
Abstract
Findings in this study of combined physical and cognitive training may help refine current protocols and facilitate development of personalized combined training programs for older adults with cognitive impairments.
Combined physical and cognitive training has been proposed as one promising approach for improving cognitive function among older adults with cognitive decline. Studies have shown that combined training has enhanced cognitive performance in various cognitive–motor domains, including memory, processing speed, and executive function, among older adults with cognitive impairment (Law et al., 2014). Nevertheless, cognitive impairment is heterogeneous among older adults. These individual differences may affect older adults’ responses and the cognitive domains that may benefit from combined training. It is important to examine how baseline global cognitive function influences the effects of combined training to optimize treatment efficacy and to identify appropriate participants for combined training.
Both high (Fairchild et al., 2013) and low (Kalbe et al., 2018) levels of baseline cognitive function were found to be associated with greater training gains. However, most current studies enrolled only healthy older adults and provided cognitive interventions alone. Only one study to date has examined the relationship between baseline cognitive impairment and cognitive improvements after combined training among both healthy older adults and older adults with cognitive impairment (Bamidis et al., 2015); in this study, a trend of differential cognitive improvements was observed between the two groups, indicating that baseline global cognitive function may affect cognitive outcomes during combined training.
Moreover, cognitive function is a multifaceted phenomenon consisting of multiple cognitive domains, including high-level domains (e.g., memory and executive function) and low-level domains (e.g., processing speed; Stuss & Benson, 1984). Each domain involves different neurocognitive processes (Stuss & Benson, 1984); as a result, the impact of baseline global cognitive function on cognitive outcomes may be different between cognitive domains. Nevertheless, most combined training studies have not evaluated the impact of baseline cognitive function on both high- and low-level cognitive domains among older adults with cognitive impairment (Law et al., 2014). How these cognitive domains are modulated by baseline global cognitive function during combined training remains uncertain.
Aside from cognitive outcomes, functional outcomes, such as instrumental activities of daily living (IADL) function, may also be affected by people’s baseline cognitive function. IADLs involve high-order reasoning and organization skills and often deteriorate with increasing cognitive impairment (Jekel et al., 2015). Understanding how baseline global cognitive function influences IADL recovery after combined training would help occupational therapy practitioners to modify current combined training protocols to facilitate restoration of IADLs among older adults with cognitive decline.
The purpose of this study was to determine the impact of baseline global cognitive function on cognitive and IADL outcomes after combined training among older adults with cognitive decline. We enrolled older adults with different levels of baseline function (i.e., mild cognitive decline [MCD] vs. moderate to severe cognitive decline [MSCD]) and assessed their cognitive changes in the high- and low-level cognitive domains. Our hypotheses were developed on the basis of a theoretical model of cognitive function (Dams-O’Connor & Gordon, 2013). In this model, cognitive processes are hierarchically organized into a pyramid in which the fundamental cognitive skills (e.g., processing speed) are located at the lower level, and the complex cognitive skills (e.g., executive function and memory) are located at the higher level. The lower level cognitive function supports the execution of the higher level cognitive function. Because older adults with MCD still have relatively preserved fundamental cognitive function, it is possible that combined training would build on those lower level cognitive skills to enhance restoration of higher level cognitive function.
By contrast, fundamental cognitive function may already be impaired among older adults with MSCD; thus, improving higher level cognitive function may be difficult for these participants. Combined training may improve general cognitive function and the lower level cognitive domains to restore the foundation of higher level cognitive domains. Therefore, we hypothesized that participants with MCD would have greater improvements in the high-level cognitive domains (i.e., executive function, including inhibitory control, task-switching abilities, and working memory) than participants with MSCD. These participants may be able to generalize the learned cognitive ability to IADLs. By contrast, we hypothesized that participants with MSCD would have greater improvements in general cognitive function and the low-level cognitive domains (i.e., processing speed).
Method
The data for this study were extracted from those of a large clinical trial investigating the effects of frequency of combined training among older adults with cognitive decline (registered at ClinicalTrials.gov [NCT03619577]). The participants (N = 91) who received one session of training per week in that clinical trial were included in the present analyses. Participants were recruited from local communities and senior centers. The inclusion criteria were (1) age ≥60 yr, (2) ability to follow the study instructions (Mini-Mental State Examination scores ≥17; Folstein et al., 1975), (3) having self- or informant-reported memory or cognitive complaint, (4) having no diagnosis of Alzheimer’s disease or other types of dementia, and (5) ability to safely participate in training with adequate cardiopulmonary function. The exclusion criteria were (1) unstable medical conditions (e.g., myocardial infarction in the prior year), (2) concomitant neurologic disorders, (3) participation in other studies, and (4) inability to provide informed consent. Participants with Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005) scores ≥23 but <30 were classified as participants with MCD, and those with MoCA scores <23 were classified as participants with MSCD (Carson et al., 2018). The local ethics board approved all procedures.
Participants practiced physical activity training for 45 to 55 min followed by 45 to 55 min of cognitive training at each session for one session per week for 12 wk. The physical activity training included cardiovascular exercise, core and limb muscle strengthening, resistance training, flexibility, and balance training. Each session consisted of a 5- to 10-min warm-up, 35 to 40 min of physical activity training, and a 5-min cooldown. Training modalities included arm, wrist, and ankle weights; resistance and stretching bands; and exercise balls. These modalities were selected because they were easy for adults in the community to carry out and practice, and they were commonly used modalities for physical activity training (Law et al., 2014). Participants exercised in a classroom with a group-based format. Five to 10 participants formed a group. A trained occupational therapist led the training session. After completing physical activity training, participants stayed in the same classroom and participated in the cognitive training in the same group-based format and led by the same occupational therapist.
The cognitive training used a structured multidomain approach. The cognitive domains for training included attention, visual and verbal memory, processing speed, and executive function. The first 20 min were focused on training a specific cognitive domain. For example, to train visual attention, participants were asked to identify a target that was different from the others in a picture. The next 20 min were focused on training multiple cognitive domains. For example, to train inhibitory control, processing speed, and visual attention, participants were asked to raise their arms when they saw a target picture but to keep their arms relaxed when irrelevant pictures appeared. The final 10 to 15 min were used to consolidate the newly acquired skills. The instructor gave feedback to each participant and discussed strategies to improve performance. The instructor followed a standard curriculum but allowed discussions on the basis of the participants’ needs.
Participants were assessed within 1 wk before and after training by evaluators blinded to the purpose of this study. The outcome measures are commonly used to assess cognition and IADLs among older adults and have good reliability and validity. The MoCA was used to assess general cognitive status (Nasreddine et al., 2005). The standard error of measurement (SEM) of the MoCA was established as 1.5 (Feeney et al., 2016). The Digital Symbol Substitution Test (DSST) from the Wechsler Adult Intelligence Scale (Wechsler, 1981) was used to evaluate information processing speed. The Word Recall Test (WRT) from the Wechsler Memory Scale–Third Edition (Wechsler, 1997) was used to assess working memory (Kent, 2013). The total number of words recalled in the word list for four trials were summed to represent working memory capacity. The Stroop Color and Word Test (SCWT) was used to examine inhibitory control (MacLeod, 1991). The differences in time (in seconds) between the congruent and incongruent subtests were used. The Trail Making Test (TMT; Parts A and B) was used to assess task-switching ability (Sánchez-Cubillo et al., 2009). The difference score (B − A) was used as the outcome. The Lawton–Brody Instrumental Activities of Daily Living Scale (Lawton–Brody IADL) was used to evaluate IADLs for living independently in the community (Lawton & Brody, 1969). The ordinal score system (score ranging from 1 to 5 with a summed score of 31) was used.
We compared baseline characteristics between MCD and MSCD groups using the independent t test for continuous variables and the χ2 test for categorical variables. We compared changes in outcomes using the two-way, mixed-design analyses of variance with group (MCD vs. MSCD) as a between-subjects factor and time (pre- vs. posttraining) as a within-subject factor. The effect size of ηp 2 was calculated to represent the magnitude of interaction and main effects. A ηp 2 > .14 represented a large effect, a ηp 2 of .06 represented a moderate effect, and a ηp 2 of .01 represented a small effect (Portney, 1993). The paired t test was used as the post hoc test to evaluate directional changes from pre- to posttraining within groups. The effect size d (Cohen’s d) was calculated to indicate the magnitude of changes from pre- to postintervention.
The baseline characteristic variables were treated as covariates if they significantly differed between groups at baseline, and an additional within-subject analysis of covariance was then performed to evaluate effects involving the covariates (Schneider et al., 2015). Because our hypotheses were based on the hierarchical model of cognitive function, we further explored whether the levels of baseline global cognitive function (i.e., the baseline MoCA scores) would affect changes in outcomes using the Pearson correlation coefficient. We analyzed data using PASW Statistics (Version 18.0).
Results
The adherence and compliance of the participants were good. All enrolled participants completed all of the training sessions and the assessments. Both groups differed significantly in initial MoCA scores, t(89) = −12.66, p < .001 (Table 1). No between-groups difference was found in educational level, t(89) = −1.46, p = 1.25, or gender, χ2(1) = 0.53, p = .47. However, the MSCD group was significantly older than the MCD group, t(89) = 4.32, p < .001. As a result, we treated age as a covariate using the within-subject analysis of covariance. The result showed that age did not affect changes of all outcomes from pre- to posttraining (Age × Time; MoCA, p = .6; Lawton–Brody IADL, p = .32; DSST, p = .22; WRT, p = .12; SCWT, p = .39; TMT, p = .9). Significant main effects of group were found for all outcome measures, and significant main effects of time were found for all outcomes except the SCWT, F(1, 89) = 1.01, p = .32, and TMT, F(1, 89) = 0.98, p = .32 (Table 2).
Baseline Characteristics of Participants
Note. MCD = mild cognitive decline; MoCA = Montreal Cognitive Assessment; MSCD = moderate to severe cognitive decline.
Results of the Two-Way Mixed Analysis of Covariance
Note. DSST = Digital Symbol Substitution Test; Lawton–Brody IADL = Lawton–Brody Instrumental Activities of Daily Living Scale; MoCA = Montreal Cognitive Assessment; SCWT = Stroop Color and Word Test; TMT = Trail Making Test, Parts A and B; WRT = Word Recall Test.
Significant interaction effects were found for the MoCA, F(1, 89) = 13.16, p < .001, ηp 2 = .13; Lawton–Brody IADL, F(1, 89) = 7.16, p = .009, ηp 2 = .07; WRT, F(1, 89) = 9.07, p = .003, ηp 2 = .09; and SCWT, F(1, 89) = 19.65, p < .001, ηp 2 = .18. The post hoc tests showed that the MoCA and Lawton–Brody IADL scores significantly improved from pre- to posttraining in the MSCD group—MoCA, t(39) = −4.69, p < .001; Lawton–Brody IADL, t(39) = −2.92, p = .006—but not in the MCD group—MoCA, t(50) = −0.56, p = .58; Lawton–Brody IADL, t(50) = −1.5, p = .14 (Table 3 and Figure 1). Conversely, the SCWT scores significantly improved from pre- to posttraining in the MCD group, t(50) = 3.37, p = .001, but declined in the MSCD group, t(39) = −2.94, p = .006. The WRT scores improved from pre- to posttraining in both groups but were greater in the MCD group, t(50) = −6.49, p < .001, than the MSCD group, t(39) = −2.18, p = .04. Although the Group × Time interaction was not significant for the TMT, TMT scores improved from pre- to posttraining in the MCD group (pretraining, M = 14.20, SD = 13.69; posttraining, M = 9.23, SD = 8.22; Δ = −4.86), t(50) = 2.7, p = .01, d = 0.44, but not in the MSCD group (pretraining, M = 30.19, SD = 27.58; posttraining, M = 30.02, SD = 29.3; Δ = −0.17), t(39) = 0.03, p = .98, d = 0.01. Both the MCD group (pretraining, M = 49.57, SD = 16.62; posttraining, M = 52.51, SD = 17.97), t(50)= −2.87, p = .006, d = 0.17, and the MSCD group (pretraining, M = 24.83, SD = 10.51; posttraining, M = 26.9, SD = 11.27), t(39)= −1.91, p = .06, d = 0.19, showed similar degrees of improvements for the DSST.
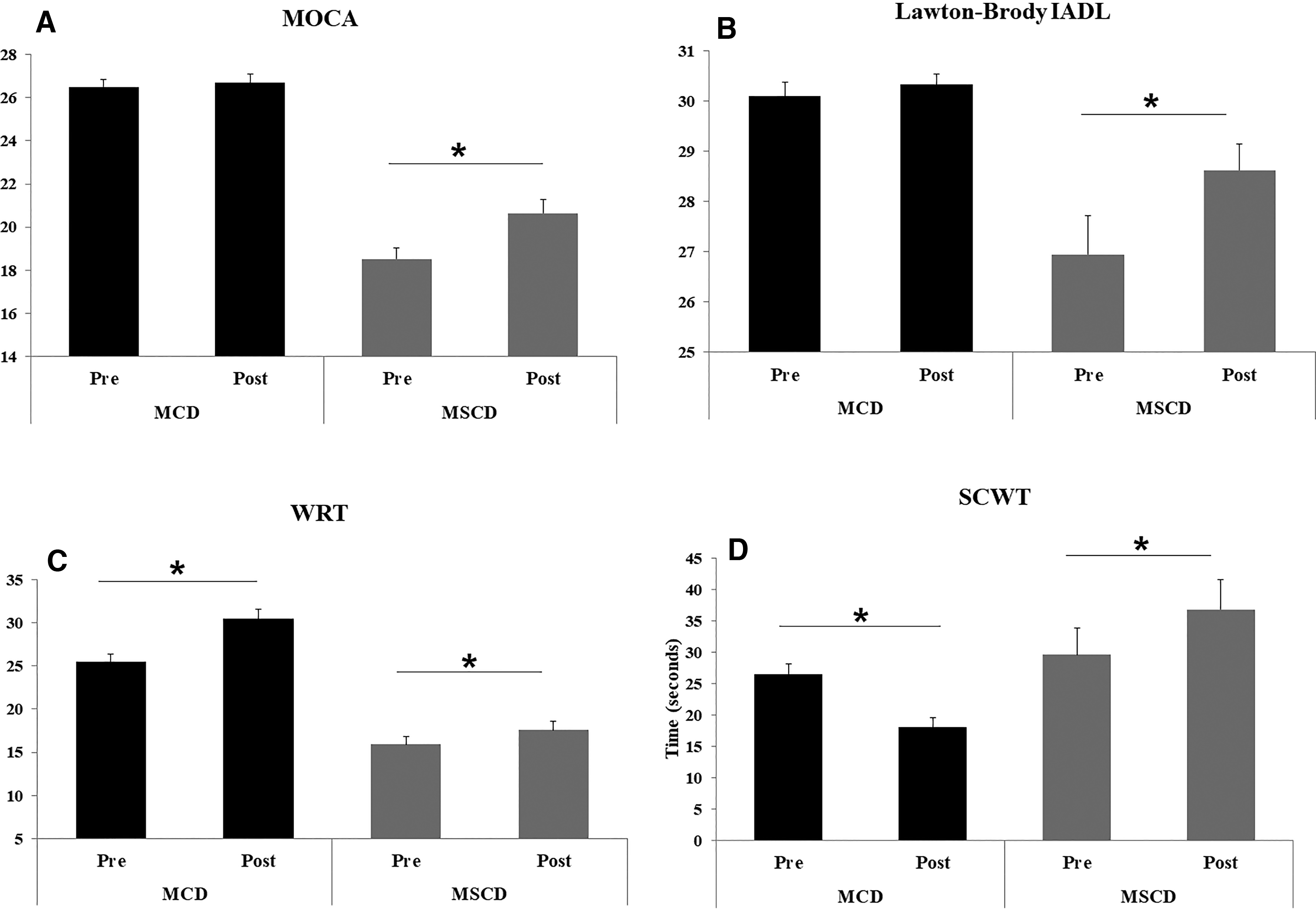
Score changes for the (A) MoCA, (B) Lawton–Brody IADL, (C) WRT, and (D) SCWT among the MCD and MSCD groups.
Results of the Within-Group Differences
Note. Lawton–Brody IADL = Lawton–Brody Instrumental Activities of Daily Living Scale; MCD = mild cognitive decline; MoCA = Montreal Cognitive Assessment; MSCD = moderate to severe cognitive decline; SCWT = Stroop Color and Word Test; WRT = Word Recall Test.
Significant correlations were found between the baseline MoCA scores and the changes in scores on the MoCA (r = −.41, p < .001), Lawton–Brody IADL (r = −.37, p < .001), SCWT (r = −.34, p = .001), and WRT (r = .32, p = .002). No correlations were found between the baseline MoCA scores and changes in DDST (p = .86) and TMT (p = .66) scores.
Discussion
We identified differential changes in the global and specific cognitive domains and IADLs between MCD and MSCD groups. Participants with MCD had greater improvements in the high-level cognitive domains, including inhibitory control and cognitive flexibility, than participants with MSCD. These participants could suppress the unwanted reactions, respond only to the task-relevant stimulus, and alternate their focuses between two relevant stimuli much faster than before training. Working memory capacity also increased more in the MCD group than the MSCD group. By contrast, participants with MSCD demonstrated improvements in general cognitive function and IADLs. Processing speed increased in both groups.
Moreover, we identified a negative relationship between participants’ baseline cognitive function and changes in general cognitive function and IADLs after combined training, indicating that participants with more impaired initial cognitive function improved more in fundamental cognitive skills and IADLs than those with preserved initial cognitive function. In contrast, a positive relationship was identified between baseline cognitive function and memory capacity as well as between inhibitory control and cognitive flexibility changes, suggesting that participants with preserved initial cognitive function improved more in high levels of cognitive function than those with more impaired cognitive function after combined training. These findings were mostly in line with the hypothesized hierarchical cognitive model, except for the IADL domain.
To our knowledge, this study is the first to indicate the differential benefits of combined training on cognitive and IADL outcomes among older adults with different baseline cognitive function. Consistent with our hypotheses, we found positive changes in executive function predominantly among participants with MCD. This result indicates that baseline cognitive function may affect how participants respond to combined training and, more important, the specific cognitive domain that might benefit from training. In particular, restoration of higher level cognitive function may depend on the integrity of overall cognitive function. Indeed, executive function is a unified and diverse process that involves basic neurocognitive function (Miyake et al., 2000). Performance on executive function tasks has also been found to be associated with basic cognitive ability (e.g., processing speed; Salthouse, 1996). Therefore, a preserved overall cognitive function might be a potential prerequisite for restoring higher level cognitive function during combined training.
We also found a greater increase in working memory capacity among participants with MCD than among participants with MSCD. This result again suggests that working memory recovery may be influenced by the integrity of global cognitive function. However, different from the result for executive function, participants with MSCD also exhibited improved working memory capacity, although not as much as participants with MCD. This result is similar to findings of previous studies that showed that working memory improvement was positively correlated with participants’ baseline performance (Bürki et al., 2014 Lövdén et al., 2012). Those studies, however, included only healthy adults. Our study expands on the findings of those previous works and identifies a similar trend of interindividual responses for combined training among older adults with cognitive decline.
Contrary to our hypotheses, participants with MCD did not show significant IADL improvements. This outcome may be because of the ceiling effect of subjective IADL measures. Most participants with MCD were already performing IADLs independently and had obtained high scores on the Lawton–Brody IADL measure before training. As a result, the effects of combined training may be underestimated in these participants. To minimize this potential confounding factor, we strongly recommend that occupational therapy practitioners include various performance-based IADL assessments. Performance-based IADL measures require people to perform IADL tasks in real time and may be more sensitive to detect IADL changes than subjective measures.
Including various types of IADL measures will also enable a comprehensive evaluation of IADL changes among participants with MCD. Similarly, we did not find significant improvement in global cognitive function in the MCD group, possibly because of ceiling effects of the MoCA. The participants with MCD had already achieved high MoCA scores at the baseline, thus leaving little room for improvement after combined training. In future studies, researchers could adopt multiple cognitive assessments, for example, computerized cognitive tests to complement the MoCA, and generate an appropriate global cognitive index for participants with MCD (Antony et al., 2017).
To our surprise, IADLs improved among the participants with MSCD. Compared with participants with MCD, participants with MSCD often experience greater IADL deficits, which accelerate deterioration of cognitive function and lead to dementia (McGuire et al., 2006). Combined training may be a potentially useful strategy to disrupt this vicious cycle by restoring IADLs. Our study also suggests that the participants with MSCD may still retain the cognitive plasticity to generalize the learned abilities for IADLs. The finding of increased general cognitive function along with improved IADLs may indicate a potential transfer from cognition to daily performance among these participants.
Our study supports the two competing views of interindividual differences on training gains, which are the magnification view and compensation view (Lövdén et al., 2012). The magnification view posits that people with better baseline cognitive performance benefit from training more than those with lower baseline cognitive performance because they have abundant neurocognitive resources to acquire and implement new strategies (Bürki et al., 2014). In contrast, the compensation view posits that people with good neurocognitive assets have already performed at their optimal levels and that no room is left for further improvements (Lövdén et al., 2012).
Our findings show that both views might be true because we did find benefits of combined training among participants with both high and low baseline cognitive levels. More important, we found that it was the targeted cognitive and functional domain that determined whether one view would outweigh the other. The magnification view may outweigh the compensation view with regard to high-level cognitive processes, whereas the compensation view may explain the interindividual differences in general cognitive status and IADLs. However, it is plausible that some low-level cognitive processes (e.g., processing speed) may be less likely to be affected by baseline cognitive function. The complicated interactions between targeted cognitive and functional domains and magnification and compensation views warrant further investigation.
Our study demonstrates that initial global cognitive function may affect restoration of both IADL and cognitive domains, which may have implications for restoration of functional cognition among older adults with cognitive decline. Functional cognition refers to the cognitive ability to perform common daily activities, and it is important for independent living (Giles et al., 2020). Functional cognition is also a critical domain for occupational therapy practice (Giles et al., 2020). On the basis of our findings, it is possible that functional cognition recovery may potentially be affected by initial global cognitive function because we found that IADL and cognitive domain changes depended on the levels of baseline global cognitive function. Older adults with MSCD may have a greater chance to recover functional cognition after combined training and, thus, may be suitable participants to receive combined training. However, we did not directly assess functional cognition using performance-based IADL measurements. In future studies, researchers could investigate whether initial cognitive function affects functional cognition restoration after combined training using performance-based measurements, such as the Assessment of Motor and Process Skills (Nygård et al., 1994) and the Performance Assessment of Self-Care Skills (Chisholm et al., 2014), or specific functional cognition involving common daily activities, such as the Kitchen Task Assessment (Baum & Edwards, 1993), among older adults with cognitive decline.
Limitations
Six limitations should be considered. First, the MSCD group was older than the MCD group. Nevertheless, our statistical analysis showed that age did not affect outcome changes and may be less likely to influence the study interpretation.
Second, although we provided evidence of interindividual differences in cognitive and functional changes, it may also be beneficial for future studies to assess neural mechanistic changes of the brain.
Third, no follow-up assessments were completed. Future studies could determine whether the domain-specific changes are maintained in the follow-up period.
Fourth, the differences between TMT–B and TMT–A were lower in our study than in a previous study (Tombaugh, 2004). This finding could be because of variabilities in performance between different samples and regions (Soukup et al., 1998). Older adults with cognitive decline were recruited in our study, whereas healthy older adults were enrolled in the previous study. Older adults with cognitive decline often have insufficient response inhibition ability (Wylie et al., 2007); as a result, when an error occurs during tests, they may have difficulty stopping the ongoing movements and correcting the errors, which consequently leads to shorter completion times. By contrast, healthy older adults can pause and spend time correcting the errors, thus resulting in longer completion times. Thus, further studies are needed to examine the TMT across different levels of cognitive function of older adults.
Fifth, the data of this study were extracted from a large clinical trial that examined the effects of high- versus low-frequency combined training among older adults with cognitive decline. Two reasons explain why we included the data of the low-frequency training group. First, previous studies have delivered low-frequency combined training; however, they only evaluated the treatment effects (Law et al., 2014). Our study provides additional information on how interindividual differences in baseline cognitive function might affect treatment effects of the low-frequency combined intervention. Second, the low-frequency training protocol is commonly implemented to improve physical and cognitive health among older adults in Taiwan. We believe our results are valuable for the health care system in Taiwan. Although the large clinical trial was not designed specifically to evaluate the impact of severity on participants’ recovery, the recruitment procedure, training duration, and frequency of this study were developed on the basis of the protocols of most combined training studies (Law et al., 2014). However, it is still possible that these procedures and parameters may not be optimal for the purpose of this study. Further studies will be needed to validate our findings.
Sixth, the results may not be applicable to older adults with a diagnosis of Alzheimer’s disease or other types of dementia because we did not include these older adults in our study.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: Baseline global cognitive function may need to be considered when providing combined physical and cognitive training for older adults with cognitive decline. Domain-specific improvements may be expected between older adults with MCD and older adults with MSCD after combined training. Our findings may be useful for identifying older adults who are suitable to receive combined training and for individualization of the combined training protocols.
Conclusion
Our study indicates that baseline global cognitive function may affect cognitive and functional outcomes regarding combined physical and cognitive training among older adults with different levels of cognitive decline. High-level cognitive abilities, such as memory and inhibitory control, improved among participants with preserved cognitive function, whereas general cognitive function and IADLs improved among participants with MSCD. This information may help occupational therapy practitioners to identify older adults who are appropriate to receive combined training and to facilitate development of a personalized combined training plan.
Footnotes
Acknowledgments
This study was supported by Chang Gung Memorial Hospital (Grants CMRPD1F0411-413, CORPD1J0011, and BMRP553); the Healthy Aging Research Center; Chang Gung University, as part of the Featured Areas Research Center Program within the Framework of the Higher Education Sprout Project by the Ministry of Education in Taiwan (Grant EMRPD1I0451); and the Ministry of Science and Technology in Taiwan (Grant 106-2314-B-182-024-MY3).