
Abstract
This article provides the first synthesis of the existing literature on the relationship between ACLS scores and functional and adaptive functional performance of people living with mental illness.
Living with mental illness affects a person’s everyday life. Mental illness has been reported to have the second largest burden of nonfatal disease (Australian Institute of Health & Welfare, 2016), and this burden is mostly due to an associated reduction in functional ability (Rajji et al., 2014). People with mental illness, particularly less prevalent illnesses such as schizophrenia and bipolar disorders, are likely to have difficulties with functioning across numerous occupations (Morgan et al., 2012), including, for example, community living (Rocca et al., 2018; Strassnig et al., 2018); gaining and maintaining employment (Hakulinen et al., 2019); social competence (Halverson et al., 2020); managing money and finances (Labrum, 2018); and various activities of daily living (ADLs), such as personal hygiene, dressing, and maintaining regular nutrition (Velligan et al., 2000).
Functional Performance and Adaptive Functional Performance
The functional ability of people living with a mental illness is complicated or challenged by changes in the environment in which they live, fluctuations in their mental state, and changes in the resources available. Such challenges contribute to the demand for ongoing adaptation or adjustment to what they do as part of their functional performance (Bowie et al., 2006; Velligan et al., 2007).
Although adaptive functioning is a term frequently used in literature, there is no consensus on its meaning. Definitions range from a focus on personal control (Thompson, 2002) to the ability to perform daily activities in accordance with desired roles (Oakley et al., 1985; Stein et al., 1995). A common thread throughout various definitions is not only the expectation of behavioral competence (functional performance) but also the ability to adjust performance to changing circumstances (adaptive functional performance). In this scoping review, we define functional performance as competence in completing usual or habitual everyday tasks, in a single time frame, and in a stable or familiar context. Adaptive functional performance is defined as the ability to successfully adapt or modify one’s usual functional performance to manage fluctuations in personal capacity, well-being, and available resources that occur over time or in a changing setting.
For example, making a hot cup of tea, with familiar equipment, one weekend morning at home would be considered functional performance. In contrast, making a hot cup of tea daily for a year, during which time multiple factors relating to person (such as illness) and environment (different kitchen, equipment, time, and people) may arise, requiring modification in the way the task is done, would be considered adaptive functional performance.
Cognitive Deficits
People with mental illness commonly experience cognitive deficits. Research has demonstrated the links between cognitive deficits and functional capacity (Bowie & Harvey, 2006; Bowie et al., 2006; Green & Harvey, 2014; Rajji et al., 2014; Velligan et al., 2000). However, although there is evidence that cognitive impairment affects a person’s ability to function, it is not clear whether it affects functional performance and adaptive functional performance in the same way. This may, in part, be due to an inconsistent distinction made between functional performance and adaptive functional performance.
Allen Cognitive Level Screen
The Allen Cognitive Level Screen (ACLS; Allen et al., 2007) is used by occupational therapists working in mental health as a quick screening measure of cognition and is based on the cognitive disability model (Katz, 1992). The ACLS purports to assess functional cognition, or the interaction between a person’s global cognitive processing capacity and specific task demands (Allen et al., 2007). An ACLS score is obtained by observing a person performing a graded task of leather lacing and comparing their performance against standardized scoring criteria. The task involves attending to sensory cues, verbal and demonstrated instructions and cues, and feedback from motor actions. The score is then validated by observing the person’s functional performance on other tasks (Allen et al., 2007). The scores obtained are based on the hypothesis that a hierarchical continuum of observable patterns in both functional performance and adaptive functional performance exists and that a person’s global cognitive processing capacity produces similarly ordered errors in functional performance (Allen et al., 2007). The ACL hierarchy ranges from 0 (coma) to 6 (normal cognition), and ACLS scores range from a low of 3 (the person requires a high level of supervision to ensure safety during performance of tasks) to a high of 6 (no cognitive assistance is required).
In accordance with the predictive hierarchy proposed in the cognitive disability model, each ACLS score level has an associated set of recommended supports and safety precautions needed to enable a person’s “best ability to function” (Allen et al., 1998, p. 3). Although the ACLS is a performance-based measure of cognition, the extent to which ACLS scores predict both the functional performance and the adaptive functional performance of people living with a mental illness is not clear.
Occupational therapy practitioners strive to facilitate optimum function. Cognition is assessed to support this aim, and the ACLS is one tool, widely used by occupational therapists internationally, to do so. Although research on the use of the ACLS in mental health practice has been published over the past 40 yr, no comprehensive review of this body of work has been conducted, nor have gaps in the existing literature been established. An initial scan of the literature revealed no randomized controlled trials and the use of a diverse range of study designs and functional performance measures, making quantitative synthesis impossible. Therefore, we carried out a scoping review with the aim of collating, summarizing, and reporting on the existing literature on the relationship between ACLS scores and the functional and adaptive functional performance of adults living with a mental illness.
Method
The five-stage scoping review methodology proposed by Arksey and O’Malley (2005) was adopted for this project. This method provides a framework to review the breadth of available literature on a subject in a rigorous and transparent way (Arksey & O’Malley, 2005). The five stages are as follows: (1) identify the research question; (2) identify relevant studies; (3) select studies; (4) chart the data; and (5) collate, summarize, and report the results.
Research Question
For this scoping review, the research question was, “What is known from published, English-language, peer-reviewed literature about the relationship between ACLS scores and functioning for adults living with a mental illness?”
Identification of Relevant Studies
Broad search terms were used to ensure the breadth of available literature on ACLS and mental health was encompassed. Searches were conducted of the CINAHL, MEDLINE, PsycINFO, and OTseeker electronic databases with the following search terms: Allen cognitive.mp. Psychiat*.mp Mental health.m.p Schizophren*.m.p 2 or 3 or 4 1 and 5
The ProQuest database was also searched using the search terms [“allen cognitive” AND (psychiat* or “mental health” or “schizophren*)]. No date limits were included in the search to ensure inclusion of all relevant literature. A total of 210 records were identified.
Study Selection
Figure 1 provides details of the study selection process. Duplicates were removed by Kylie Stewart, resulting in 162 studies. Titles and abstracts were then screened independently by Stewart and Nicola Hancock. For inclusion in the study, the following criteria were required: publications were peer reviewed, in English, and reported on the assessment of any relationship between the ACLS and functional performance, adaptive functional performance, or both, and participants were adults (ages 18–65 yr), with the majority of the study sample having a mental health diagnosis. When any disagreements arose between Stewart and Hancock, the articles were retained. This screening resulted in the exclusion of 120 publications. Forty-two full-text articles were reviewed independently by these two reviewers against the criteria listed previously, and disagreements were resolved by consensus. Fifteen studies were included in the final analysis.
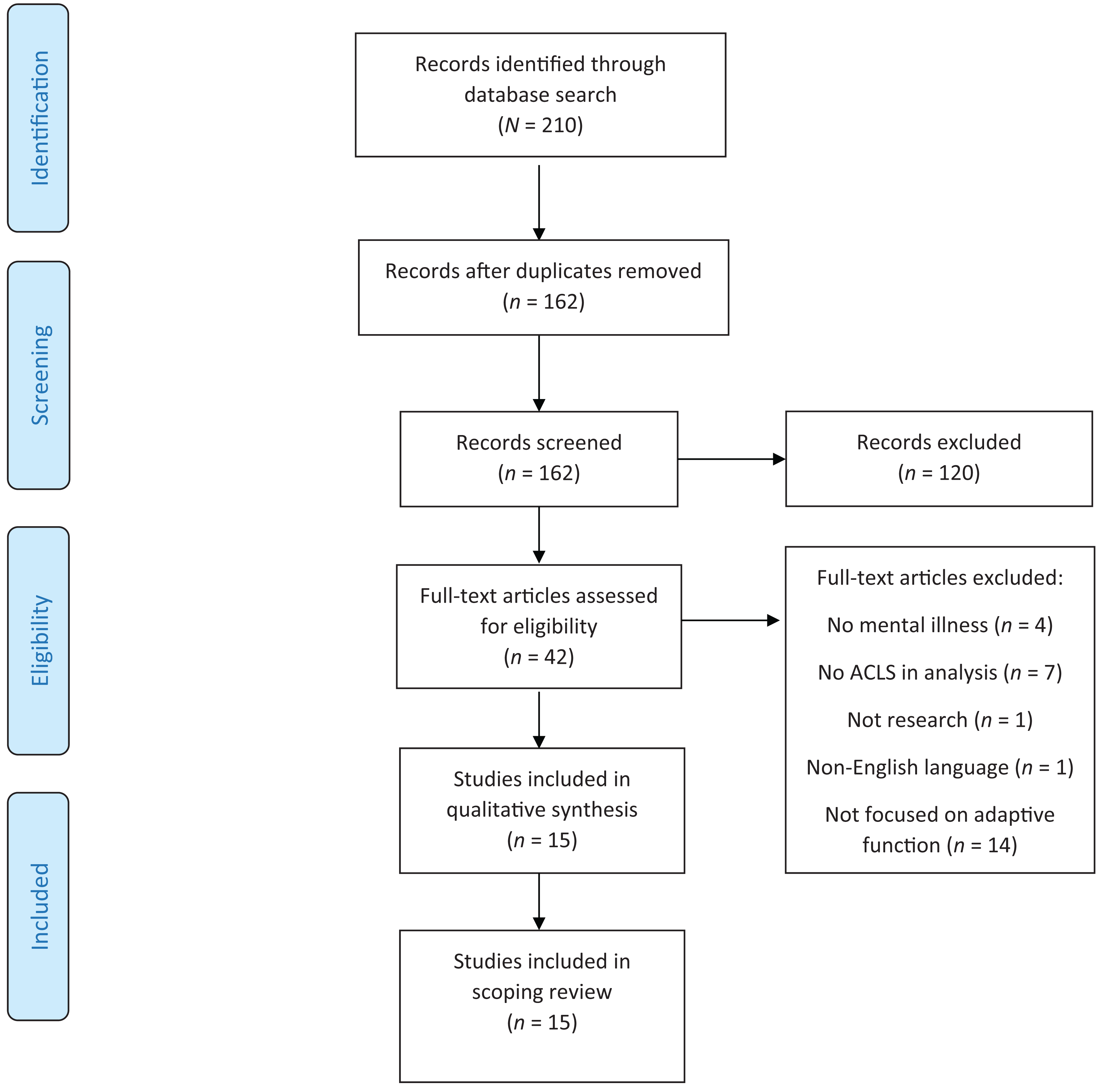
PRISMA flow diagram for study selection.
Data Charting
From each of the 15 included studies, the following data were extracted: author, title, year and country of study, setting of study, participant diagnosis, number of participants, assessments or measures used, timing between assessments, statistical analysis conducted, and aspects of functional performance and adaptive functional performance examined. When a usual or known single task was assessed at a single time point, in a familiar or stable context, it was deemed to be an assessment of functional performance. When more complex tasks or activities were assessed, or familiar tasks were assessed over time or in unfamiliar or multiple contexts, it was deemed to be an assessment of adaptive functional performance.
Tasks and activities were assessed and charted as ADLs if they were considered daily self-care activities; as social skills if they were centrally about a person’s ability to communicate and interact with others; as roles if they involved a set of behaviors and actions associated with expectations in social and performance contexts; and as community living if they pertained to a person’s overall capacity to manage living in the community.
Collating, Summarizing, and Reporting
Numerical and thematic summaries of the data were completed to map the type and location of participants, range of measures used, and direction of relationships between ACLS scores and functional or adaptive functional performance. Study authors were contacted when clarification of data was required. To enable comparison and identify gaps in research, studies were thematically organized and grouped.
Results
Table A.1 in the Appendix provides a summary of all articles included in this review. The largest number of studies were conducted in the United States (n = 6; Davidhizar et al., 1991; Helfrich et al., 2011; Henry et al., 1998; Penny et al., 1995; Schubmehl et al., 2018; Velligan et al., 1998), followed by Australia (n = 4; Cairns et al., 2013; Keller & Hayes, 1998; Scanlan & Still, 2013; Stewart et al., 2019) and Hong Kong (n = 2; Leung & Man, 2007; Yeung & Chan, 2006), with single studies conducted in Canada (McAnanama et al., 1999), China (Chan & Yeung, 2008), and Israel (Raweh & Katz, 1999). Dates of publication ranged from 1991 to 2019. A total of 1,583 participants were included across all 15 studies, and sample size ranged from 11 to 225 participants. More than half (n = 9) of the publications reported all participants’ diagnosis as schizophrenia or psychotic illness (Chan & Yeung, 2008; Keller & Hayes, 1998; Leung & Man, 2007; McAnanama et al., 1999; Raweh & Katz, 1999; Schubmehl et al., 2018; Stewart et al., 2019; Velligan et al., 1998; Yeung & Chan, 2006), with the remainder including a range of mental health diagnoses. The majority (63%) of participants (n = 9 studies; Davidhizar et al., 1991; Henry et al., 1998; Keller & Hayes, 1998; McAnanama et al., 1999; Penny et al., 1995; Scanlan & Still, 2013; Schubmehl et al., 2018; Stewart et al., 2019; Velligan et al., 1998) were in inpatient mental health units at the time of the study.
The majority of studies (n = 8; Chan & Yeung, 2008; Helfrich et al., 2011; Henry et al., 1998; Leung & Man, 2007; Raweh & Katz, 1999; Scanlan & Still, 2013; Schubmehl et al., 2018; Yeung & Chan, 2006) did not report on the time frame between administration of the ACLS and functional assessments. A single functional performance study (Penny et al., 1995) reported on the time frame between assessments (same day); of the 13 studies focused on adaptive functional performance, 7 reported a time frame (Cairns et al., 2013; Davidhizar et al., 1991; Keller & Hayes, 1998; McAnanama et al., 1999; Penny et al., 1995; Stewart et al., 2019; Velligan et al., 1998). When reported, the time elapsed between ACLS administration and assessment of adaptive functional performance ranged from the same day (Cairns et al., 2013; Davidhizar et al, 1991; Penny et al., 1995) to 3.5 yr later (Velligan et al., 1998).
Table A.2 reports the aspects of functioning assessed and the significance of their relationships with ACLS scores for both functional and adaptive functional performance. Table A.3 summarizes the type of performance (functional or adaptive functional, whether adaptive functional performance data were retrospective or prospective), its relationship with ACLS scores, and the data collection method.
Functional Performance
The relationship between ACLS scores and level of functional performance (i.e., a discrete activity assessed at a single point in time) was reported in 6 studies (Helfrich et al., 2011; Leung & Man, 2007; Penny et al., 1995; Scanlan & Still, 2013; Schubmehl et al., 2018; Velligan et al., 1998; see Table A.3). The content of these data was analyzed from three perspectives. First, broadly across these 6 studies, a significant positive relationship between ACLS scores and functioning was reported for 89% of tasks; that is, higher cognition scores were related to better functional performance. Some 11% of tasks showed no relationship to ACLS scores. (Note that percentages were calculated by the ratio of identified elements compared with the total number of elements assessed in all studies.)
Second, type and number of tasks and the direction of their relationship to ACLS scores were analyzed (see Table A.2). ADLs were reported in the majority of the 6 studies that assessed functional performance (Helfrich et al., 2011; Leung & Man, 2007; Scanlan & Still, 2013; Schubmehl et al., 2018; Velligan et al., 1998), followed by social skills (Leung & Man, 2007; Penny et al., 1995), and then roles (Penny et al., 1995). A positive relationship with ACLS scores was reported for all but one type of ADL (safe community living). For self-care, a mix of positive and no relationship was reported.
Third, methods used to collect data to measure functional performance were identified and included observation (Leung & Man, 2007; Penny et al., 1995), self-report (Helfrich et al., 2011), or a mixture of both (Scanlan & Still, 2013; Schubmehl et al., 2018; Velligan et al., 1998) at a single point in time (see Table A.3). Both self-report of tasks (80%) and direct observation of tasks (91%) were consistently related to ACLS scores. The majority of functional performance measures were performed with people on inpatient units (Penny et al., 1995; Scanlan & Still, 2013; Schubmehl et al., 2018; Velligan et al., 1998), and 2 studies assessed people in the community (Helfrich et al., 2011; Leung & Man, 2007; see Table A.1).
Adaptive Functional Performance
The findings for the 13 studies that reported on adaptive functional performance are summarized from four perspectives. First, global analysis indicated that results yielded by these studies were not uniform, with 6 (Cairns et al., 2013; Chan & Yeung, 2008; Keller & Hayes, 1998; Penny et al., 1995; Scanlan & Still, 2013; Yeung & Chan, 2006) reporting only significant positive relationships, 2 (McAnanama et al., 1999; Raweh & Katz, 1999) having no significant relationship, and 5 (Davidhizar et al., 1991; Henry et al, 1998; Schubmehl et al., 2018; Stewart et al., 2019; Velligan et al., 1998) having a mix of positive and no relationship (see Table A.2).
Second, types of activities and their relationship to ACLS scores were analyzed. Living situation before admission to the hospital, number of days spent in the community before readmission to the hospital (in the 12 mo postdischarge), medication adherence, money management, phone use, laundry skills, room care, travel, and parent or caregiving roles all demonstrated consistent positive relationships to ACLS scores (see Table A.2). Living situation on discharge from the hospital, self-care, independence in ADLs, instrumental or global function, social competence, productive role, and the homemaker role all had a mix of positive or no relationship to ACLS scores. The assessments of community living—number of returns to the hospital, days spent in the hospital over a period of time after discharge, amount of assistance required in a person’s living environment, and the Routine Task Inventory assessment of ADLs—all showed no relationship to ACLS scores. A positive significant relationship was reported for 64% of adaptive functional performance activities, whereas no significant relationship was found for 36% of such activities. There were no instances of negative relationships. The majority of adaptive functional performance measures were performed with people in the community (n = 8; Cairns et al., 2013; Chan & Yeung, 2008; Keller & Hayes, 1998; McAnanama et al., 1999; Raweh & Katz, 1999; Stewart et al., 2019; Velligan et al., 1998; Yeung & Chan, 2006); 7 studies reported on the assessment of people over time in an inpatient setting (Davidhizar et al., 1991; Henry et al., 1998; Keller & Hayes, 1998; McAnanama et al., 1999; Penny et al., 1995; Stewart et al., 2019; Velligan et al., 1998; see Table A.1).
Third, frequency of the type of activities reported in the 13 studies was collated. Community living activities were reported most frequently (n = 7; Chan & Yeung, 2008; Davidhizar et al., 1991; Henry et al., 1998; Schubmehl et al., 2018; Stewart et al., 2019; Velligan et al., 1998; Yeung & Chan, 2006), followed by ADLs (n = 6; Cairns et al., 2013; Davidhizar et al., 1991; Keller & Hayes, 1998; McAnanama et al., 1999; Scanlan & Still, 2013; Velligan et al., 1998), roles (n = 4; Henry et al., 1998; Penny et al., 1995; Scanlan & Still, 2013; Velligan et al., 1998), and then social skills (n = 3; Davidhizar et al., 1991; Keller & Hayes, 1998; Velligan et al., 1998; see Table A.2). The ACLS had the strongest relationship with roles (71%), followed by ADLs (69%), social skills (67%), and community living (54%).
Finally, the data were categorized according to the way information about adaptive function was obtained (see Table A.3). Most studies focused solely on retrospective adaptive functional performance (n = 7; Cairns et al., 2013; Chan & Yeung, 2008; Davidhizar et al., 1991; Keller & Hayes, 1998; McAnanama et al., 1999; Raweh & Katz, 1999; Yeung & Chan, 2006); 3 focused on a mix of performance that included retrospective adaptive functional performance (Penny et al., 1995; Scanlan & Still, 2013; Schubmehl et al., 2018); 1 focused solely on prospective adaptive functional performance (Stewart et al., 2019); and 2 focused on a mix of performance that included prospective functional performance (Schubmehl et al., 2018; Velligan et al., 1998). As shown in Table A.3, adaptive functional performance was assessed by observation (n = 8; Chan & Yeung, 2008; Davidhizar et al., 1991; Henry et al., 1998; Keller & Hayes, 1998; Penny et al., 1995; Raweh & Katz, 1999; Stewart et al., 2019; Yeung & Chan, 2006) and by self-report or both observation and self-report (n = 5; Cairns et al., 2013; McAnanama et al., 1999; Scanlan & Still, 2013; Schubmehl et al., 2018; Velligan et al., 1998) over time. Observation of adaptive functional performance (72%) yielded more consistent relationships to ACLS scores than self-report (29%). Assessment of adaptive functional performance that occurred before administration of the ACLS, that is, retrospective functioning, was used in the majority of studies (n = 11; Cairns et al., 2013; Chan & Yeung, 2008; Davidhizar et al., 1991; Henry et al., 1998; Keller & Hayes, 1998; McAnanama et al., 1999; Penny et al., 1995; Raweh & Katz, 1999; Scanlan & Still, 2013; Schubmehl et al., 2018; Yeung & Chan, 2006). Prospective assessment of adaptive functional performance after the ACLS was administered was used less frequently (n = 4; Henry et al., 1998; Schubmehl et al., 2018; Stewart et al., 2019; Velligan et al., 1998).
Discussion
This scoping review examined the peer-reviewed literature on the relationship between ACLS scores and functional ability of adults with a mental illness. For the purpose of this study, functional performance was defined as competence in completing a usual, everyday task at a single point in time in a nonchanging context. In contrast, we defined adaptive functional performance as the ability to successfully adapt or modify functional performance to navigate and manage fluctuations in personal capacity, well-being, and available resources that occur over time or in changing settings. Although a positive relationship between ACLS scores and functional performance was consistently reported across the literature (89% of tasks), the relationship between adaptive functional performance and ACLS scores was less consistent (64% of activities).
Functional Performance
The literature evidences a consistent relationship between in-the-moment functional performance of a usual task in stable conditions and ACLS scores, suggesting that ACLS scores are a good measure of people’s current functional performance. The consistency of this relationship remained high irrespective of whether functional performance was measured using self-report (80% of tasks assessed had a significant relationship to ACLS scores) or direct observation (91% had a significant relationship to ACLS scores). Equally, this relationship remained consistent irrespective of the task the study authors chose to assess. These findings collectively suggest that the ACLS is a promising tool for occupational therapists to use in determining the ability of a person living with mental illness to perform uncomplicated, usual, daily tasks at one point in time. However, there are limitations to this body of literature: only 6 studies (40% of included studies) examined functional performance. Most of these 6 studies (n = 4) assessed people in an inpatient setting that could be assumed to be highly controlled and not a natural environment, rather than in the community context (n = 2). Most had relatively small sample sizes. Therefore, the findings need to be viewed with these limitations in mind.
Adaptive Functional Performance
The reported relationship between adaptive functional performance of activities and ACLS scores was much less consistent across the studies reviewed. The timing of assessments, the complexity of activities selected to assess adaptive functional performance, and how adaptive functional performance was measured all affected the relationship between adaptive functional performance and cognition as measured by the ACLS.
Timing of Assessments
It is important to note that the majority of studies did not report the exact length of time between when ACLS scores were obtained and when adaptive functional performance was measured. A relationship between adaptive functional performance and ACLS scores was more likely (69%) when adaptive functional performance was measured retrospectively. When measured prospectively, adaptive functional performance was related to cognitive measures in only 50% of studies. The small amount of research using prospective assessment of adaptive functional performance (n = 4; Henry et al., 1998; Schubmehl et al., 2018; Stewart et al., 2019; Velligan et al., 1998), along with the mixed findings from these studies, suggest that it cannot be asserted with confidence that ACLS scores are a good predictor of how a person will function in the future. It is interesting to note that occupational therapists in Australia and internationally use ACLS scores and corresponding ACLS recommendations to predict a patient’s prospective functional performance, that is, postdischarge plans and community living prospects. Studies in which community living was measured prospectively, after administration of the ACLS, had the least consistent positive association (33% of activities). These results indicate that there is little evidence on whether ACLS scores can indeed predict patients’ prospective performance, suggesting that use of the ACLS for future planning should proceed with caution until further evidence of its predictive validity is ascertained. Future research that clearly articulates the time frame between administration of the ACLS and performance of function and an increase in the number of studies focusing on prospective adaptive functional performance are needed.
Context and Complexity of Activities Assessed
One finding of this review was that the complexity of activity assessed affected the relationship with ACLS scores. When a specific cluster of activities of adaptive functional performance activities was assessed, such as ADLs, a more consistent relationship with ACLS scores was found (73% of activities). As measures of adaptive functional performance became more multifaceted or broad (e.g., community living), the results were less consistent (only 56% of activities had a relationship with ACLS scores). There may be several reasons for this. First, contexts will fluctuate over time. When a greater breadth of activities is assessed, greater contextual fluctuations can be expected and therefore a greater requirement exists for the person to be able to adapt. Second, none of the included studies considered or reported on contextual factors or on whether factors changed over time. Without these data, it is difficult to gain a meaningful assessment of how well people can adapt their performance to navigate and manage contextual or environmental fluctuations. Although the ACLS has a list of recommended supports, the supports and barriers that occur and how these fluctuate need to be examined to gain a useful assessment of a person’s ability to function in their natural environment over time.
Method of Assessing Adaptive Functional Performance
Another finding of this review indicated that the method of assessing adaptive functional performance affected the relationship with ACLS scores. Unlike functional performance, for which we observed consistent relationships with ACLS scores irrespective of method of assessment, when we looked at adaptive functional performance, self-report appears less consistently related to cognition scores (29% of activities) than observation (71%). Again, it is possible that a lack of consideration of environmental nuances such as supports from family or others limits the utility or blunts the accuracy of assessments of adaptive functional performance. Self-report, or even clinical observation if not constant and direct, might result in a score reflecting higher- or lower-than-actual adaptive functional performance if environmental supports are facilitating or hindering a person to achieve that level of performance. Although these results suggest caution in using self-report measures with people with a mental illness to report on adaptive functional performance over time, they also highlight the need for more in-depth investigation into how and what supports enable people to navigate changes over time to successfully function in the community. Cognition alone might not be a good single measure of adaptive functional performance.
Moreover, the lack of consistently used measures across this body of literature suggests that consensus in occupational therapy practice and research is limited regarding the definition of and best way to measure functional performance and adaptive functional performance. In the process of compiling this review, we devised definitions of functional performance and adaptive functional performance that we hope will progress this focus in research and practice, enabling clearer and more transparent distinctions to be made.
Limitations
Although a scoping review was deemed most appropriate because of the diverse measures of functional performance and methods used, this approach also affected the analyses we could use. The use of statistical significance in this review rather than effect size means that our findings may be influenced by sample size, because significance is easier to achieve in larger samples. Because analysis involves a simple unweighted count of findings, the reported results may overemphasize studies with multiple findings or studies with small sample sizes. Studies that examined performance over time implicitly assumed that ACLS scores are stable over time. The data to date on the temporal stability of ACLS scores are limited.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practitioners working with adults who have a mental health diagnosis: Practitioners can be confident that ACLS scores give a good indication of a person’s in-the-moment functional performance. Practitioners should be cautious about inferring a person’s future adaptive functional performance ability from ACLS scores.
Future research is needed to establish sound and consistent assessment of adaptive functional performance that incorporates an understanding of the natural environment.
Conclusion
To aid in this scoping review, we identified a clear distinction between functional performance and adaptive functional performance to examine literature reporting on their relationship to ACLS scores. In our scoping review of 15 studies, we found a consistent relationship between in-the-moment functional performance of a discrete task and ACLS scores; the timing of assessments, the complexity of activities selected to assess adaptive functional performance, and how adaptive functional performance was measured all affected the relationship between adaptive functional performance and cognition as measured by the ACLS. Gaps in this literature included the limited consensus on and research regarding the definitions of and best way to measure functional and adaptive functional performance; inconsistent and unreported time frames between when ACLS scores were obtained and when adaptive functional performance was measured; and a lack of reporting of contextual factors that might change over time, thus affecting performance. Further research addressing these gaps is needed to provide guidance on the usefulness of the ACLS in assessing functional and adaptive functional performance of adults living with a mental illness.
Footnotes
*
Indicates articles included in the scoping review.
Acknowledgments
Kylie Stewart took a leadership role in the design, data collection, analysis, and writing of this scoping review. All authors contributed to the study design, data analysis and interpretation, and the writing of this review. The authors declare no financial support has been received in conjunction with the generation of this submission, and they declare no conflict of interest with respect to the authorship or publication of this review.
Appendix. Supplemental Tables
Type of Performance, Relationship With ACLS Scores, and Measure of Performance
| Study | Type of Performance and Relationship With ACLS Score | Measure of Performance | ||||||
|---|---|---|---|---|---|---|---|---|
| FP | AFP | AFP and Retrospective Functioning | AFP and Prospective Functioning | Significant Relationship Between Function and ACLS (p < .05) | Single Observation | Observation Over Time | Self-Report | |
| Cairns et al. (2013) | X | X | A | X | ||||
| Chan & Yeung (2008) | X | X | A | X | ||||
| Davidhizar et al. (1991) | X | X | S | X | ||||
| Helfrich et al. (2011) | X | S | X | |||||
| Henry et al. (1998) | X | X | X | S | X | |||
| Keller & Hayes (1998) | X | X | A | X | ||||
| Leung & Man (2007) | X | A | X | |||||
| McAnanama et al. (1999) | X | X | N | X | ||||
| Penny et al. (1995) | X | X | X | A | X | X | ||
| Raweh & Katz (1999) | X | X | N | X | ||||
| Scanlan & Still (2013) | X | X | X | A | X | X | X | |
| Schubmehl et al. (2018) | X | X | X | X | A | X | X | X |
| Stewart et al. (2019) | X | X | S | X | ||||
| Velligan et al. (1998) | X | X | X | S | X | X | X | |
| Yeung & Chan (2006) | X | X | A | X | ||||
| Total | 6 | 13 | 11 | 4 | A = 7; S = 6; N = 2 | 5 | 11 | 6 |
Note. A = all assessed factors; ACLS = Allen Cognitive Level Screen; AFP = adaptive functional performance; FP = functional performance; N = none of the assessed factors; S = some of the assessed factors.
Citation: Stewart, K., Hancock, N., Chapparo, C., & Stancliffe, R. J. (2022). Functional performance and the Allen Cognitive Level Screen for adults with mental illness: A scoping review (Table A.3). American Journal of Occupational Therapy, 76, 7602205150. https://doi.org/10.5014/ajot.2022.045757