
Abstract
This longitudinal study demonstrates statistically significant improvements in skill levels when comparing the use of a competency evaluation combined with an online multimedia manual handling learning system.
Safe moving and handling of people is an integral part of patient care, and a range of legislation and guidance is available to protect the health and well-being of employees in the United Kingdom (Health and Safety at Work etc. Act, 1974; Health and Safety Executive, 2004; Management of Health and Safety at Work Regulations, 1999; National Back Exchange, 2010; Smith, 2011). A study by Alnaser (2015) identified patient handling as the primary factor in musculoskeletal injuries experienced by 23% of occupational therapy practitioners over a 12-mo working period. Research suggests that, to decrease the risk of injury, educators of health care professionals (HCPs) should teach safe people handling techniques as standard practice (Nelson et al., 2007; Waters et al., 2006). However, evidence indicates that traditional manual handling training is largely ineffective in reducing back pain and back injury (Clemes et al., 2010) because appropriate techniques and evidence-based principles often do not transfer to the workplace (Haslam et al., 2007). A lack of opportunity to practice in the working environment (Brown & McCracken, 2009; Ling et al., 2011), combined with a lack of clear recollection of procedures and knowledge, may result in an increase in errors, resulting in increased risk of injury for the patient or employee.
Providing occupational therapy students with moving and handling skills training is essential to ensure that they have the necessary practical skills and foundational knowledge of back care and applicable legislation for safe practice. The College of Occupational Therapists (2006) has stated that institutions of higher education should provide students with generic manual handling training as part of their undergraduate training (Health and Care Professions Council [HCPC], 2013). A range of literature focusing on qualified HCPs has recommended that these skills be regularly updated, yet standardized delivery of practical skills training for undergraduate students varies across higher education institutions and may or may not be delivered as part of practice placement.
A key support provided by HCPs to both formal and informal caregivers is advice regarding safe people handling techniques to enable caregivers to support their family members (Royal College of Occupational Therapists, 2018). Bartley et al. (2015) cited the importance of HCPs having a combination of skills and knowledge of up-to-date equipment so that they can recommend safe handling interventions in a timely way. Before therapists can deliver safe advice and training to caregivers, however, it is essential that they be competent and confident in their own people handling skills, including knowledge of a range of people handling methods, equipment, and applicable legislation. Frost and Barkley (2012) advocated the development of new approaches to practical skills training to embed people handling skills while reinforcing HCPC’s (2013) recommendations that students take responsibility for their learning and professional accountability.
Electronic learning is the use of information and communication technologies, such as interactive web services, as tools to support the learning process, allowing learners to “access more diversified learning experiences without the limitations of time, space, and place” (Chen, 2011, p. 1501). Gallagher et al. (2014) compared DVD-assisted training and face-to-face instruction in completing a hoist transfer for final-year occupational therapy students (N = 12). They found no significant difference between the two groups, although they noted that students who received face-to-face training had higher levels of perceived confidence than those who engaged in DVD-assisted training. The use of videos as a training resource is known to be an effective addition to traditional training (Wieling & Hofman, 2010), providing the videos are relevant (Zhang et al., 2006), and result in improved learning goals (Blomberg et al., 2014; Seidel et al., 2013).
Online learning is now considered part of mainstream medical and health professional education (Masters & Ellaway, 2008; Miller et al., 2010). The multimedia A1 online learning system (A1 Risk Solutions® Ltd., Manchester, United Kingdom) incorporates a range of videos and learning resources to meet different learning styles. The system is designed to facilitate learning for all HCPs and covers a wide range of equipment and techniques that learners can access at any time, supporting the theory of just-in-time training. According to Tiernan (2014), this practice learning approach meets a learner’s need just before it is required, maximizing the educational outcome, and it is particularly effective when implementing practice guidelines. There is currently one other e-learning program specifically aimed at manual handling for use in a health care setting across medical and nursing groups (Anderson et al., 2014), but it is limited to a short online test and has a limited video base. Because of these limitations, we decided that the A1 online learning system was more appropriate to meet the needs of undergraduate occupational therapy students.
An earlier study by Webb et al. (2016) with volunteer undergraduate occupational therapy students (N = 130) demonstrated positive results from using videos from the A1 online learning system to reduce the risks for the handler and patients while increasing skills. The follow-up longitudinal study reported in this article evaluates the impact of replacing traditional tutor-led annual practical update sessions (3 hr duration) with the online A1 system and an individual 45-min competency evaluation.
Method
A quasi-experimental design in the form of a 3-yr longitudinal study was used to evaluate the impact of a change in teaching style on the development of people handling skills. As of September 2016, the pedagogical methods for moving and handling training were changed from annual tutor-led group practical updates to an individual classroom competency approach combined with access to the A1 online learning system. Practical updates for returning Year 2 and Year 3 students were removed and replaced with an annual 45-min competency evaluation (Table 1) consisting of four common moving and handling tasks. Only Year 1 students received practical hands-on sessions, after which they had access to all the learning resources and videos in the A1 online learning system for the remainder of their undergraduate training.
Change in Pedagogy
Participants
All students enrolled in the undergraduate honors occupational therapy program at the University of Salford were included in this study. All student participants (N = 243; see Supplemental Appendix Table A.1, available online with this article at https://research.aota.org/ajot) had completed the tutor-led moving and handling practical training in Year 1. Students were excluded if their weight exceeded the safe working load of the equipment, had not attended the Year 1 training, or had an existing medical condition or injury that prevented them from carrying out moving and handling techniques.
Procedure
Student participants attended an individual 45-min competency evaluation session in which they demonstrated their practical skills and competency in carrying out four common moving and handling tasks: (1) assisted sit-to-stand (Task 1a), (2) repositioning in a chair using a one-way glide sheet (Task 1b), (3) inserting a pair of flat slide sheets to move someone up on the bed (Task 2), and (4) fitting a universal sling in sitting and hoisting from a chair (Task 3). These tasks had been demonstrated to students and practiced as part of their Year 1 mandatory 6-hr training.
Three practical skill stations containing the moving and handling equipment necessary for each practical task were set up in one clinical room at the University of Salford. Each station included one patient and one assessor to maintain consistency throughout the data collection, and screens were used to ensure privacy and avoid students observing each other. Students were allocated 15 min for each station (including scoring time and brief feedback). On completion of the task, each student moved on to the next practical skill station until all three stations were completed (Tasks 1a and 1b were combined in one practical station completed in 15 min). The total time required for all three tasks was 45 min.
Assessors
To ensure objective and robust assessment of the practical tasks, assessors were recruited from the occupational therapy teaching team to observe the students carrying out each task and score their performance. To minimize assessor variability, all assessors attended training and debriefing sessions at the university before data collection. The study aims were outlined to the assessors, and role play was used to apply the Competency Assessment Tool (CAT; see the Supplemental Appendix, available online) to each task, ensuring a standardized and objective approach and minimizing misinterpretation of the evaluation tool. To improve reliability and consistency of scoring, each assessor was assigned to only one practical station (i.e., one specific moving and handling task).
Patients
To evaluate skills effectively without introducing any bias or assistance from fellow students, patients were recruited to take part in each of the three tasks to be assessed. The volunteer patients involved in the study were older people who were not known to the students (ethical approval was received from the University of Salford ethics panel, No. HSCR14/123). Before data collection, these volunteer patients were briefed on their role in each task. Risk assessments approved through university ethics procedures were adhered to throughout data collection, and there was no incidence of injury to students or patients throughout the 3-yr study. The patients were instructed to be cooperative but not to assist or prompt the students in any way during the assessment.
Outcome Measure: Competency Assessment Tool
The CAT (see the Supplemental Appendix) was developed using standard guidelines from The Guide to the Handling of People (Smith, 2011), using activity analysis of each manual handling task linked to risk assessment and safe practice. The CAT was piloted in a previous study (Webb et al., 2016), is used in the assessor training, and is now available as the Salford Moving and Handling Competency Passport (Webb & Harrison, 2019). The CAT generates three different scores: (1) skill level (elements of task performed correctly), (2) number of errors (elements of tasks performed incorrectly), and (3) assessor’s perception of the student’s level of safety.
Data were collected with the CAT at three critical stages of the undergraduate program (see Supplemental Appendix): (1) beginning of Year 2 (September 2016), (2) beginning of Year 3 (September 2017), and (3) end of Year 3 (June 2018).
Results
Baseline data from Webb et al. (2016) were used for each year group at each data collection point to compare students’ scores before and after the 2016 change in teaching style (see Table 1) and to measure the impact of access to the A1 online learning system on skill level and errors as students progressed through their undergraduate studies.
Normality analysis informed the use of parametric statistical tests, so after calculation of means and standard deviations, we used analysis of variance (ANOVA) to analyze data for all tasks to compare differences between the before and after September 2016 groups at the data collection points in 2016, 2017, and 2018. In addition to the ANOVA using Bonferroni post hoc tests, the means of several combinations of Year 2 and Year 3 data were analyzed via t tests using R (R Core Team, 2018). To avoid false-positive readings and increase the reliability of the multiple comparisons, the p values were adjusted using a false discovery rate (FDR) method (Pawitan et al., 2005). FDR is designed to control the expected proportion of incorrect rejections of the null hypotheses (false discoveries) and minimize the likelihood of these happening by chance; it is a less restrictive post hoc test than the Bonferroni, which reduces the probability of getting a false positive, but it can also increase the probability of getting a false negative (Pawitan et al., 2005).
Table 2 shows mean percentage scores for each task as the students progressed through the program and identifies the significance of comparisons of Year 2 at the September 2016 and September 2017 data collection points for Tasks 1b, 2, and 3 and of Year 3 at June 2017 and June 2018 data collection points for the same tasks. Overall, the results indicate that, in terms of learning and performance, the change in pedagogy had no detrimental effect on the post-2016 groups, despite a reduction in direct practical sessions, and on some tasks they outperformed the traditional training group each year.
Mean Percentage Score for Each Task at Each Data Collection Point With F Statistic and p Values After ANOVA With Bonferroni Correction
Note. Analysis of variance (ANOVA) indicates significance at the indicated comparisons.
p < .000.
p < .004.
p < .005.
p < .006.
Figure 1 shows multiple t tests comparing the performance of different cohorts of Year 2 and Year 3 students on four tasks. Control data for each year of study are included as comparators, with the average score achieved by students at each data collection point using the traditional tutor-led training with annual practical updates. In comparison with the pre-2016 group, students showed the most significant improvements on Tasks 2 and 3.
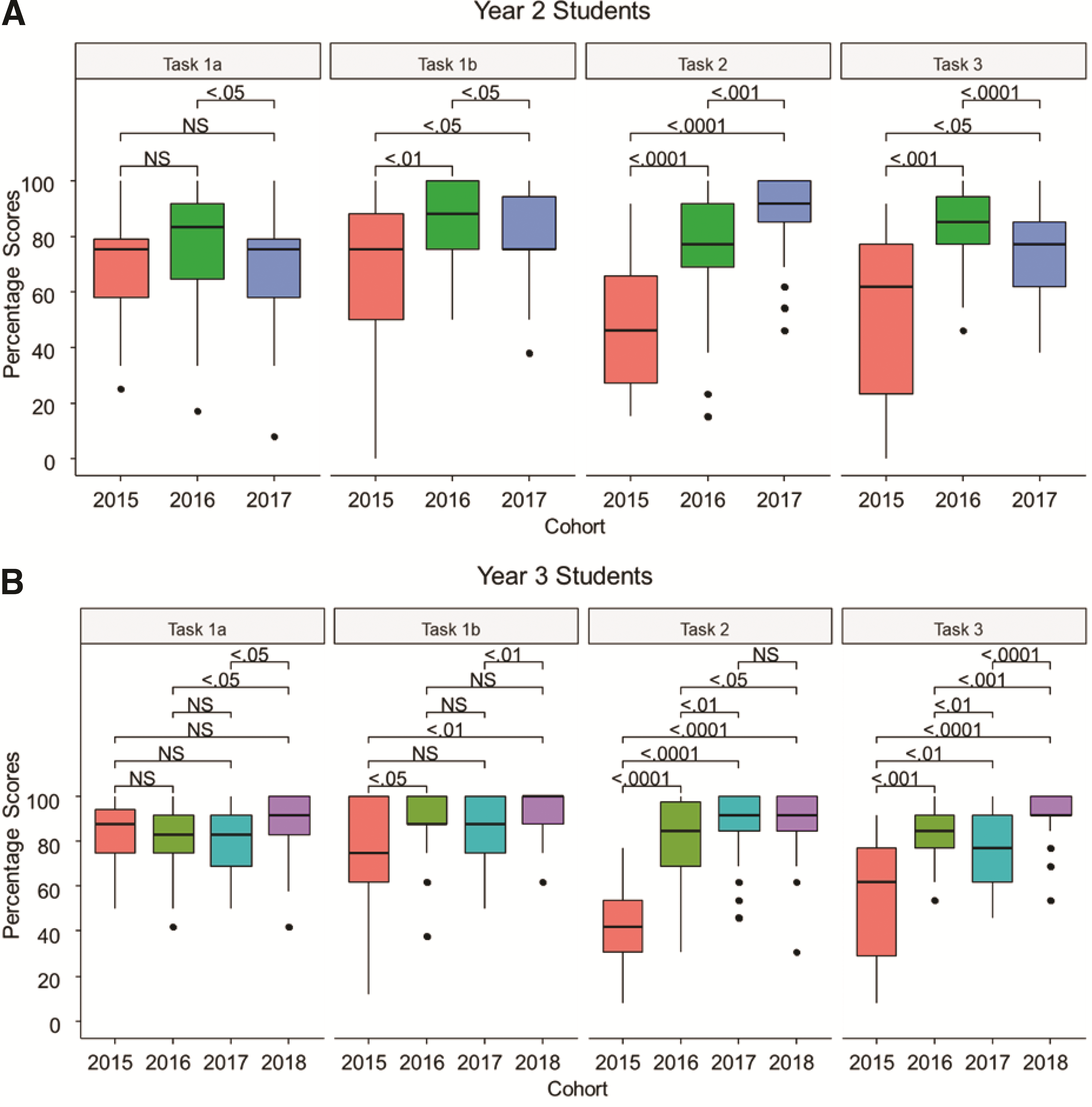
Progression in percentage scores across all tasks before 2016 teaching style (2015) compared with scores at (A) beginning of the year (September 2016 and 2017) for Year 2 students and (B) beginning of the year (September 2016 and 2017) and end of the year (June 2018) for Year 3 students.
A similar trend is observed for Year 2 and Year 3 students. To increase the reliability of the tests, p values were controlled via FDR rather than Bonferroni. Task 1b, 2, and 3 results for Year 3 students suggest a higher consistency in the scores obtained by the post–September 2016 groups. The variability of the scores obtained for those tasks is nearly always noticeably lower than the scores obtained by the pre–September 2016 group. For Tasks 2 and 3, this is confirmed by significantly low p values.
Safety Levels
After each task, the assessors were required to record whether they felt the student had displayed unsafe practice. Levels of safety at the final data collection point were significantly higher than those of Year 3 students who received traditional tutor-led training, with students who received the new competency approach scored at 100% safe on Task 1b (repositioning in chair using one-way glide sheet) and the more complex Task 3 (fitting a universal sling in sitting position to hoist from a chair). Students who received tutor-led training scored at 35% and 55% unsafe, respectively, on these tasks. Reductions in unsafe practice were also observed for Task 1a (assisted sit-to-stand), from 10% to 4%, and Task 2 (inserting flat slide sheets to move someone up on the bed), from 65% to 12%.
Discussion
Increased Scores and Improved Skills
Results overall indicate continued positive outcomes, with students performing better on the more complex tasks than those who received traditional training with tutor-led sessions and annual updates. Statistically significant increases in scores were noted for Tasks 1b, 2, and 3 among Year 3 students, with a significant rise in competency before final placement. Results in the final data set also indicate a reduced range in scores, reflecting a more consistent level of competency in the cohort rather than a wider range that would suggest some students were performing very well and others were just barely achieving competency, as can be seen in some of the data from before September 2016 for students who received traditional training. This interactive approach is supported by Kolozsvari et al. (2011), who substantiated the merits of overtraining to achieve a level of competence beyond a basic pass mark, which ultimately enhances skill transfer in practice. The findings support Barnes’s (1998) practice learning approach of just-in-time training with the on-demand learning and fresh revision of contents accessed via the A1 online learning system closer to the time of use, which had a positive impact on comprehension and retention of information and helped to reduce errors.
Increased Safety Levels
Significant increases in student safety levels as a result of the competency approach were noted, in particular on Task 3. This task is the most complex of the tasks, with 55% of students who received the tutor-led approach being identified as unsafe. Despite the lack of additional practical training, at the endpoint measurement in June 2018, 100% of Year 3 students observed performing this task were considered safe. A similar trend was observed with the second most complex task, Task 2, on which unsafe practices were reduced from 65% to 12%. Access to the A1 online learning system using a strategic approach may have led students to focus on what they considered to be the more complex tasks, watching the videos at a time that suited them to boost their confidence during the competency assessment. Gallagher et al. (2014) noted that video-assisted instruction offers the advantage of students being able to pace their learning and, as a permanent resource, allows repetitive practice to aid in development and retention of psychomotor skills (Stefanidis et al., 2006). This study’s findings support those of Van Bruwaene et al. (2009) and Gallagher et al., demonstrating that access to the online system, combined with practice in the competency sessions, increases proficiency in skill development.
Increased Responsibility for Learning by Accessing the Online System
As previous advocates of hands-on skill development through practical tutor-led sessions, removal of this opportunity initially challenged our beliefs. We considered it to be a bold step in pedagogical delivery style. The changes held significant risk: What if students did not engage with the online system? How would they respond to taking away the practical sessions? What could this mean for patient safety? How would educators perceive the changes? Would students fail on placement?
What has become clear is that access to the A1 online learning system is a permanent and readily accessible resource (unlike the face-to-face tutor-led sessions that occurred only once a year). Students have taken more responsibility for their own learning and professional development, demonstrating more positive engagement in preparation for the classroom competency session. This proactive approach is an improvement on the previous approach in which students attended an update session, signed the register, and were deemed competent to practice for another year. Although initial feedback from tutors is lacking when engaging with the online system, the competency evaluation process and CAT feedback (Webb & Harrison, 2019) meets Van Bruwaene et al.’s (2009) recommendations to further motivate students to increase their practical skills. A study by Hills et al. (2012) explored changes in educational approaches with typical Generation Y, tech-savvy occupational therapy students, identifying a shift to multimedia education methods, including online learning, recorded lectures, and e-books. The Hills et al. study identified emerging technology for developing competence in practice skills and supported the use of simulation for practice placement preparation and debriefing as an experience to produce skills or responses (Merryman, 2010). The combination of the online system and the competency evaluation meets the recommendations of both of these studies and supports their positive findings.
This approach is not unique to occupational therapy or the student community, and similar strategies could be advantageous for a range of qualified professionals in the health care community, helping to bridge the gap between traditional training and often poor engagement with mandatory update sessions. A combination of access to the system to complete tests and quizzes, and to reflect on set problems or hot topics in a work environment, offers an alternative and often more engaging approach to continuing professional development. The A1 system allows for continual updates, responding to the common errors identified as part of the research and any changes in guidance from professional bodies or industries in the moving and handling community. Learner engagement is easily tracked and provides evidence of access to safe techniques, which could be useful if any critical incidents needing investigation occur in a range of health and social care facilities.
Reduced Classroom Update Sessions
Rather than ticking off a box for mandatory training attendance every 12 mo, the A1 system offers access to support whenever the learner needs it. This is particularly useful when teaching clinical skills relatively early in professional programs that may not be revisited until a later date, such as on a clinical placement (Gallagher et al., 2014). In this way, the online system and competency approach acts as an aide memoire to encourage safe application of skills and support clinical reasoning by providing an evidence-based, 24/7 multimedia risk assessment tool, encouraging active engagement and regular skills updates. Our results demonstrate that skills have improved along with levels of safety, with a marked reduction in student anxiety, particularly in the weeks before placement, when numerous requests for additional practical sessions did not occur, again saving staff resources in the delivery of ad hoc practical workshops to help alleviate students’ concerns.
Limitations
This study challenged the traditional tutor-led style of training students in moving and handling skills and evaluated a huge change in learning and evaluation style with undergraduate occupational therapy students at the University of Salford. However, some limitations in the study design may need consideration when interpreting the results. The CAT used to collect data was not a validated tool, although it had been piloted in a previous study (Webb et al., 2016). Despite attempts to control intrarater reliability (training of assessors and using one assessor for the same task consistently throughout the study), assessors may still have lacked consistency (interrater reliability) when completing the CAT. Tutors used email prompts, posing questions and challenges, as a reminder to students to access the online system, but access ultimately relies on students being motivated and responsible for their learning. Limited technical ability or lack of internet access will affect the ability to access the learning materials online and therefore learning and skill development.
Implications for Occupational Therapy Education
This study has the following implications for occupational therapy education: Active engagement with the online system and the learning tools within it, combined with regular skill checking, encourages a learner-centered, problem-solving, and reflective approach to practical skill development using a just-in-time approach. The online system is suitable for providing skills updates and continuing professional development to a range of qualified therapists and caregivers. Students’ increased competency will promote enablement, patient safety, tissue viability, and harm-free care of service users. The use of an effective multimedia online moving and handling and risk assessment learning system combined with a competency assessment approach can reduce associated training costs.
Conclusion
This longitudinal study demonstrates statistically significant improvements in skill levels when comparing the use of a competency evaluation combined with an online multimedia manual handling learning system. Improvements in skill scores were highly significant (p ≤ .0001) for the more complex tasks of inserting flat slide sheets to move someone up on a bed and fitting a universal sling in sitting and hoisting from a chair. Students engaged well with the system, and by the end of Year 3 they were better equipped in their moving and handling skills despite less actual hands-on practical teaching of those skills. The A1 system is designed for use by a full range of health care practitioners and qualified and unqualified, formal or informal caregivers from a wide range of employers, statutory, voluntary, and private.
The results of this study support a shift away from the annual mandatory update model often used by both higher education institutions and health and social care providers. This competency approach, which results in improved skills and safety levels compared with a more passive tutor-led style, offers a solution that more effectively engages both students and registered practitioners in developing their skills and reinforces the value of just-in-time training (Tiernan, 2014) and the waste of resources invested in less effective annual updates (Brown & McCracken, 2009; Haslam et al., 2007; Ling et al., 2011). The Salford Moving and Handling Competency Passport, formerly the CAT, gives constructive, itemized feedback and identifies areas for future development to take into practice placement, encouraging a lifelong learning approach. The competency approach used in this longitudinal study continues to demonstrate encouraging and significant results and offers an evidence-based, sustainable, and effective alternative to tutor-led annual training to support a range of health care professions in keeping up to date with the necessary skills to support clients and caregivers in a range of care environments.
Supplemental Material
Supplementary material for Improving Competency in Safe Patient Handling Through Online Learning Beyond the Classroom: A Longitudinal Study
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.044388.pdf for Improving Competency in Safe Patient Handling Through Online Learning Beyond the Classroom: A Longitudinal Study by Jo Webb, Peter Hogg, Martin Twiste and Elon Correa in The American Journal of Occupational Therapy
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.