
Abstract
A review of electronic health records found that patients receiving occupational therapy services in the NCCU had a lower likelihood of community discharge; however, these findings may result from therapists’ consideration for the safest discharge location to ensure the greatest balance between independence and support.
Patients in the neurological critical care unit (NCCU) have complex needs that require multidisciplinary care by teams with expertise in managing patients with neurological conditions (Suarez et al., 2004). Published NCCU standards from the Neurocritical Care Society identify occupational therapists as essential NCCU personnel (Moheet et al., 2018). A systematic review of studies on occupational therapy in the medical intensive care unit concluded that a multidisciplinary approach including occupational therapy is important in delivering high-quality care with better outcomes (Eakin et al., 2015). However, studies on the relationship between occupational therapy and outcome indicators among neurological critical care patients are lacking.
Community discharge is generally considered a favorable hospital outcome for NCCU patients. Compared with patients discharged to an institution, patients discharged to the community have better long-term outcomes (Brown et al., 2020), have less costly health care (Werner et al., 2019), and have better quality of life (van Eeden et al., 2015). Given that occupational therapists in hospital settings target independent living skills, receipt of occupational therapy services may enable a safe community discharge for NCCU patients by restoring functional ability. Enabling a safe community discharge is complex, however, and it is likely influenced by patient factors not amenable to change in the acute care setting. For example, older patients and patients with higher comorbidity burden are more likely to receive occupational therapy services (Freburger et al., 2018), but they are also less likely to be discharged to the community (Kubo et al., 2021). In such cases, occupational therapists may advocate for discharge to another institution (e.g., skilled nursing facility, inpatient rehabilitation facility) as a safer discharge disposition for the patient. Thus, research is needed to determine the extent to which patient characteristics, receipt of occupational therapy services, and discharge disposition relate to one another.
The purpose of this study was to examine the extent to which patient factors and receipt of occupational therapy predict discharge disposition for NCCU patients. We hypothesized that receipt of occupational therapy services in the NCCU would be associated with discharge disposition and that this relationship would be moderated by both age and comorbidity burden.
Method
Design
We conducted a retrospective cross-sectional study of deidentified patient data to describe occupational therapy utilization and interventions in a NCCU at a large urban academic hospital. Average census for this unit was 21.4 patients, with one full-time-equivalent occupational therapist. Data were obtained from electronic health records (EHRs) for 1,134 adults (age ≥18 yr) admitted to the NCCU from May 2013 through September 2015. Patients younger than age 18 yr or with missing data were excluded from the study, resulting in a final sample of 1,035 patients. The study was approved by the local institutional review board.
Data Collection
Administrative data and data from occupational therapy flow sheets were extracted, checked for completeness, and validated. We determined the extent to which patient-related factors and receipt of occupational therapy predicted discharge disposition (the dichotomous dependent variable; community [home or supported living] or noncommunity [inpatient rehabilitation facility, skilled nursing facility, etc.]). We selected variables available in the EHR on the basis of the Behavioral Model of Health Services Use (Andersen, 1995), which advocates for the inclusion of predisposing (e.g., age, sex), enabling (occupational therapy use), and illness (e.g., comorbidity burden) factors in health services research. The following predictors were entered as independent variables: sex, age, minority status, length of stay (LOS) in the NCCU, baseline Glasgow Coma Scale (GCS) score, Elixhauser Comorbidity Index, and occupational therapy use. Minority status was dichotomized as racial or ethnic minority or nonminority. We used the total GCS score, which ranges from 3 to 15, with higher scores indicating a higher level of consciousness (Teasdale & Jennett, 1974). We calculated the Elixhauser Comorbidity Index by first using the ICD–9 and ICD–10 R package (Wasey et al., 2019) to evaluate the presence of comorbidities identified by Elixhauser et al. (1998). To evaluate the severity of comorbidity burden, we constructed a weighted summary index according to Moore et al. (2017).
Data Analysis
All analyses were performed using R (Version 3.6.2). We calculated descriptive statistics for the independent variables both across and within discharge disposition. We then specified a logistic regression model predicting discharge disposition (0 = noncommunity setting; 1 = community setting). All independent variables were entered simultaneously. Because we sought to examine whether the relationship between occupational therapy utilization and discharge disposition differed across patient characteristics, in addition to predictors, we entered interactions between occupational therapy utilization and other predictors. We set α = .05.
Results
Approximately 39% of the sample received occupational therapy services, and 74% were discharged to the community. The sample was evenly distributed with respect to sex (male = 51%, female = 49%), and the average age was 55 yr (SD = 16.0; Table 1). Logistic regression results revealed that older age, longer LOS, greater comorbidity burden, and receipt of occupational therapy services decreased the likelihood of being discharged to the community (Table 2).
Descriptive Statistics (N = 1,035)
Note. GCS = Glasgow Coma Scale; OT = occupational therapy.
Logistic Regression Model Predicting Discharge Disposition (N = 1,035)
Note. Continuous predictors are mean-centered. GCS = Glasgow Coma Scale; OT = occupational therapy; ref. = reference category.
p ≤ .05.
p ≤ .001.
Interaction results indicate that the relationship between occupational therapy utilization and discharge disposition differed by sex and age. Figure 1 illustrates that among women, occupational therapy utilization was associated with a decreased likelihood of community discharge (odds ratio [OR] = 0.37, 95% confidence interval [CI] [0.184, 0.562]), but this effect was more pronounced among their male counterparts (OR = 0.19, 95% CI [0.094, 0.288]). With respect to age, Figure 2 illustrates that although those who received occupational therapy were less likely to be discharged to the community relative to those who did not receive it, the effect dissipated among older patients. None of the other interactions reached statistical significance.
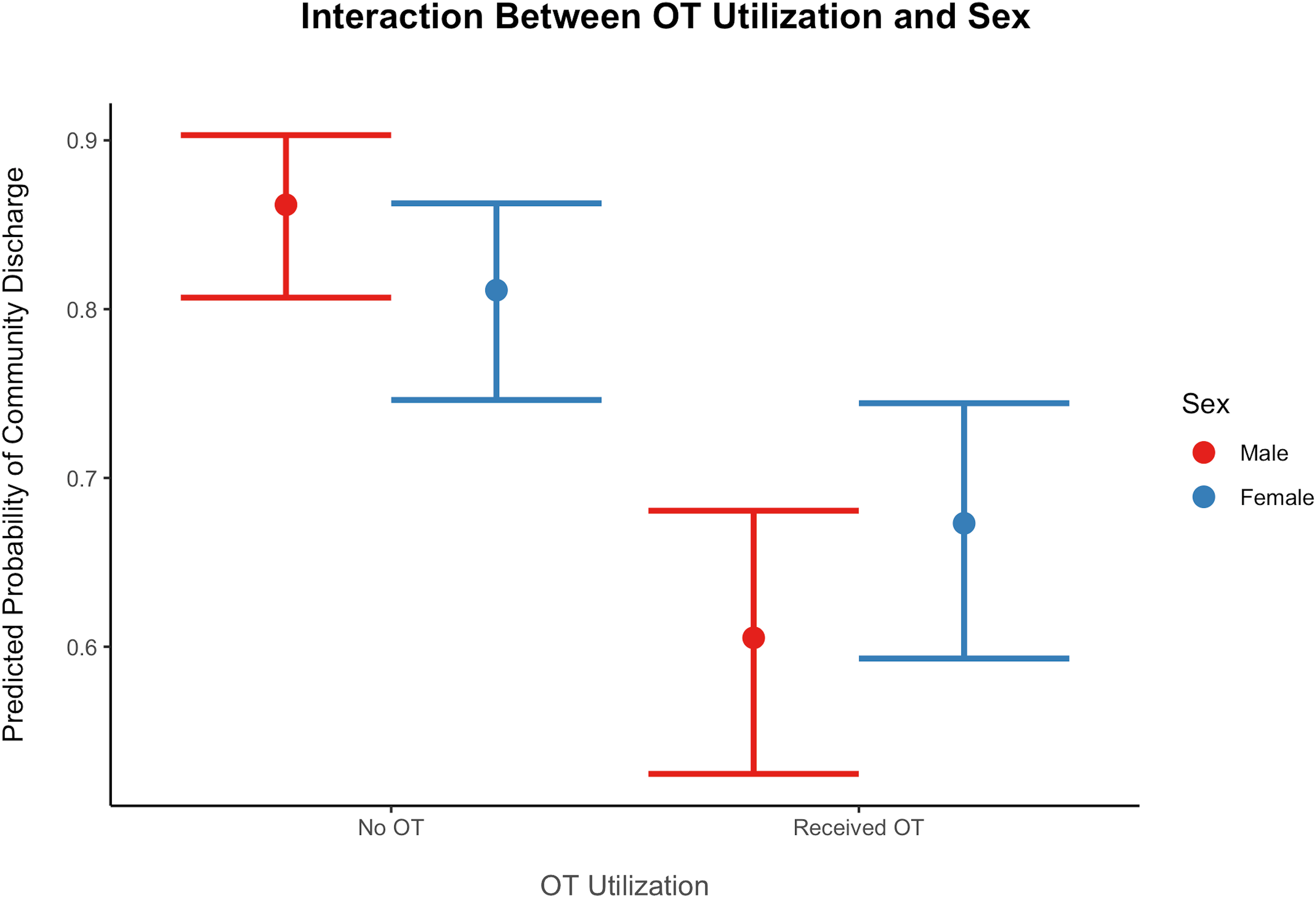
Plot of the interaction between OT utilization and sex in predicting community discharge.
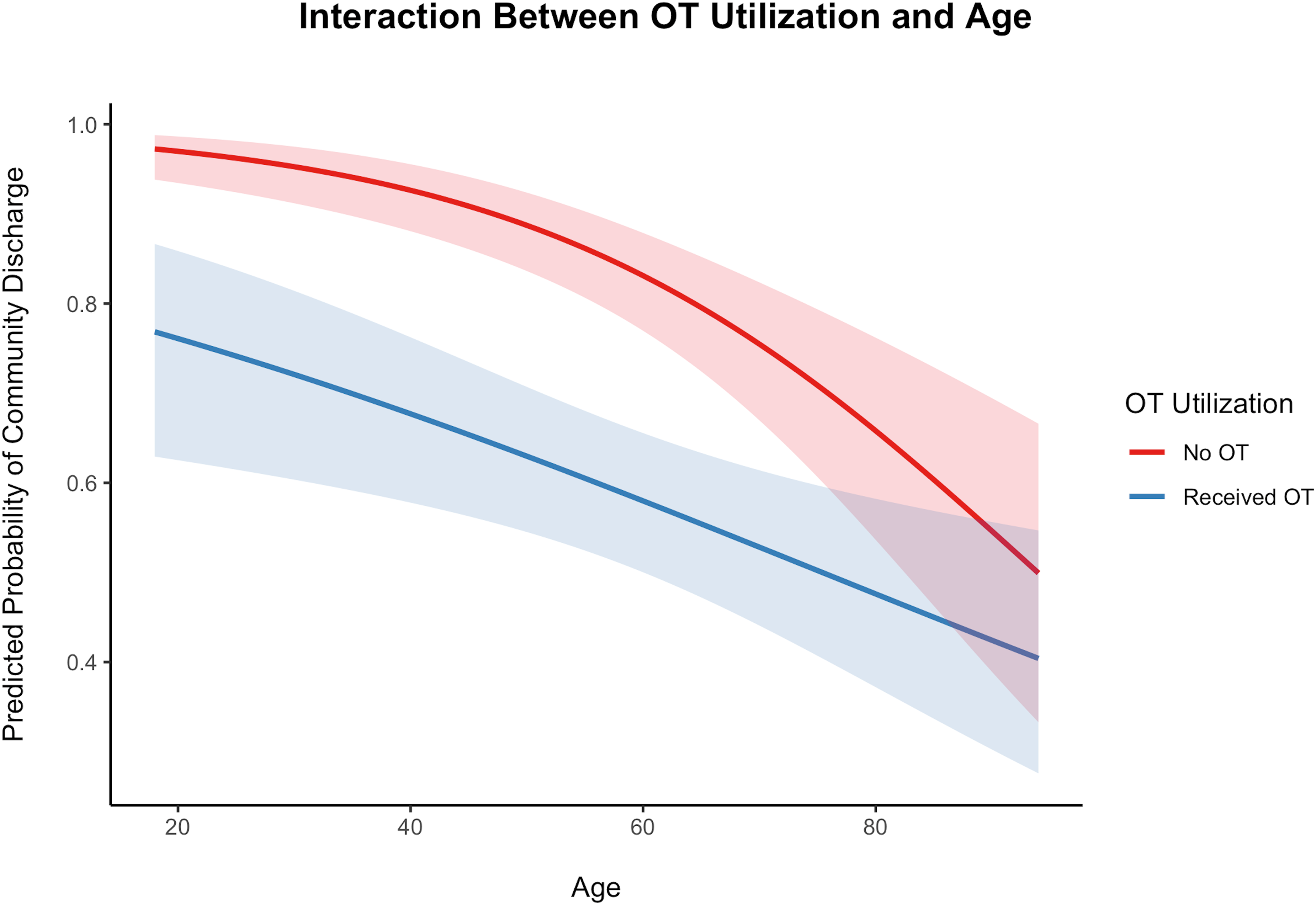
Plot of the interaction between OT use and age in predicting community discharge.
Discussion
Current health care policies emphasize community discharge as a quality indicator of acute care hospitalization (Centers for Medicare & Medicaid Services, 2019). The current study revealed that older patients, those with a greater comorbidity burden, and those who received occupational therapy in the NCCU were less likely to be discharged to their home or other community setting. Slightly more than one-third of our sample received NCCU occupational therapy services, and these patients had 75% lower odds for community discharge compared with nonrecipients. Although this may seem like a less than favorable outcome of occupational therapy, patient age, comorbidity burden, and occupational therapists’ discharge recommendations likely influence the relationship between receipt of occupational therapy and discharge disposition, as we describe next.
The probability of community discharge differed between occupational therapy recipients and nonrecipients among younger patients, but this relationship dissolved among older patients. Increasing age has been well established as a significant predictor of postcritical care institutional discharge (Gehlbach et al., 2011), and older adults are also more likely to receive rehabilitation services such as occupational therapy (Freburger et al., 2018). Older age is associated with several factors that limit the functional independence required for community discharge (Jette et al., 2014; Romero-Ortuno et al., 2016; Saab et al., 2019). Thus, reduced health and functional capacities associated with increasing age might contribute to a patient’s overall need for occupational therapy but also reduce the overall likelihood for home discharge, even when occupational therapy services are provided.
Patients with greater comorbidity burden were less likely to be discharged to the community, a finding that aligns with other research suggesting that increased comorbidity burden is associated with functional deficits or disabilities (Kabboord et al., 2016), which could make community discharge unsafe. Accordingly, we expected that the results of the current study would show that the relationship between occupational therapy utilization and community discharge differed depending on comorbidity burden. The results of the interaction term analysis did not support this hypothesis. However, as with the influence of age-related factors on discharge disposition, health and functional deficits linked to higher comorbidity burden may necessitate continued post-NCCU institutional care even when patients receive occupational therapy in the NCCU. Additional research is needed to examine the impact of comorbidity burden and occupational therapy services on short-term outcomes such as community discharge, in the context of improving longer term outcomes such as community independence and avoiding hospital readmission.
Occupational therapists commonly assess and base discharge recommendations on age- and comorbidity-related health and functional deficits. In this way, patients seen by an occupational therapist benefit from the therapist’s recommendations for the safest discharge location to ensure the greatest balance between independence and support (Rogers et al., 2017). For older patients with higher comorbidity burden, discharge to an institution is often seen as a more sensible outcome when discharge to home would be unsafe and could lead to readmission (Pritchard et al., 2019). The current study lacked information on therapists’ discharge recommendations; accordingly, we recommend that future research examine the relationship among patient characteristics, occupational therapy discharge recommendations, and discharge disposition. Such work could examine the extent to which postacute care is a sensible short-term outcome to ensure better long-term outcomes for some NCCU patients.
We were surprised to find an interaction between gender and receipt of occupational therapy. The relationship between occupational therapy services and community discharge was more substantial among men compared with women. The literature on the independent effects of sex on discharge setting and therapy utilization is mixed and often varies by diagnosis (Kumar et al., 2019; Mitchell et al., 2016). Thus, a lack of consensus exists on the actual effects of sex on discharge disposition and therapy utilization, and unmeasured variables may explain why sex influences therapy outcomes and utilization.
Several important variables are likely related to discharge disposition and occupational therapy services that were not available to us in this study, for example, data on patients’ functional status, previous living situation, and administrative processes. In-hospital functional status is positively associated with community discharge (Stein et al., 2015). Rehabilitation patients who lived at home preadmission are more likely to return home (Stineman et al., 2014). In acute and postacute settings, patients with an available caregiver are more likely to be discharged home (Rodakowski et al., 2017). Receipt of occupational therapy services may be influenced by referral processes, workflows, or other protocols used in the NCCU. For example, certain diagnosis-specific order sets (e.g., with subarachnoid hemorrhage) trigger an occupational therapy consult, which may not be the case for patients admitted after glioma resection. Patient-level data for order sets or other means of generating an occupational therapy referral were not available to us. Future research should investigate the influence of functional status, caregiver support and previous living situation, and administrative processes.
Implications for Occupational Therapy Practice
Occupational therapists in the NCCU play a critical role in preparing patients for discharge to the safest possible location. This study has the following implications for occupational therapy practice: Receipt of occupational therapy in the NCCU may be associated with a higher likelihood of noncommunity discharge (i.e., to inpatient rehabilitation, skilled nursing, or long-term care). Activity limitations and comorbidity burden may be greater for recipients of occupational therapy, and NCCU patients are presumably less prepared for community discharge. Future research must examine additional variables that likely influence discharge planning for NCCU patients, such as functional status and living situation.
Conclusion
This study helps to explain the extent to which patient factors and NCCU occupational therapy utilization relate to discharge disposition. Our findings suggest that the receipt of occupational therapy is associated with reduced odds of community discharge. This finding may be because occupational therapy recipients have greater functional limitations and comorbidity burden than nonrecipients. Prospective research is needed to tease out the influence of practitioner decision making regarding occupational therapy utilization in the NCCU. As we consider the study findings within the context of the NCCU standards, we suggest that future research must refine these standards with respect to occupational therapy utilization and outcomes.
Footnotes
Acknowledgment
This work was supported by a Health Services Research Grant (AOTFHSR19MALCOLM) from the American Occupational Therapy Foundation.