therapy practitioners.
On the basis of this review, there is evidence that online modules are an intervention approach that has potential to improve work-related skills (Dorstyn et al., 2017, 2018). Online education on aspects of work prepared participants to understand vocational and career goals and improved self-esteem among community members with MS (Dorstyn et al., 2018). In addition, online education resulted in gains in self-efficacy, identity, and life optimism (Dorstyn et al., 2017). Using online resources to supplement individualized goal-oriented interdisciplinary therapy should be considered if clients have a desire to return to work or are seeking alternative work opportunities.
In addition, moderate strength of evidence indicated that group yoga classes help to improve quality of life and social functioning among community members with MS (Hasanpour-Dehkordi et al., 2016). Incorporating yoga into therapy or as a leisure activity for adults with MS who are interested in yoga should also be considered. Because research is limited, occupational therapy practitioners will need to continue to use their clinical judgment and expertise to determine the appropriate interventions when working with adults with MS. The outcome of the review indicates that more evidence is required.
Implications for Occupational Therapy Practice, Research, and Education
This review has the following implications for occupational therapy practice, research, and education:
Evidence supports the positive outcomes of online modules to prepare adults with MS for work. Providing training materials and individualized goal-oriented therapy improved self-esteem, self-efficacy, identity, life optimism, and satisfaction.
Evidence supports the use of group yoga sessions to improve quality of life and social functioning among adults with MS.
Well-designed studies of work and social participation for adults with MS are needed.
Future research needs to focus on occupation-based interventions to improve participation outcomes for adults with MS.
Limitations
This review was limited by the small number of studies and low level of evidence of the studies. Only English-language studies were included, which may have resulted in missing pertinent articles. Although a standardized approach was taken for the review, it is possible that articles were missed. Articles that did not include successful interventions may not have been published, thus raising the possibility of publication bias. As always with occupational therapy research, the complexity of the interventions and differences between participant groups can make it difficult to compare studies.
Conclusion
Evidence supported interventions to improve work and social participation for adults with MS; however, we found no evidence for education, volunteering, or leisure. These facets of occupation are important for people with MS, and research is needed to guide clinical practice. There is a critical need for research in these areas to support the interventions for use with adults with MS.
Supplemental Material
Supplementary material for Evidence for Occupational Therapy Interventions Supporting Work and Social Participation for Adults With Multiple Sclerosis: A Systematic Review
Supplementary material, sj-docx-1-aot-10.5014_ajot.2021.048058.docx for Evidence for Occupational Therapy Interventions Supporting Work and Social Participation for Adults With Multiple Sclerosis: A Systematic Review by Julie Ann Nastasi and Linda Harris in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Elizabeth G. Hunter and Deborah Lieberman at the American Occupational Therapy Association (AOTA) for their support throughout the systematic review. The systematic review was sponsored by AOTA. The authors have no conflict of interest to report.
Appendix A. Search Strategy for Questions 1,2,and 3
Evidence and Risk-of-Bias Tables for the Systematic Review
Risk-of-Bias Table for Noncontrolled Studies
| Citation | Study Question or Objective Clear | Eligibility or Selection Criteria Clearly Described | Participants Representative of Real- World Patients | All Eligible Participants Enrolled | Sample Size Appropriate for Confidence in Findings | Intervention Clearly Described and Delivered Consistently | Outcome Measures Prespecified, Defined, Valid and Reliable, and Assessed Consistently | Assessors Blinded to Participant Exposure to Intervention | Loss to Follow-Up After Baseline ≤20% | Statistical Methods Examine Changes in Outcome Measures From Before to After Intervention | Outcome Measures Were Collected Multiple Times Before and After Intervention | Overall Risk of Bias Assessment |
| Dorstyn et al. (2017) | Y | N | NR | Y | Y | Y | Y | NR | N | Y | Y | M |
| Lexell et al. (2014) | Y | Y | Y | Y | N | N | Y | NR | Y | Y | Y | M |
Note. Y = yes; N = no; NR = not reported. Adding Yes scores for each item and dividing by 11 yields a risk-of-bias rating: low risk (L) = 75%–100%, moderate risk (M) = 25%–75%, and high risk (H) = 0%–25%. Risk-of-bias tool adapted from Quality Assessment Tool for Before–After (Pre–Post) Studies With No Control Group, by National Heart, Lung, and Blood Institute, n.d. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
This table is a product of AOTA’s Evidence-Based Practice Program and AOTA and is copyright © 2021 by the American Occupational Therapy Association. It may be freely reproduced for personal use in clinical or educational settings as long as the source is cited. All other uses require written permission from the American Occupational Therapy Association. To apply, visit http://www.copyright.com.
Citation: Nastasi, J. A., & Harris, L. (2021). Evidence for occupational therapy interventions supporting work and social participation for adults with multiple sclerosis: A systematic review (Table B.3). American Journal of Occupational Therapy, 75, 7504185120. https://doi.org/10.5014/ajot.2021.048058
*
Indicates articles included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.