
Abstract
A review of the current literature identifies evidence-based interventions within the scope of occupational therapy practice to improve ADLs and sleep for people with PD
Evidence-based practice in occupational therapy relies on research that demonstrates the effectiveness of various interventions. To support best practice for occupational therapy practitioners who work with people with Parkinson’s disease (PD), we conducted a systematic review (SR) to identify interventions that have been used to improve or maintain the performance of activities of daily living (ADLs), rest, and sleep for this population.
Approximately 930,000 Americans have PD, and this number is expected to rise to 1.2 million by 2030 (Marras et al., 2018). People diagnosed with PD experience varying degrees of disturbance in activity of daily living (ADL) and rest and sleep function (Hariz & Forsgren, 2011; Oerlemans & de Weerd, 2002). In the clinical practice of occupational therapy, addressing ADL performance is important because impairment in ADLs has been associated with higher rates of hospitalization (Hoyer et al., 2013), longer hospital stays (Carpenter et al., 2007), higher rates of admission to long-term care (Gaugler et al., 2007), and higher mortality rates (Millán-Calenti et al., 2010). Impaired sleep quality is a frequent early symptom seen in people with PD and has been negatively correlated with their perceived quality of life (Duncan et al., 2014; Gomez-Esteban et al., 2011; Pandey et al., 2016). In addition, effective performance in these areas has been considered an essential component of occupational balance since the founding of occupational therapy (Meyer, 1922).
A prior SR of the literature on the efficacy of occupational therapy interventions for people with PD was conducted and published by Foster et al. in 2014. That review included articles published between January 2003 and May 2011 and focused on any interventions that were within the scope of occupational therapy, regardless of outcome measure. Evidence was summarized for several outcome areas (motor performance, balance, cuing strategies, and wellness initiatives), but no studies at that time used outcome measures related to the efficacy of interventions to improve ADL performance in people with PD (Foster et al., 2014). This gap in the literature is significant both because ADL performance is a core goal of occupational therapy intervention and because impairment in ADL performance is common in people with PD because of the motor and nonmotor symptoms of the disease (Hariz & Forsgren, 2011; Leroi et al., 2011).
Satisfactory ADL, rest, and sleep performance stems from the functioning of multiple client factors, including sensorimotor, psychosocial, and cognitive systems (Bugalho et al., 2016). All of these systems can be affected by the progressive manifestations of symptoms common to PD, including bradykinesia, incoordination and tremoring, rigidity, flat affect, impaired cognition, depression, anxiety, autonomic disturbances, and sensory impairment (Sveinbjornsdottir, 2016). People with PD experience impairment in their level of efficiency and independence in completing ADLs such as grooming, feeding, and dressing (Hariz & Forsgren, 2011). Although ADLs and rest and sleep performance are recognized issues for people with PD, the definitions of these outcomes frequently vary.
For the purposes of this SR, ADLs, rest, and sleep are used as defined in the Occupational Therapy Practice Framework: Domain and Process (4th ed.; OTPF–4; American Occupational Therapy Association [AOTA], 2020). ADLs consist of bathing and showering, toileting and toilet hygiene, dressing, eating and swallowing, feeding, functional mobility, personal hygiene and grooming, and sexual activity. Rest and sleep are “activities related to obtaining restorative rest and sleep to support healthy, active engagement in other occupations” (AOTA, 2020, p. 32). In this SR, we sought to answer the question, What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve or maintain performance and participation in ADLs and rest and sleep for adults with PD? This work updates the SR by Foster and colleagues (2014) and provides a narrower focus on ADL, rest, and sleep outcomes relevant to best occupational therapy practice.
Method
This SR was supported by AOTA’s Evidence-Based Practice (EBP) Program and is one of a series of reviews related to PD (see Boone et al., 2021, and Foster et al., 2021, in this issue). The review was conducted according to the Cochrane Collaboration methodology (Higgins & Green, 2011) and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting an SR (Moher et al., 2009). The methodology used for the review was a collaborative effort among AOTA staff, the review authors, a medical librarian, and a research methodologist.
Inclusion Criteria
To be included, articles had to be peer reviewed and published in English between January 2011 and December 2018. Only studies providing evidence at Levels 1b, 2b, and 3b based on the Oxford levels of evidence (Oxford Centre for Evidence-Based Medicine, 2009) were chosen for review (Table 1). All interventions studied had to be within the scope of occupational therapy practice as defined in the OTPF–4, which includes occupations and activities, interventions to support occupations, education and training, advocacy, group interventions, and virtual interventions (AOTA, 2020, pp. 59–62). Only studies that measured the outcomes of ADLs, rest, or sleep were included, and the population of interest was adults (age >18) with PD. Pertinent SR articles were hand searched for additional articles. Conference abstracts, poster presentations, dissertations, theses, and noninterventional studies were excluded.
Levels of Evidence
Note. RCT = randomized controlled trial. Adapted from Oxford Centre for Evidence-Based Medicine: Levels of evidence (March 2009), by Oxford Centre for Evidence-Based Medicine, 2009. https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009
Information Sources
Databases searched included MEDLINE, PsycINFO, CINAHL, OTseeker, and the Cochrane Database of Systematic Reviews. Individual bibliographies and journals were hand searched as needed. Search terms were developed by the authors and then reviewed by members of the AOTA EBP Program team.
Study Selection and Analysis
The EBP Program research methodologist provided authors Barbara M. Doucet and Ingrid Franc with 627 abstracts to review. The abstracts were uploaded to a common Dropbox location and independently evaluated by Doucet and Franc to determine whether the articles potentially met basic eligibility criteria. The two authors then met to reach a consensus on whether each abstract indicated that the full study should be examined for possible inclusion.
A comprehensive evidence table was created that described the risk of bias, level of evidence, study design, participants, setting, inclusion criteria, intervention and control conditions, outcome measures, and results for all articles selected for inclusion. Both significant and nonsignificant findings were included in the evidence table (see Table A.1 in the Appendix).
The U.S. Preventive Services Task Force (2018) strength of evidence table was used to evaluate each intervention theme. Strong strength of evidence includes two or more Level 1 well-designed, well-conducted studies with strong findings. Moderate strength of evidence consists of at least one Level 1 or multiple Level 2 and 3 studies that are sufficient to determine effect on health outcomes but with confidence constrained by the number, size, or quality of studies or inconsistent findings. Low strength of evidence indicates that the evidence is insufficient to determine effects on health because of the limited number or size of studies, inconsistent findings, or lack of pertinent health-related information.
Authors Doucet and Franc evaluated the articles selected for review individually using risk-of-bias assessments appropriate to the study design (Higgins et al., 2016). Quality elements were identified as being either present or absent; these elements included selection bias, performance bias, detection bias, reporting bias, blinding, attrition, sample size, and enrollment (Table A.2). Each article was scored as having low, moderate, or high overall risk of bias (Table A.3).
Results
Six hundred twenty-seven abstracts were provided for review. After reviewing the abstracts, we selected 124 articles for full review; 89 of these did not meet the inclusion criteria or were low-quality studies that duplicated results found in higher quality studies. Thus, 35 of these articles were included in the review, and 10 additional articles that met the inclusion criteria were extracted from 10 SRs, bringing the final article total to 45 (Figure 1).
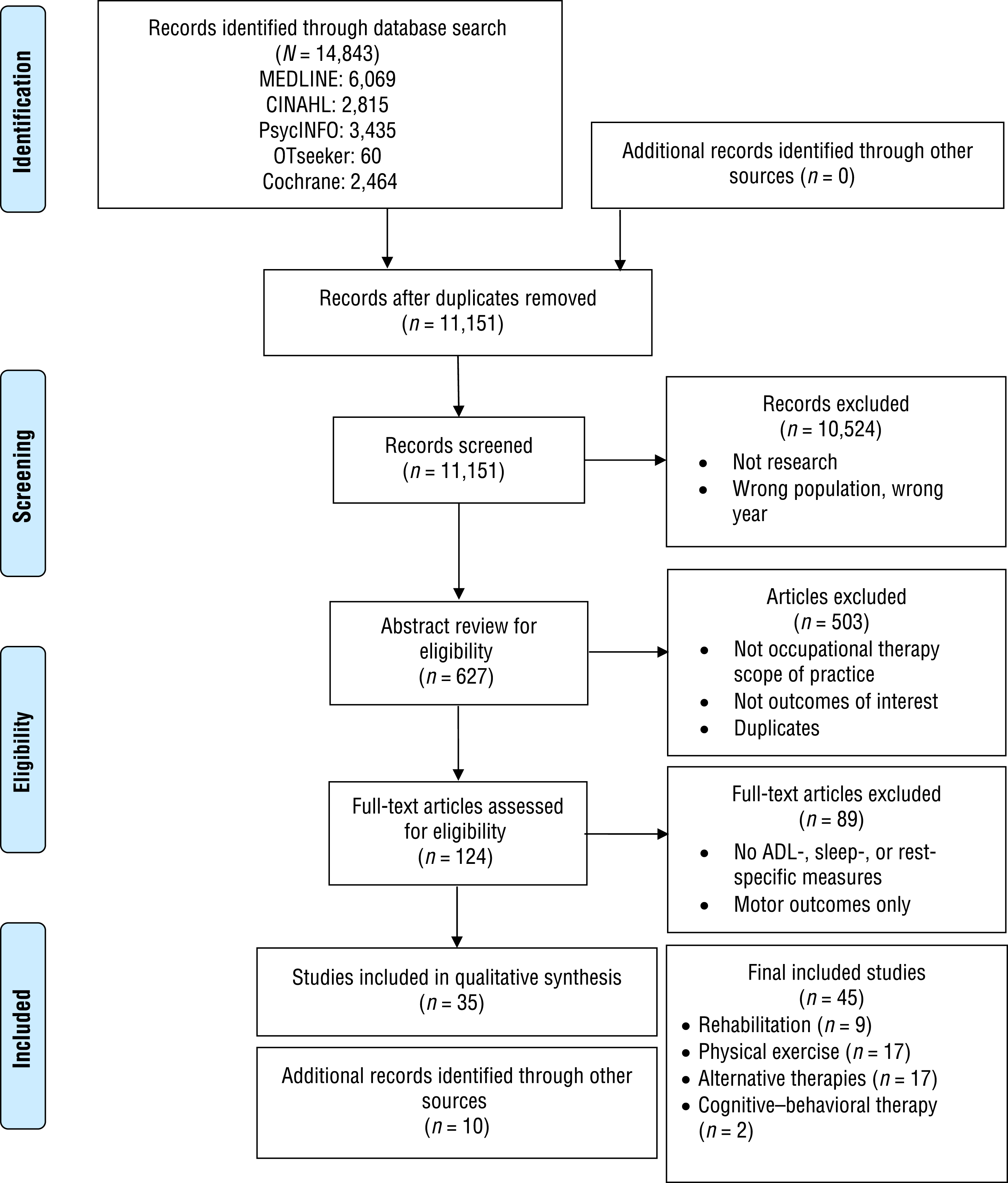
Flow diagram for studies included in the systematic review.
We analyzed the 45 studies and grouped them into four intervention themes: rehabilitation, physical exercise, alternative therapies, and cognitive–behavioral therapy (CBT). No studies used measures of rest as an outcome. Therefore, the results address only the outcomes of ADL and sleep performance. Thirty-one studies had low risk of bias, 13 had moderate risk of bias, and 1 had high risk of bias.
The interventions took place in inpatient rehabilitation facilities (n = 8), outpatient settings (n = 14), and various community settings (n = 23), including participants’ homes, municipal pools, research labs, and dance studios. Three-quarters (76%, n = 34) of the studies were conducted outside the United States. The two most frequently used assessment tools across studies were the Unified Parkinson’s Disease Rating Scale Section II (UPDRS II; Fahn & Elton, 1987), a measure of ADL performance, and the Parkinson’s Disease Questionnaire–39 (PDQ–39; Jenkinson et al., 1997). Both tools are typically administered via self-report.
Rehabilitation
Four Level 1b randomized controlled trials (RCTs) and 5 Level 2b RCTs met the inclusion criteria. The interventions evaluated in these 9 studies included multidisciplinary intensive rehabilitation treatment (MIRT; n = 7) and outpatient occupational therapy (n = 2).
Multidisciplinary Intensive Rehabilitation Treatment
Strong strength of evidence indicates that MIRT improves ADL performance, and moderate strength of evidence indicates that it improves sleep in people with PD. All 7 studies were conducted at inpatient rehabilitation facilities in Italy. The most common intervention duration was 4 wk (Ferrazzoli et al., 2018; Frazzitta et al., 2012, 2014; Frazzitta, Maestri, Bertotti, et al., 2015; Frazzitta, Maestri, Ferrazzoli, et al., 2015); Monticone et al.’s (2015) intervention lasted 8 wk, and Palamara et al.’s (2017) intervention lasted 6 wk.
Occupational therapy interventions provided as part of MIRT consisted of ADL training, hand and finger exercise, self-management, and cognitive–behavioral strategies (Ferrazzoli et al., 2018, Level 1b); ergonomic education, modification of ADLs at home, adaptive equipment recommendation, and ADL training using adaptive techniques (Monticone et al., 2015, Level 1b); and transfer training, bed mobility, dressing training, hand exercise, and home exercise programs (Frazzitta et al., 2012, Level 2b; Frazzitta, Maestri, Bertotti, et al., 2015, Level 2b; Frazzitta, Maestri, Ferrazzoli, et al., 2015, Level 1b; Frazzitta et al., 2014, Level 2b). The occupational therapy intervention in the study by Palamara et al. (2017, Level 2b) was described only as “occupational therapy to improve autonomy in everyday tasks” (p. 1078). In all studies, occupational therapy was provided for 1 hr/day, 5 days/wk.
All of the studies in this theme found significant improvement in ADL performance immediately on completion of MIRT, and several showed continued gains in follow-ups that varied from 4 to 12 mo (Ferrazzoli et al., 2018; Frazzitta et al., 2012; Frazzitta, Maestri, Bertotti, et al., 2015; Monticone et al., 2015). Participants had significantly improved sleep scores on the Parkinson’s Disease Sleep Scale after MIRT compared with the control group, who received pharmacological treatment only and showed no change (Frazzitta, Maestri, Ferrazzoli, et al., 2015).
Outpatient Occupational Therapy
Low strength of evidence is available for outpatient occupational therapy interventions to improve ADL performance in people with PD because of the small number of studies and inconsistent results. A study from outpatient clinics in the United Kingdom showed no significant ADL improvement on the PDQ–39 after four occupational therapy sessions that provided advice and equipment but very little task practice (Clarke et al., 2016, Level 1b). Clarke et al. (2016) concluded that the intervention was not effective, but Mestriner (2016) subsequently published criticism of the methodology used in Clarke et al.’s study. Sahu et al. (2018, Level 2b) compared groups receiving (1) traditional outpatient occupational therapy (e.g., ADL training, hand function, bilateral coordination, dual task training) plus walking training and (2) traditional occupational therapy only; both groups showed significant gains in FIM® ADL scores.
Physical Exercise
Four Level 1b RCTs, 8 Level 2b RCTs, 1 Level 2b non-RCT, and 4 Level 3b pretest–posttest studies met the inclusion criteria and provide evidence on the efficacy of physical exercise interventions to improve ADL performance in people with PD. The type of exercise program varied across studies, so we further subdivided this theme into the categories of resistance training, multimodal exercise programs, exercise programs targeting specific body structures, and physical exercise for sleep.
Resistance Training
Only 1 study explored the effect of resistance training on ADLs; therefore, low strength of evidence is available for the use of resistance training to improve ADLs. Participants in a resistance training program showed no significant improvement in ADL scores on the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS–UPDRS; Ferreira et al., 2018, Level 2b).
Multimodal Exercise Programs
Moderate strength of evidence indicates that group-based multimodal exercise programs can improve ADL performance, but the studies’ outcomes were inconsistent, and only 1 was a high-quality study. An outpatient group exercise program of flexibility, balance, and functional tasks resulted in significantly improved UPDRS II scores compared with an aerobics program with home exercises (Schenkman et al., 2012, Level 1b). Significant improvements in UPDRS II scores were found after multimodal exercise sessions (stretching, strengthening, mobility exercises, balance training, Wii games; Pompeu et al., 2012, Level 2b). Pedreira et al. (2013, Level 2b) saw significant improvement in PDQ–39 ADL scores after a physical therapy group intervention combined with Wii games compared with physical therapy only.
A multimodal exercise program of balance, gait, and dual-task training resulted in significant improvement in UPDRS II scores compared with a nontreatment control condition (Wallén et al., 2018, Level 1b). Lee et al. (2019, Level 2b) found no gains in ADL performance in participants who completed a group intervention using line dancing and resistance band exercise compared with a usual care control group. Volpe et al. (2014, Level 2b) found significantly improved PDQ–39 and UPSRS II scores for participants in an exercise program of stretching, balance exercises, and perturbation activities in water compared with participants in the same program on land. Carvalho et al. (2015, Level 2b) found no significant improvement on the UPDRS II in participants in three groups—aerobic exercise, strengthening exercise, and traditional physical therapy. An individual agility boot camp with one-on-one guidance by a physical therapist resulted in significantly improved UPDRS II scores, but no significant improvement was seen when the boot camp was delivered in a group or home exercise format (King et al., 2015, Level 1b).
Exercise Programs Targeting Specific Body Structures
Moderate strength of evidence indicates that exercise programs that target specific body structures can improve ADLs. A high-quality RCT evaluating the HOMEDEXT hand exercise program found significant improvement in participants’ dexterity-related ADLs compared with the control condition of resistance band training (Vanbellingen et al., 2017, Level 1b). An outpatient postural exercise program, the Mézières method, resulted in significantly improved UPDRS II scores compared with a home exercise group (Paolucci et al., 2017, Level 2b). Participants in a weekly lower extremity exercise program using a cycle ergometer showed significant improvement in UPDRS II scores (Lauhoff et al., 2013, Level 3b). Two oral–motor exercise programs resulted in improved chewing and swallowing (Argolo et al., 2013, Level 3b) and significantly improved time and volume per swallow (Athukorala et al., 2014, Level 3b). A pelvic floor exercise program reduced participants’ urinary frequency and urgency (Vaughan et al., 2011, Level 3b).
Physical Exercise for Sleep
Two Level 2b studies, 1 an RCT and 1 a non-RCT, explored the use of various exercises to reduce sleep disturbances in people with PD. Both found significant improvement and provide moderate strength of evidence for this type of intervention. The RCT examined a resistance training exercise intervention that resulted in significantly reduced sleep disturbance and improved sleep quality scores (Silva-Batista et al., 2017). In the non-RCT, an individual exercise program using balance and coordination tasks, rhythmic exercises, resistance training, and aerobic circuits also significantly reduced sleep disturbances (Nascimento et al., 2014).
Alternative Therapies
Two Level 1b, 11 Level 2b, and 4 Level 3b studies met the inclusion criteria for review. These studies provide evidence related to a variety of alternative therapy interventions addressing ADL performance and sleep in people with PD.
Alternative Therapies for ADL Performance
Fourteen studies used alternative therapies to address ADL performance. These alternative therapies include the following:
Mindfulness meditation: Two studies provide moderate strength of evidence that mindfulness meditation group programs can significantly improve ADL performance (Advocat et al., 2016, Level 2b; Son & Choi, 2018, Level 1b).
Gaming: Moderate strength of evidence supports the use of gaming interventions to improve ADL performance. Four studies using the Xbox (Özgönenel et al., 2016, Level 2b), Wii (Gonçalves et al., 2014, Level 3b; Herz et al., 2013, Level 3b), and Kinect (da Silva Souza et al., 2018, Level 3b) gaming platforms all resulted in significantly improved ADL performance.
Tai chi: Low strength of evidence for the use of tai chi to improve ADL performance is available from a small number of low-quality studies with conflicting results. Choi (2016, Level 2b) found that tai chi resulted in significantly improved ADLs; however, Nocera et al. (2013, Level 2b) found no change in ADLs after a tai chi intervention.
Ai chi and aquatic therapy: Low strength of evidence for ai chi (tai chi movement patterns completed in an aquatic environment) and aquatic therapy is available from a small number of studies with inconsistent results. Two Level 2b studies used the same ai chi protocol (Pérez de la Cruz, 2017, 2018), but significant ADL improvement was seen only in the 2017 study. Villegas and Israel’s (2014, Level 2b) ai chi study showed significant improvement in ADLs. A study comparing “obstacle” and traditional aquatic therapy resulted in significantly improved ADL performance for both intervention groups (Zhu et al., 2018, Level 2b).
Dance: Low strength of evidence for the use of dance to improve ADLs is available from one study. The study compared a tango dance intervention to a no-treatment control condition and found no significant improvement in ADLs (Duncan & Earhart, 2012, Level 1b).
Singing: Low strength of evidence for the use of singing to improve swallow function is available from one study. Participants who performed singing exercises either once or twice a week showed significantly improved laryngeal function for swallowing (Stegemöller et al., 2017, Level 2b).
Alternative Therapies for Sleep
Four studies used alternative therapies to address sleep performance, providing moderate strength of evidence for the efficacy of alternative therapies to improve sleep. Three intervention methods positively affected sleep: Group meditation-based exercise significantly improved sleep disturbance (Son & Choi, 2018, Level 1b), full body massage significantly improved sleep quality (Skogar et al., 2013, Level 2b), and bright light therapy resulted in significantly less insomnia (Martino et al., 2018, Level 3b). In addition, sleep quality decreased significantly for a hatha yoga group compared with a no-treatment control group (Cheung et al., 2018, Level 2b).
Cognitive–Behavioral Therapy
Two RCTs were related to the efficacy of CBT interventions to improve sleep, providing moderate strength of evidence supporting the use of CBT to improve sleep in people with PD. CBT combined with bright light therapy reduced insomnia and improved sleep compared with a placebo intervention (Rios Romenets et al., 2013, Level 2b). Participants in an online CBT program for insomnia showed significant improvements in sleep compared with a standard intervention to promote sleep (Patel et al., 2017, Level 2b).
Discussion
In this SR, we examined the evidence for interventions within the scope of occupational therapy practice to support the performance of ADLs and sleep in people with PD. The studies included were grouped into four intervention themes: rehabilitation, physical exercise, alternative therapies, and CBTs.
Strong evidence from multiple high-quality studies supports inpatient MIRT to improve ADL function in people with PD, and moderate evidence indicates that MIRT can improve sleep performance. Low strength of evidence indicates that resistance exercise programs can improve ADLs, but moderate strength of evidence indicates that group and individual multimodal exercise programs can do so. Moderate strength of evidence supports targeted exercise programs (oral motor, pelvic floor, hand) to improve ADLs and resistance exercises and multimodal exercise to improve sleep. Several alternative therapies had a positive impact on ADLs and sleep, and moderate evidence supports CBT interventions to improve sleep.
The previous SR by Foster et al. (2014) found no studies that measured sleep or rest as an outcome. The inclusion of ADL and sleep outcome measures in the studies in the current review reflects a positive trend away from measuring only impairments (e.g., strength, memory) in people with PD. Like the previous SR, ours found few studies of typical occupational therapy interventions such as ADL training, environmental or task modifications, occupational performance interventions, functional mobility training, and LSVT–BIG programming. Despite improvements in the number of studies using ADL outcomes, we noted weaknesses in instrument selection. The most frequently used tools to measure ADLs were the UPDRS and the PDQ–39, both patient-reported instruments. Self-report assessments have been shown to have less accuracy than therapist-rated assessments, with self-rated assessment results skewed toward better performance (Marks et al., 2019).
Limitations
We reviewed 45 studies, but more may exist that we were unable to identify. Non-English-language articles may also exist but were not included. Only 10 studies were Level 1b high-quality RCTs. Many of the others had small samples and did not report blinding of assessors or participants. Because the interventions studied were dissimilar and patient populations tend to be inherently diverse, the findings of this review should be interpreted with caution. The use of varied outcome measures across studies may have affected our findings. We did not review studies that met the inclusion criteria but were of low quality or reported duplicate results because of length considerations. Meta-analysis of the data reported in the studies might have provided further clarity of results.
Implications for Occupational Therapy Practice and Research
Many treatment interventions identified in this SR resulted in improved ADL and sleep performance in people with PD. Most interventions could be implemented by occupational therapy practitioners either with or without further training. Unfortunately, the efficacy of common occupational therapy interventions to improve ADLs, rest, and sleep have not been studied with people with PD. We strongly recommend that future researchers study the efficacy of occupational therapy interventions such as ADL training, environmental and task adaptation, graded occupational performance, and functional mobility training with people with PD. Additionally, because of the potential for inaccuracies in self-report measures and poor sensitivity in some ADL outcome tools, more therapist-rated, objective methods for measuring ADL task performance are needed. Such methods might include measuring efficiency by timing ADL tasks or using tools such as the Assessment of Motor and Process Skills or the Physical Performance Test as ADL measures. The sleep measures used in the included studies appear to be sound tools that may be effective in future research.
Footnotes
Acknowledgments
This systematic review was funded and supported by the American Occupational Therapy Association; the authors were provided an honorarium for this work. The authors have no conflict of interest to report.
Appendix. Evidence and Risk-of-Bias Tables for the Systematic Review
Risk-of-Bias Table for Noncontrolled Studies
| Citation | Study Question or Objective Clear | Eligibility or Selection Criteria Clearly Described | Participants Representative of Real-World Patients | All Eligible Participants Enrolled | Sample Size Appropriate for Confidence in Findings | Intervention Clearly Described and Delivered Consistently | Outcome Measures Prespecified, Defined, Valid and Reliable, and Assessed Consistently | Assessors Blinded to Participant Exposure to Intervention | Loss to Follow-Up After Baseline ≤20% | Statistical Methods Examine Changes in Outcome Measures From Before to After Intervention | Outcome Measures Were Collected Multiple Times Before and After Intervention | Overall Risk of Bias Assessment |
| Argolo et al. (2013) | Y | Y | Y | Y | N | N | Y | Y | Y | Y | N | M |
| Athukorala et al. (2014) | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | L |
| da Silva Souza et al. (2018) | N | Y | Y | NR | N | Y | Y | NR | Y | Y | Y | M |
| Gonçalves et al. (2014) | Y | Y | Y | Y | N | N | Y | NR | Y | Y | N | M |
| Herz et al. (2013) | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | N | L |
| Martino et al. (2018) | Y | Y | Y | Y | Y | N | N | N | Y | Y | N | M |
| Stegemöller et al. (2017) | Y | Y | Y | N | N | N | Y | N | Y | Y | N | M |
| Vaughn et al. (2011) | Y | Y | Y | Y | N | Y | N | Y | Y | Y | N | M |
Note. N = no; NR = not reported; Y = yes. Adding Yes scores for each item and dividing by 11 yields an overall risk-of-bias rating: L = low overall risk (75%–100%); M = moderate overall risk (25%–75%). Risk-of-bias tool adapted from Quality Assessment Tool for Before–After (Pre–Post) Studies With No Control Group, by National Heart, Lung, and Blood Institute, n.d. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
Citation: Doucet, B. M., Franc, I., & Hunter, E. G. (2021). Interventions within the scope of occupational therapy to improve activities of daily living, rest, and sleep in people with Parkinson’s disease: A systematic review (Table A.3). American Journal of Occupational Therapy, 75, 7503190020. https://doi.org/10.5014/ajot.2021.048314
*
Indicates articles included in the systematic review.