
Abstract
This results of this study indicate that a hybrid model of telerehabilitation incorporating both in-person and distance-based treatment is likely optimal for SCI.
Spinal cord injury (SCI) is a life-altering injury that often has a negative physical, emotional, and financial impact (Dallolio et al., 2008; Nas et al., 2015; Yılmaz et al., 2014). Treatment is highly specialized, requiring an explicit understanding of SCI, including the body’s response to injury and the required interventions. People who sustain an SCI often encounter barriers to accessing specialized health care, including lack of proximity to a specialized facility, transportation, and caregiver support (Cottrell et al., 2017). These limitations may adversely affect the person’s functional outcome and overall independence level.
Telehealth and telerehabilitation services provide an alternative to in-person health care delivery, permitting a remote mode for the education, training, and health care support that are needed for adjustment to injury. Telehealth is the use of telecommunication by health care professionals to deliver health care information remotely to clients and other providers over a distance-based platform (American Occupational Therapy Association [AOTA], 2010). Telerehabilitation is the remote delivery of rehabilitative health care by physical therapists, occupational therapists, speech-language pathologists, and recreational therapists (AOTA, 2010; Eichler et al., 2017; Hauber et al., 1999; Russell et al., 2011).
Previous telehealth studies have evaluated client satisfaction and effectiveness with various populations. Van Straaten et al. (2014) studied client satisfaction after supervised physical therapy via video conferencing for shoulder rehabilitation. Clients reported decreased pain and improved functional outcome scores; the authors concluded that supervised video conferencing was an appropriate alternative treatment for this population. Coulter et al. (2017) compared a web-based physical therapy program and a conventional, in-person physical therapy program and found good participant compliance in the telerehabilitation group, indicating that it is a feasible and acceptable option. However, the authors concluded that further research would be needed to confirm their results over a longer intervention time frame. Overall, participants have evaluated telerehabilitation positively (Coulter et al., 2017), finding it to be convenient and motivating (Eriksson et al., 2011; Shulver et al., 2017).
In this qualitative study we explored the following two research questions: (1) What are occupational therapists’ experiences with and perspectives on telerehabilitation use with the SCI population? and (2) What are occupational therapists’ perceptions of the benefits of and barriers to telerehabilitation use with the SCI population?
Study Significance
Although research related to clients’ telehealth perspectives is available (Coulter et al., 2017; Eriksson et al., 2011; Shulver et al., 2017), a knowledge gap exists concerning practitioners’ perspectives. Adding to the telerehabilitation research may provide additional evidence for clinical practice implementation and address potential barriers to its use. In addition, the coronavirus 2019 (COVID-19) pandemic has increased the need for and use of telehealth services, so understanding therapist and client perceptions may facilitate future use.
Method
Study Design
This study had a qualitative design that facilitated a richer understanding of clinicians’ telerehabilitation experiences, perspectives, thoughts, and opinions. A basic interpretive approach allowed for an exploration of multiple clinicians’ perceptions of telerehabilitation, including its significance, implication, and value (Merriam, 2002).
Purposeful sampling and rational judgment informed sample recruitment that adequately represented a range of perspectives and experiences. The two inclusion criteria were licensed occupational therapist with (1) at least 5 yr clinical experience working with the SCI population and (2) inpatient SCI experience of at least 1 yr. Exclusion criteria were (1) inability to speak and read in English and (2) inability to participate in the time frame allotted for data collection.
Because of this study’s preliminary nature, and to limit data saturation, a sample of 6 to 8 participants was deemed optimum to accurately analyze and understand participants’ thoughts. Eleven clinicians were invited to participate, of whom 5 responded with interest. One additional clinician, on a reserve recruitment list, was invited and included in the study, resulting in 6 clinician participants. Institutional review board (IRB) approval was obtained from the University of Maryland before recruitment. Data collection occurred from September 2018 through January 2019.
Procedure
Recruitment
Participants were recruited from the University of Maryland Rehabilitation and Orthopedic Institute (UMROI) and through other professional contacts of the primary researcher (Ritu Goel). We selected UMROI as a recruitment site because of its location, affiliation with the University of Maryland Shock Trauma Center, experience with SCI care, and Commission on Accreditation of Rehabilitation Facilities accreditation.
A recruitment email invited 11 occupational therapists with inpatient and outpatient SCI rehabilitation experience. The first 6 interested occupational therapists (who met the inclusion and exclusion criteria) to respond to the recruitment email were sent a subsequent email that included a cover letter, information sheet, and demographic questionnaire. Invitees were notified that a $25 Amazon electronic gift card would be issued in exchange for participation. A completed demographic questionnaire, which served as a participant agreement document, was requested of interested invitees.
Informed Consent
The information sheet was sent as an attachment to the recruitment email, providing prospective participants with all informed consent guidelines. The University of Maryland IRB classified this study as “exempt” and thus as not requiring a signed informed consent form before participation. All included participants were notified that their involvement was voluntary.
Instruments
Two instruments were used for data collection: (1) a demographic questionnaire and (2) a semistructured interview.
Demographic questionnaire
The demographic questionnaire requested information on each prospective participant, thus assisting in the development of a diverse sample. Participants were discouraged from including any personal identifiers (e.g., name, employer) on the questionnaire.
Semistructured interview
The single, 1:1, semistructured interview included the following three topics: (1) telerehabilitation in occupational therapy practice, (2) benefits of and barriers to use, and (3) appropriateness of and feasibility to use with SCI. After participants provided consent, they were emailed interview questions, allowing them time to prepare thoughts and responses.
Interviews were privately scheduled between Goel and each participant, were conducted in person, and required a single meeting of approximately 30 min. Participants were requested to refrain from including personal identifiers of themselves or others, to maintain confidentiality. Interviews were audio recorded, transcribed, and reviewed by Goel to ensure accurate, verbatim transcriptions. During transcription, all personal identifiers, if any, were omitted to maintain participant anonymity.
Positionality of Researcher
Goel, an occupational therapist with 11 yr of clinical experience (including clients with SCI), met all inclusion criteria, held personal views on the research topic, and was a professional colleague of all clinicians invited to participate. She was not a participant in the study; however, she did conduct all interviews. To reduce bias, she reflected on her own thoughts and feelings toward the research topic before, during, and after each interview.
Data Analysis
Member Checking
Each transcript was emailed to the respective participant for member checking. Participants were requested to validate, clarify, and addend their respective interview data, as needed, to ensure response accuracy.
Coding
The coding process began with individual, random interview excerpt coding by Goel and a second researcher (Paula Richley Geigle). Excerpt codes were compared and discussed in regard to congruency and to ensure the essential meaning of the transcript was illuminated. After excerpt coding, all six full transcripts were independently coded by both Goel and Geigle, followed by a review and further comparison. During the secondary review, codes were compared between interviews and then refined and condensed. As the coding process continued, emergent concepts were compared with one another and categorized. Both researchers independently categorized the data and identified themes and subthemes. Goel and Geigle discussed and agreed on emergent themes and decided that Goel would explore the further grouping of these themes into broader, overarching categories.
The constant comparative method integrates collected data with the emerging categories, allowing for further code specification and identification of recurrences in the data and arising trends as well as management of data saturation (Boeije, 2002 ; Creswell, 2007). Using this method, we determined six interviews sufficient to provide full, rich data given that no new themes emerged on analysis of the sixth interview.
Triangulation
To further establish trustworthiness, a third researcher (Laura Santurri) reviewed the emergent themes and codes. Goel and Santurri conversed and further refined themes and subthemes and developed a theme table (Table 1). In addition, a theme schematic was created to portray a visual representation of outcomes, depicting the correlations between themes (Figure 1).
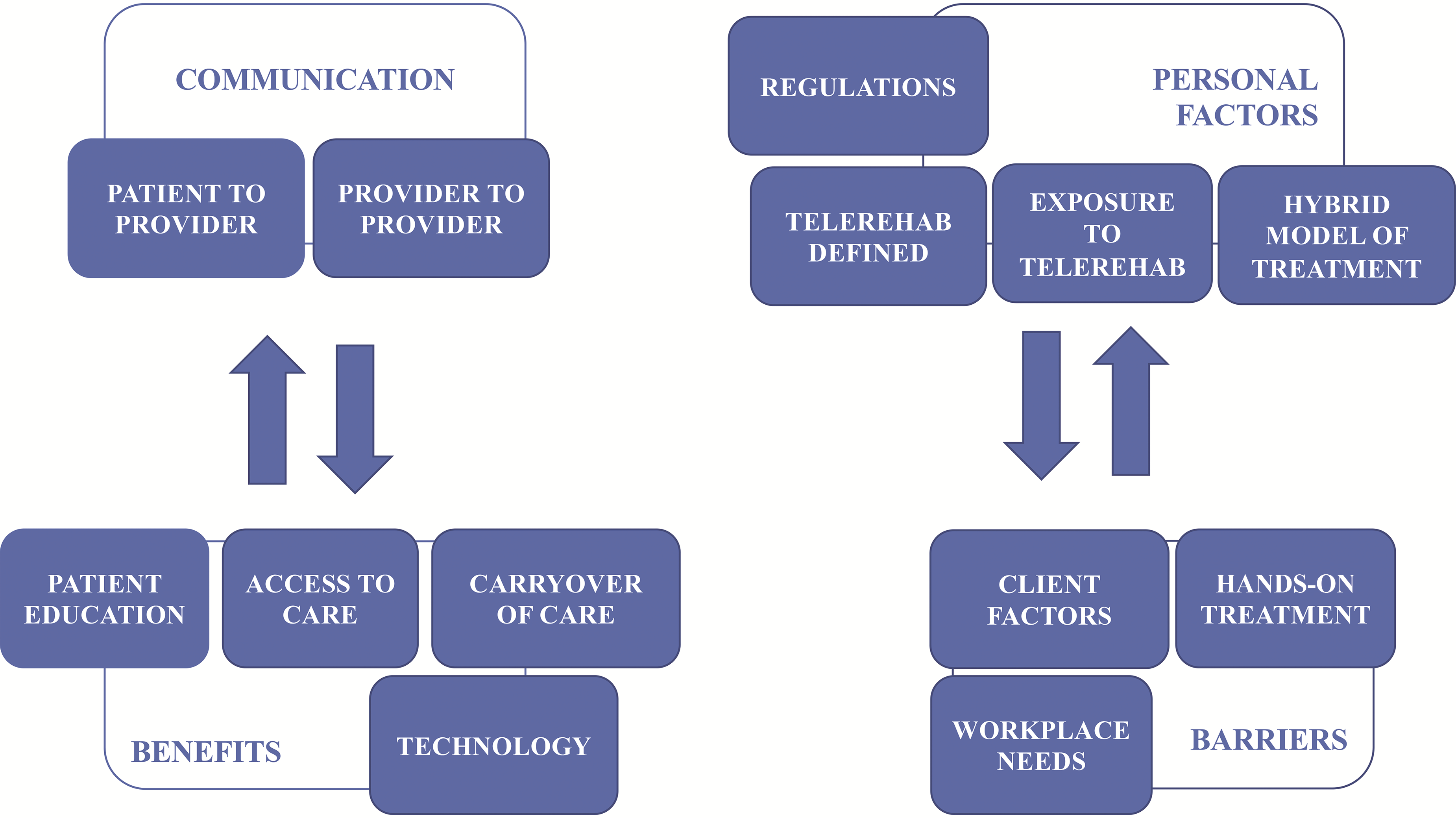
Visual representation of resultant themes and associated subthemes, with indication of the correlation between emergent themes.
Theme, Subthemes, and Codes Used
Note. ADLs = activities of daily living; HEP = home exercise program; IADLs = instrumental activities of daily living.
Findings and Results
Sample Description
Six occupational therapists (5 women and 1 man) were included in the study, representing a broad age range and various experience levels (Table 2). All participants had prior work experience with SCI. At the time of data collection, the sample consisted of 2 educators at a local university, who did not hold a clinical position, and 4 clinicians, who provided treatment at UMROI.
Participant Demographics
Note. SCI = spinal cord injury.
Themes
Four overarching themes emerged: (1) communication, (2) personal factors, (3) benefits, and (4) barriers.
Communication
The development and incorporation of electronic medical records within hospital systems has improved overall efficiency and communication among providers, hospital systems, and clients. Participants generally agreed that “the move toward electronic documentation has [led to fewer] delay[s]” (Participant 5 [P5]), thereby allowing “health care providers [to] more easily access and share documentation, lab results, [and] X-rays” (P4). In addition, P2 stated that by “linking the medical records electronically, we are able to see when people are in other [hospital] systems” if those systems use the same software platform, for improved continuity of care. P1 explained that telerehabilitation may provide “socially isolated” clients “the opportunity to interact with a doctor, therapist, or psychologist” remotely, to address their needs.
Personal Factors
Five participants (P1–P5) voiced concerns regarding their lack of knowledge about and exposure to telerehabilitation as well as regulations for implementation and reimbursement. P2 requested “a general introduction” to telerehabilitation, “what it really means, and how it would be implemented.” Similarly, P1 was interested in “researching the ethics and legal aspects of licensure . . . knowing what we can and can’t do. . . . Can you provide service if you’re not in the same places?” Concerning privacy and security, P6 encouraged “protect[ing] people’s health information,” suggesting that treatment should be provided “someplace where it’s going to be private.”
P5 commented on the difficulty in exclusively using telerehabilitation for SCI treatment, stating, “I just don’t see it as a full supplement to that hands-on [engagement] with your patients.” Therefore, a “hybrid model” (P1) or “collaboration” (P3) of virtual and in-person visits was suggested to “reduce the frequency of in-person visits” (P1).
Benefits
Increased access to health care, client education, and carryover of care were identified as benefits of telerehabilitation services. All participants (P1–P6) felt that barriers to attending therapy could be rectified with virtual access to health care. Telerehabilitation would increase “access to specialty medicine, especially for people in rural areas . . . they can access that unique knowledge” (P1) and “help to spread the services out to those underserviced areas” (P6). As a preventive measure, P6 identified “using telerehab” as an “option to keep people out of the hospital [and] prevent readmissions.” P2 felt comorbidities or medical status might have affected attendance; “if not leaving the house could be an option, . . . a lot of people [could] access therapy more consistently.” P5 stated that for a “patient in a wheelchair or power chair [in instances of] inclement weather . . . it may be easier to access health care [virtually] if they’re limited [in] their ability to get in and out of their house.”
In addition, telerehabilitation was suggested as a medium for client education for “wound [care]” and “mentor[ing]” (P1), and “educational videos” of “ADLs, . . . sexuality, transferring, [and] exercise” performance (P2). P6 suggested that telerehabilitation may “help caregivers [and] patients ease their anxiety” postdischarge by providing access to therapists during the transition. P5 added,
We spend a lot of time preparing our patients for discharge. They’ve experienced these life-changing injuries and basically have to relearn how to live their lives and survive, so you don’t always get to find out how well patients are doing after they’ve left; [telerehabilitation] would be a great way to follow up with them.
In preparation for discharge home, therapists perform in-person evaluations of the client’s home environment to assess safety and accessibility and to provide equipment recommendations. Three participants (P1, P4, P5) stated that in-person home assessments can be difficult to schedule and attend; however, technology may ameliorate these issues. P5 mentioned that “being a go-to for our trauma center, they take patients from all over the state, and so it’s not easy to just get in the car and drive two to three hours to a patient,” suggesting that telerehabilitation may be an option “to get a visual perspective of the patient’s home” without having to drive there.
Participants also suggested that technology use may increase client engagement (P2, P3, P4) and functional independence (P3, P4) and improve social interaction skills (P1). P4 stated that clients will have “a positive attitude about learning because it’s helping to give them more independence,” identifying speech-to-text transcription technology and voice-activated controls as available tools that promote independence.
Barriers
Hands-on manual treatment, workplace technology needs, and client factors such as financial status and physical and cognitive limitations were identified as barriers to telerehabilitation. P6 stated that telerehabilitation “might not be appropriate for everybody or at certain stages in the rehab process.” Participants identified concerns with the cessation of manual treatment and hands-on care, expressing that “with some spinal cord–injured patients . . . the nature of our therapy is so hands on,” (P2) and telerehabilitation could “stop the application of manual techniques . . . which are really paramount” (P1). Also, during a telerehabilitation session, “if an issue arises . . . I can’t step in to intervene” (P5).
Client factors such as socioeconomic and financial status (P1, P3, P4), cognition (P1, P5), physical ability (P4), hearing and vision limitations (P5), and caregiver assistance (P2, P3, P6) were identified as potential barriers to telerehabilitation use and implementation with clients with SCI. Regarding financial status, P3 stated that “we would need to ensure that they have the technology; . . . for many of my past clients that would’ve been an issue.” Caregiver support to assist clients with transfers (P6) and provide manual assistance (P2) were also seen as potential barriers to accessing telerehabilitation services:
Ensuring that they have family support, that somebody could be there to help carry out some of the things . . . especially [clients with] the higher level spinal cord injuries, which are the ones I believe would benefit the most, would need to have someone there to assist them. (P3)
Thematic Analysis and Discussion
In this qualitative study we explored urban occupational therapists’ perspectives on benefits of and barriers to telerehabilitation for clients with SCI. At the study development stage, a gap in the research existed regarding the occupational therapists’ perspective on telerehabilitation use. Rich, qualitative evidence exemplifying practitioners’ impression of telerehabilitation with this population may narrow this knowledge gap.
To highlight the participants’ clinical background, they are referred to as “study clinicians” for the remainder of this article. Overall, all 6 study clinicians expressed interest in learning about telerehabilitation because of a lack of knowledge and exposure.
Benefits of Telerehabilitation
Limitations in functional mobility and independence may increase depression risk (Hwang et al., 2016; Nas et al., 2015) and social isolation (Barclay et al., 2016; Ward et al., 2007; Whiteneck et al., 1992) in people with SCI. Hwang et al. (2016) reported that engagement in leisure activity after SCI minimized and prevented depression while increasing overall life satisfaction. Such social interaction opportunities (i.e., video conferencing for mentoring or virtual coaching) may be provided via telehealth. Steel et al. (2011) found that clients were highly satisfied with video conferencing as a mode of treatment delivery, achieving similar treatment outcomes as clients receiving in-person treatment without compromising the development of a strong therapeutic relationship. Shulver et al. (2017) found that older adults (ages 60–92 yr) were pleased with the convenience, motivation, and self-awareness that telerehabilitation promoted.
Regarding limitations in activities of daily living (ADLs) and the assistance needed for community outings such as grocery shopping, Ward et al. (2007) found that clients expressed increased comfort in their own functional ability and problem-solving skills when they had access to an occupational therapist. P4 stated that technology helps increase clients’ independence through computer applications and voice-activated technology for home management, including automated lights, television controls, and grocery shopping and delivery. Education on technology use for home management skills may be addressed with telerehabilitation, providing this population with an alternate method of achieving independence.
Therapists and clients rarely interact after clients have been discharged from inpatient rehabilitation. As inpatients, clients and caregivers receive an overwhelming amount of education in preparation for discharge. Study clinicians hypothesized that telerehabilitation services may provide a method for education review and a mode to track postdischarge progress, thereby ensuring adequate carryover of care in the home or an alternative postdischarge environment and potentially preventing hospital readmissions. Similarly, Eriksson et al. (2011) found that clients appreciated access to a therapist for feedback and support after surgery and concluded that clients felt more capable and motivated after a telerehabilitation session. Moreover, clients and caregivers expressed a positive perception of telerehabilitation with improved home program carryover and motivation (Hung & Fong, 2019).
Lack of proximity to a specialized rehabilitation facility is a limiting factor in client attendance and follow-through with therapy (Hauber et al., 1999; Mathewson et al., 2000). Tousignant et al. (2006) determined telerehabilitation to be an acceptable alternative delivery method if in-person therapy services are unavailable, which may help rectify limitations in therapy attendance (i.e., transportation, proximity, caregiver availability), aligning with 100% of our study clinicians’ remarks. Currently, multidiscipline health care professionals use telehealth to increase service accessibility (Eichler et al., 2017; Hauber et al., 1999; Russell et al., 2011; Tousignant et al., 2011), a mode of accessing specialty health care study clinicians felt that clients with SCI would benefit from.
Barriers to Telerehabilitation
Although telerehabilitation provides clients with an alternate method of accessing therapy, not all aspects of therapy can be performed by means of a distance-based platform; therefore, 83% of the study clinicians suggested a hybrid model. Manual skills and hands-on assistance (i.e., objective measurements, manual treatment and assist, transfer training) were therapeutic facets all study clinicians found difficult to address virtually. However, 67% of our study clinicians felt that client education and home program progression were appropriate uses for telerehabilitation. Some researchers have recommended in-person treatment in conjunction with telerehabilitation, particularly when physically accessing outpatient therapy services is a challenge (Piqueras et al., 2013; Russell et al., 2011; Tousignant et al., 2011), aligning with the current study’s findings regarding a hybrid model.
People with SCI may concurrently present with a traumatic brain injury that is causing cognitive deficits along with physical limitations. Brennan and Barker (2008) found that cognitive, physical, visual, and speech deficits affected client interest in and ability to use technology—an important confounder—and concluded that health care professionals should consider client factors when developing treatment plans and delivery methods; this, too, is in alignment with the current study’s findings. People with SCI may present with limited hand function, which hinders computer use, and thus they may require assistance (Coulter et al., 2017). Although the study clinicians suggested caregiver support as a possible solution to accessing telerehabilitation services, this unfortunately may not be feasible for all people, coinciding with P6’s statement that telerehabilitation services may not be appropriate for all clients.
Knowledge Gap
Our findings and results supplement the existing literature on the use and understanding of telerehabilitation and address gaps in the literature while articulating practitioner concerns and sentiments regarding telerehabilitation for SCI care. A residual knowledge gap exists, however. The study clinicians discussed client accessibility, regulations, and the logistics of implementing telerehabilitation, none of which have been addressed in prior studies. Our findings may encourage occupational therapy board members and legislators to address practitioner concerns regarding telerehabilitation use, such as billing, out-of-state service delivery, and rules and regulations for use (i.e., licensure, scope of practice).
Limitations
Limitations include researcher bias, the sample size and cohort, purposeful sampling, and the interview time frame. Although the primary researcher (Goel) met all inclusion criteria, steps were taken to limit researcher bias (see “Method” section). Moreover, participants were recruited from a single medical center, which potentially limits generalizability. A more diverse cohort from other hospital systems and states could produce different themes.
Areas for Future Research
This study provides preliminary information on urban occupational therapists’ perspectives on telehealth and its potential use for SCI care. Future research and follow-up studies may include reinterviewing the study clinicians to identify changes in perceptions of telehealth after the COVID-19 pandemic. Examining telerehabilitation implementation with the SCI population would help determine its effectiveness and identify interventions that are appropriate for virtual delivery.
Implications for Occupational Therapy Practice
In practice, clients benefit from consistent therapy that is not impeded by transportation or other nonmedical barriers to attendance. Telerehabilitation may increase client access to therapists to address concerns such as ADL skills, transfers, equipment, home program progression, and possible postdischarge preventive care. Our findings add to the general literature on telerehabilitation, specifically relating to SCI care, and have the following implications for occupational therapy practice: Therapists and board members should consider potential areas for telerehabilitation use in occupational therapy with the SCI population as applicable and acceptable modes of treatment. Practitioners may want to address concerns with telerehabilitation use with the SCI population before implementation with client care. Our findings may assist in the development of a hybrid model of treatment that maximizes therapy accessibility for clients without inhibiting manual and hands-on treatment. The findings may facilitate an alternative treatment delivery method for specialized care to underserved populations.
Conclusion
The results of this study should be considered hypothetical and preliminary, given that telerehabilitation was not implemented with clients. However, after study completion, the COVID-19 pandemic has brought us social distancing requirements, legislative changes, and the closures of many small businesses, including outpatient therapy clinics, all of which have hastened the implementation of telerehabilitation on a wider scale. In 2020, Maryland Governor Lawrence Hogan issued Executive Order 20-04-01-01 (“Order of the Governor,” 2020), suspending “certain state and local statutes, rules, and regulations regarding confidentiality during use of various video and telecommunications applications” in an effort to “protect the public health, welfare, and safety.” Moreover, the Maryland Department of Health (2020) permitted implementation of telehealth services via nonsecure distance-based platforms (e.g., Skype, FaceTime), thereby expanding its accessibility.
This study shows practitioner interest in and a positive outlook for the use of telerehabilitation services. A hybrid model was proposed to provide a combination of in-person and virtual visits given that all aspects of treatment are difficult to address remotely. Our findings can be used to facilitate the incorporation of telerehabilitation into the broader scope of health care, expanding therapy services and increasing accessibility and thus potentially improving client outcomes. With the recent need for telerehabilitation, knowing therapists’ and clients’ responses is vital to its advancement and a further understanding of its role in health care. Therefore, future research is needed as the profession moves toward implementation.
Footnotes
Acknowledgments
Funding for participant reimbursement was provided by the University of Indianapolis, College of Health Sciences, Indianapolis, IN. The authors thank the study participants for their time and contribution to research and clinical practice.