
Abstract
The findings of this study support the use of goniometry to measure scapular protraction and retraction in relation to occupational performance.
The scapula, as a component of functional motion of the upper extremity, is essential for meaningful occupation. The scapula provides foundational support for purposeful motions of the shoulder (Oatis, 2009). Scapulohumeral rhythm is the coordination of synchronous motions in the upper extremity; it is necessary for overhead flexion or abduction of the humerus, specifically requiring upward rotation of the scapula (Coppard & Lohman, 2015; Paine & Voight, 2013). Reaching in front of or behind the body requires scapular protraction or retraction (Coppard & Lohman, 2015; Paine & Voight, 2013). Scapular protraction involves the abduction and internal rotation of the scapula around a vertical axis. It assists in the movements necessary to complete daily functional tasks that involve reaching out in front of the body, for example, getting an item off a high shelf, combing one’s hair, applying deodorant, and reaching to put dishes away in a kitchen cabinet (Gates et al., 2016 ; Rundquist et al., 2011; Short et al., 2021). Scapular retraction involves adduction and external rotation of the scapula around a vertical axis and is necessary for activities of daily living such as toileting hygiene (Gates et al., 2016 ; Short et al., 2021).
Scapular retraction is also an important part of the kinetic chain for high-velocity motions required for athletics, such as pitching in baseball or performing the backstroke while swimming (Paine & Voight, 2013; Short et al., 2021). Using established goniometric assessment techniques, many motions of the glenohumeral joint (GHJ; e.g., flexion, abduction, rotation) demonstrate functional range of motion (ROM) values for clinical use. Without an established goniometric technique to quantify scapular protraction and retraction, these functional values for such an important component of the kinetic chain of the upper extremity remain elusive.
ROM measurements are used as an objective metric to demonstrate functional gains and to justify reimbursement during the rehabilitation process. Many pathologies may impair scapular mobility and shoulder motion—hemiparesis or scapular winging related to a stroke, rotator cuff repair, and subacromial impingement, to name a few (Paine & Voight, 2013). Although clinically accepted goniometric methods are reported in the literature for most movements of the upper extremity, there is currently no described method for measurement of scapular protraction and retraction. Short et al. (2021) proposed a goniometric technique using the relative position of the superior angle of the scapula and the acromion as anatomical landmarks to measure protraction and retraction (Figure 1A); however, the proposed method has not been empirically tested for reliability. There is thus a need to establish the interrater reliability of this novel goniometric technique for the measurement of scapular protraction and retraction.
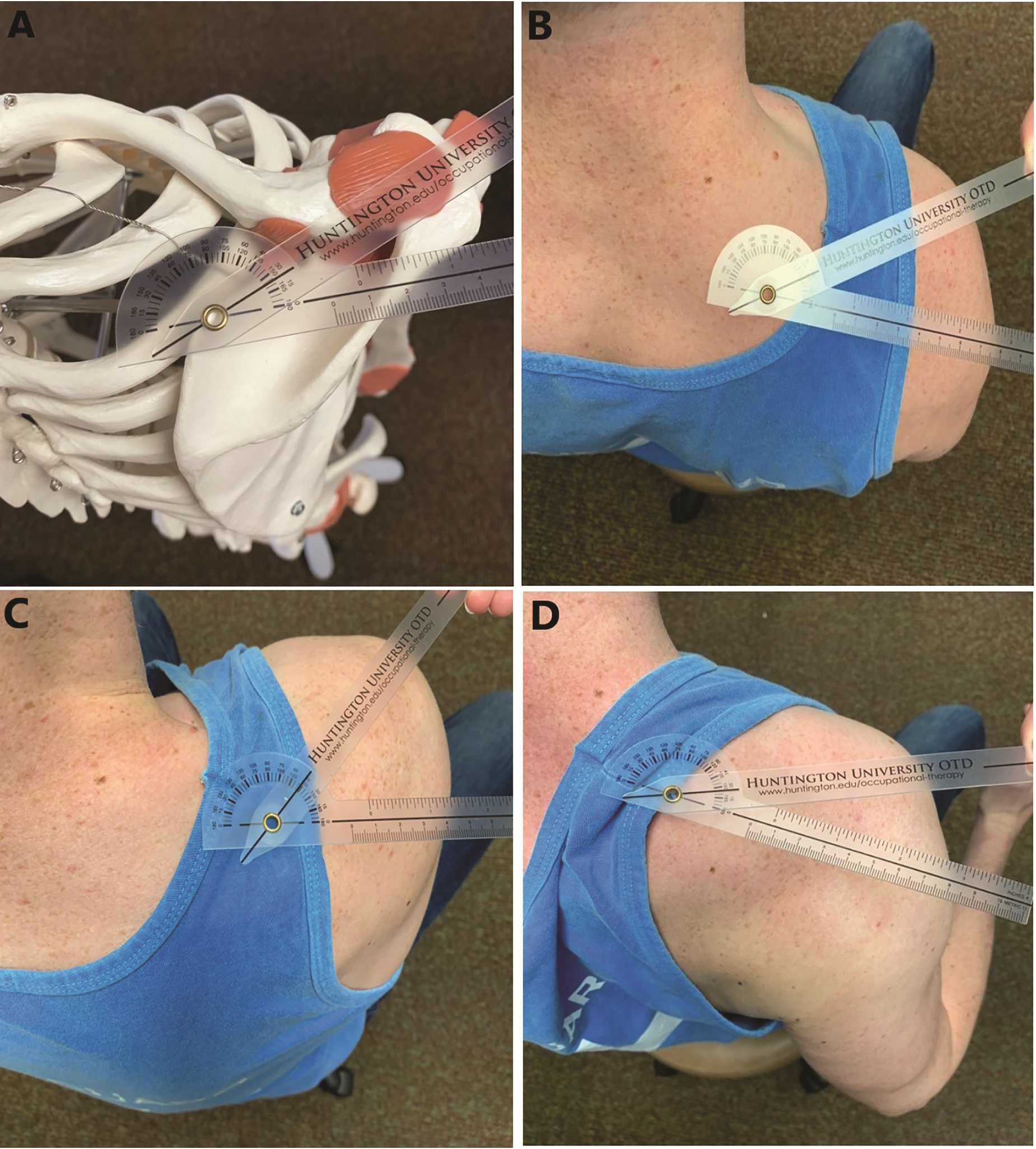
Goniometry for scapular protraction and retraction: (A) anatomical alignment of goniometer, (B) scapula at rest, (C) protracted scapula, and (D) retracted scapula.
Scapular Range of Motion
Macedo and Magee (2008) researched ROM differences between dominant and nondominant joints in both the upper and the lower extremities. Goniometry measurements were collected from the ankle, knee, hip, shoulder, elbow, and wrist joints of 90 healthy women. None of the differences in measurement between dominant and nondominant joints were significant enough to affect the estimation of ROM when using a goniometer. When analyzing the ROM of the joint angles of the upper and lower extremities, a standard error of measurement (SEM) of less than 5° for goniometric measurement was suggested as accurate, consistent, and reliable.
The literature reports two methods for quantifying the movement and position of the scapula that do not use goniometry: the Lateral Scapular Slide Test (LSST) and the digital inclinometer (Depreli & Angın, 2018; Kolber et al., 2012). Depreli and Angın (2018) examined scapular motion in relation to the vertebrae. Movement was measured using the LSST, which involved placing the GHJ in three positions: (1) neutral, (2) medial rotation with 45° of shoulder abduction in the frontal plane, and (3) maximal medial rotation with 90° of shoulder abduction in the frontal plane (Depreli & Angın, 2018). Curtis and Roush (2006) explained that the LSST may be a reliable measure to determine scapular positioning, but a broad range of error exists within these measurements.
Kolber et al. (2012) researched active shoulder elevation in the scapular plane with a goniometer and digital inclinometer to determine validity and reliability. The SEM was recorded in addition to the minimal detectable change to assess the magnitude of change for a 95% confidence interval. The results of this study indicated strong inter- and intrarater reliability for measuring GHJ motion using goniometry. Because scapular motion is an essential element of functional movement of the shoulder complex, investigation of goniometric methods to measure scapular motion is also warranted.
MacDermid et al. (1999) examined the reliability of GHJ goniometry and suggested that it had high interrater reliability, with an SEM of <8°. Therefore, for purposes of this study, an SEM of <8° was used to indicate a clinically acceptable level of variance.
We completed an extensive review of the literature and could not identify reliable methods for goniometric measurement of scapular protraction and retraction. Health care and rehabilitation professionals, specifically occupational therapists, would benefit from a practical and reliable method to measure scapular protraction and retraction as an essential component of upper extremity function. Moreover, establishing a reliable measurement technique for scapular protraction and retraction provides an objective method to assess baseline motion, monitor progress through reassessment, support reimbursement, and communicate between related disciplines. The purpose of the current study is to examine the interrater reliability of goniometric measurement of scapular protraction and retraction, as described by Short et al. (2021), using the superior angle of the scapula and acromion as bony landmarks to measure scapular motion relative to the frontal plane.
We hypothesized that measurements obtained between two expert clinicians using the proposed technique would demonstrate clinically acceptable reliability, defined for this study as an SEM of <8° (MacDermid et al., 1999).
Method
Research Design
Using an observational, descriptive design, we analyzed the interrater reliability of a novel goniometric technique to measure scapular protraction and retraction.
Participants
Purposive convenience sampling was used to recruit a sample of healthy adults older than age 18 yr in partnership with a local YMCA. Recruitment fliers were posted around the facility several weeks before the study, and staff members helped to schedule participants before data collection. The researchers also recruited participants during data collection at a registration desk set up near the entrance to the facility. Participants who were older than age 18 and had no known musculoskeletal condition that would limit scapular mobility were included; those who did not meet these criteria were excluded. We aimed to recruit a minimum of 40 participants, a trend observed in the literature for similar interrater reliability studies addressing upper extremity goniometry (Armstrong et al., 1998; MacDermid et al., 1999).
Instrumentation
A basic template was created to capture demographic information (Table 1) from the study participants. For goniometric measurements, manual 12-in. (30.48-cm) plastic goniometers with 180° interface were deemed optimal and used by each evaluator (Figure 1).
Participant Demographic Characteristics (N = 80)
Note. One participant did not provide an age; thus, the number of participants totals 79.
Procedures
We obtained ethical approval from the institutional review board of Huntington University. Students who agreed to participate received debriefing on the proposed technique used in the study and signed an informed consent form before providing demographic information. Measurements took place in a quiet room with a partition separating the two evaluators. Each participant was seated in a standard chair with a seat pan height, depth, and width of 18 in. (45.72 cm). The height of the backrest was 30 in. (76.20 cm) from the floor, allowing for clearance of the inferior angle of the scapula and full scapular retraction. The chair legs were secured to the floor to provide a stable seating surface to support the trunk and lower extremities in a neutral, upright position.
The evaluators were two occupational therapists (Nathan Short and Michelle Mays), who were also certified hand therapists, and each had more than 10 yr of clinical experience. Expert clinicians were used to complete the goniometric measurements because they have higher interrater reliability than nonexpert examiners (Blonna et al., 2012). Before implementing the study, the evaluators independently practiced the technique and then practiced together to ensure consistency. Participants were instructed to maintain their lower back against the backrest to avoid trunk flexion for all measurements.
Each participant was seated approximately 2 ft (0.60 m) from and parallel to a wall that served as a reference point for the static arm of the goniometer. The static arm was aligned perpendicular to the wall, relative to the fulcrum at the superior (medial) angle of the scapula, to maintain its position in the frontal plane. To optimize alignment of the fulcrum and moving arm of the goniometer, anatomical landmarks were identified by first palpating the acromion and then along the spine of the scapula in a medial direction to its endpoint at the superior (medial) angle (Figure 1A). Although we did not do so in this study, it may be helpful for clinicians to mark the skin over these landmarks.
Once the evaluator achieved optimal alignment, participants received verbal instructions and a demonstration of each position to measure the scapula at rest, in maximal protraction, and in maximal retraction. Respective measurements were obtained by maintaining the moving arm over the acromion and documenting the angle specified on the goniometer at the end of active range for each position. We also note that the measurements indicated the scapular position relative to the frontal plane (0°) as opposed to the starting (resting) position of the scapula.
The evaluators monitored and prevented compensatory motions—for example, trunk flexion and rotation—with verbal cueing. After the first evaluator completed all three measurements, the participant was seated behind a partition in a second chair with the same dimensions, and the second evaluator performed the same measurements. The evaluators neither saw nor heard each other’s measurements.
Data Analysis
Descriptive statistics were used for sample demographics, and the SEM was used as a metric to analyze the reliability of measurements between evaluators. The SEM was calculated in each position using the intraclass correlation coefficient values and the average of the standard deviations for the two raters. Pearson product–moment correlations were used to assess the relationships between age and the resting position of the scapula and total scapular motion. The total scapular motion was calculated by finding the difference between the angles measured in the protracted and retracted positions.
The sign and magnitude of the correlation coefficients (r values) were used to assess the direction and strength of the relationships. The strength of the r values was interpreted as follows: weak, .10–.29; moderate, .30–.49; and strong, >.50 (Cohen, 1992). The statistical significance of the r values was also assessed on the basis of a 95% confidence interval (α = .05). The resting scapular position and overall scapular motion values used in the correlation analysis were those recorded by one of the evaluators for the participants’ right upper extremity. IBM SPSS Statistics (Version 26) was used for statistical analysis.
Results
The sample (N = 80) ranged in age from 19 to 84 yr, with an equitable gender balance (56% male, 44% female), and it exceeded the target sample size. Table 2 provides the mean measurements and SEMs for resting (SEM = 3.46°), protraction (SEM = 2.93°), and retraction (SEM = 2.74°) between the evaluators. We found a weak, positive relationship between age and resting scapular position (r = .285, p = .011; Table 3), indicating that older participants were in a more protracted scapular position at rest. We also found a weak, negative correlation between age and overall scapular motion (r = −.228, p = .044; see Table 3), indicating that older participants tended to have less total scapular motion.
Mean Measurements (in Degrees) and SEM for Evaluators 1 and 2
Note. SEM = standard error of measurement.
Association of Age and Scapular Mobility
Discussion
In this study, we examined the interrater reliability of a novel goniometric technique for the measurement of scapular protraction and retraction, measuring the movement of the acromion relative to the frontal plane using the superior angle as the axis of motion (Short et al., 2021). The SEM between the two evaluators was found to be <3.5° for the resting, retracted, and protracted positions. On the basis of the established standard of an SEM of <8° (MacDermid et al., 1999), for the purposes of this study the technique demonstrated clinically acceptable interrater reliability (SEM < 4°). This finding regarding interrater reliability is particularly encouraging because the general consensus in the literature suggests that intrarater variance is typically less than interrater variance; repeated measures by the same clinician may demonstrate even higher reliability (Boone et al., 1978; MacDermid et al., 1999).
The described technique and its demonstrated reliability may serve as a consistent assessment of scapular motion, similar to measurements of the other joints of the body, as a foundation to further explore scapular mobility in a functional context. Currently, the literature is limited to gross assessments of scapular position and movement relative to the spine (Depreli & Angın, 2018). The findings of this study demonstrate consistent replication of measurements of scapular ROM between two expert clinicians among healthy participants. Establishing baseline reliability may allow the technique to be used for further analysis of typical or functional scapular protraction and retraction.
The literature emphasizes the importance of scapular motion for occupational performance such as donning and doffing clothing, participating in recreational activities, completing instrumental activities of daily living tasks such as meal preparation (Gates et al., 2016) and rest and sleep (Gordon & Grimmer-Somers, 2011), and community mobility such as driving (American Occupational Therapy Association, 2020). When a client has a deficit of scapular protraction or retraction that inhibits participation in a meaningful occupation, therapists do not have a goniometric technique to measure functional movement. The technique described in this study provides an objective, reliable measure of the scapular component of these various purposeful activities. A baseline of motion may be established with the proposed technique to develop a plan of care unique to each client and the client’s specific occupational performance deficit.
Goniometric assessment helps both the clinician and the client track and document progress throughout the intervention process (Paine & Voight, 2013). Occupational therapists encounter clients with various shoulder pathologies that may present barriers to purposeful motion and occupational performance. For example, hemiparesis related to a stroke or postural compromise due to general weakness may limit scapular mobility and the functional kinesthetic chain of the upper extremity. A reliable technique to assess scapular mobility over the course of treatment may serve as an indicator of the efficacy of treatment and progress toward occupational goals. The proposed technique may also increase motivation, allowing clients to understand their therapeutic progress with a quantitative value. This novel method offers occupational therapists a method to quantify a client’s scapular protraction or retraction as a measure of functional motion.
With additional critical analysis of the reliability and validity of this technique, normative values for the resting position of the scapula and for protraction and retraction may be established using a larger sample. Anatomically, the scapula is positioned, or protracted, approximately 30°–45° anterior to the frontal plane (Ludewig et al., 2009). However, this study’s preliminary findings suggest a correlation with age and increased protraction at rest with a decline in overall scapular mobility. Although this secondary finding is limited because of the sample size and number of older adults included in the study, it further emphasizes the need for a reliable technique for goniometric measurement of scapular protraction and retraction and may provide an additional avenue of inquiry.
In addition, the technique may also allow for the analysis of scapular movement from a functional perspective, describing the amount of purposeful motion required for specific activities and occupations. This novel goniometric technique, and initial findings supporting its interrater reliability, may provide an assessment that clinicians can use to address and restore scapular impairments to facilitate scapulohumeral rhythm as a component of occupational performance (Coppard & Lohman, 2015; Paine & Voight, 2013).
Limitations
The convenience sampling method used for the study may have contributed to participant similarities, potentially weakening external validity. Moreover, although the evaluators provided verbal instructions for and demonstrations of each scapular position, participants may not have exerted their best effort to achieve each position. In addition, intratrial variability between evaluator measurements of individual participants may have affected the results. Moving into maximal scapular retraction or protraction during the initial measurement may have increased overall scapular mobility, altering the second measurement. Moreover, the initial measurements may have contributed to an increased postural awareness, affecting the resting position of the scapula for the final measurement. A variance in height between the evaluators, who were 74 in. (187.96 cm) and 64 in. (162.56 cm) tall, respectively, may also have affected the interpretation of the goniometer measurements.
Directions for Future Research
To further critically examine the clinical reliability of this novel technique, intrarater reliability may be analyzed by repeated measurements on the same participant by the same evaluator. In addition, validity may be analyzed by comparing this technique with other methods of scapular measurement. Future research may include a more diverse sample to examine typical and functional scapular protraction and retraction using the described technique.
Implications for Occupational Therapy Practice
The results of this study provide preliminary support for the interrater reliability of goniometric measurement of scapular protraction and retraction from a superior approach. This technique may provide occupational therapists and other health care practitioners with a more precise, consistent method to quantify the motion of the scapula. This study has the following implications for occupational therapy practice: Occupational therapists may use this proposed technique during initial evaluation to establish baseline measurements of scapular retraction and protraction. Occupational therapists may use this technique to establish goals and measure therapeutic progress. The technique may serve other rehabilitative disciplines and health care providers as a standard method of scapular assessment and interdisciplinary communication.
Conclusion
This study examined the interrater reliability of a novel goniometric technique to measure scapular protraction and retraction. The results of this study support a clinically acceptable level of interrater reliability (SEM < 4°) for the technique, well below the recommended level (SEM < 8°) identified in the literature and used as the threshold for this study (MacDermid et al., 1999). Health care professionals may use this technique in future research and clinical practice for measuring scapular ROM. The researchers suggest additional empirical examination of this technique to further establish its reliability and validity.
Footnotes
Acknowledgments
We acknowledge the faculty and students of the Huntington University OTD Program for their support of this study.