
Abstract
This study provides preliminary support for MealSense, a web-based program designed to help parents of children with autism spectrum disorder address feeding difficulties related to sensory integration challenges.
Feeding is a fundamental occupation, one that is needed for optimal health, and it is an area frequently addressed by pediatric occupational therapists. Feeding difficulties, such as selective eating, negative mealtime behaviors, food refusal, and reduced acceptance of textured foods (Cermak et al., 2010; Kral et al., 2013; Kuschner et al., 2017; Marshall et al., 2014; Nadon et al., 2011; Provost et al., 2010; Zimmer et al., 2012), are prevalent in 48% to 89% of children with autism spectrum disorder (ASD), limiting successful participation in the essential daily occupation of eating and affecting the quality of life of many children and their families (Ledford & Gast, 2006). Parents of children with ASD report high stress levels and identify eating as one of the most frustrating occupations for their child (DeMyer, 1979; Hayes & Watson, 2013).
Sensory integration is defined as “the neurological process that organizes sensations from one’s body and from the environment and makes it possible to use the body effectively in the environment” (Ayres, 1989, p. 11). Multiple studies have shown a correlation between feeding challenges and sensory integration difficulties for children with ASD (Ausdereau et al., 2019; Cermak et al., 2010; Nadon et al., 2011; Schreck et al., 2004; Suarez et al., 2012). For example, sensory sensitivity—in particular tactile sensitivity—may be a factor in food selectivity for children with ASD (Cermak et al., 2010; Nadon et al., 2011; Schreck et al., 2004; Suarez et al., 2012). Thus, addressing the underlying sensory integration challenges related to feeding may lead to improved mealtime behaviors.
Parent education, a term that refers to programs that are designed to teach parents skills or provide them with information (Schultz et al., 2011), is an evidence-based component of feeding intervention for children with ASD (Adamson et al., 2013; Howe & Wang, 2013). Parent education can provide natural learning opportunities in the home that extend intervention beyond the clinic environment (Steiner et al., 2012). Parent-implemented intervention is also cost-effective and can increase the rate of progress in therapy (Steiner et al., 2012).
Recent interest in online strategies and telehealth intervention for people with ASD has been successful in meeting parents’ specific educational concerns (Kobak et al., 2011; Vismara et al., 2013.) Web-based parent education programs may address the identified barriers preventing parents from attending educational programs outside of the home, such as travel time, cost, and child care, as well as the additional time needed to schedule programs in real time and costly equipment that is required (Heitzman-Powell et al., 2013; Vismara et al., 2013). Moreover, parent education delivered virtually may be useful for times when in-person intervention is not possible, as has been the case during the coronavirus disease 2019 (COVID-19) pandemic.
To address the need for an online program that educates parents of children with ASD about the impact of sensory integration challenges on feeding and that provides a means to carry over feeding skills from the therapeutic environment into the home, we developed MealSense©, a web-based parent education program.
MealSense Program Development
MealSense is a self-paced online educational program for parents of children with ASD who have feeding difficulties related to challenges in sensory integration. We developed the MealSense program using current evidence in Ayres Sensory Integration® (ASI; Schaaf & Mailloux, 2015,) and feeding, along with feedback from experts in sensory integration, feeding, knowledge translation, and online instruction. Although MealSense is primarily a sensory-based feeding program, it acknowledges that feeding is a multifaceted occupation that may be influenced by factors related to motor, behavior, and social functioning. Designed as a supplement to direct intervention, MealSense targets the transfer of feeding skills from the clinic into the home environment through incorporation of knowledge translation strategies and an emphasis on education about sensory integration factors that may contribute to feeding difficulties. A detailed outline of MealSense content is provided in Table 1.
MealSense Content Outline
Note. ASD = autism spectrum disorder; ASI = Ayres Sensory Integration; NA = not applicable.
ASI is an evidence-based practice for children with ASD that is frequently requested and used (Schoen et al., 2019). Given the correlation between feeding challenges and sensory integration difficulties, ASI principles (Ayres, 1979; Schaaf & Mailloux, 2015) were a key perspective included in the MealSense program. MealSense includes sensory-rich experiences, encouraging active engagement of the child and offering activities that are the just-right challenge (Parham et al., 2011).
The Knowledge to Action (KTA) framework (Field et al., 2014) and knowledge translation strategies were also included in the MealSense program. KTA is a complex and dynamic process of knowledge creation and application that facilitates knowledge use by guiding the translation of knowledge into sustainable and evidence-based interventions (Field et al., 2014). KTA strategies used in MealSense included adding parent reflections, tips for completing the modules, and modification of parent worksheets to allow monitoring of progress.
The purpose of this project was to answer the following three research questions: Do expert reviewers consider MealSense to be consistent with the principles of ASI? Do expert reviewers view MealSense as adhering to best practices in feeding? Do parents of children with ASD and feeding difficulties rate MealSense as acceptable and useful?
Method
In this descriptive study, we distributed electronic surveys (Qualtrics) and a MealSense program link to expert reviewers and parents of children with ASD and feeding difficulties to obtain feedback about the program’s content, acceptability, and usefulness.
Participants
Expert reviewers (n = 5), recruited through convenience sampling by emails sent to local pediatric clinicians with experience in both sensory integration and feeding, were pediatric occupational therapists who met the following four inclusion criteria: (1) a minimum of 4 yr of clinical experience in occupational therapy, (2) advanced training and education (certification) in sensory integration, (3) a minimum of 3 yr of experience working with children who have feeding difficulties, and (4) a minimum of three pediatric feeding continuing education courses. Parent participants (n = 5) were recruited through convenience sampling from the first author’s (Audrey Trewin’s) place of employment, a large therapy clinic devoted to treatment of children with neurodevelopmental disorders. Eligibility criteria included being fluent in English and having a child between ages 2 and 8 yr with a diagnosis of ASD (no other medical diagnosis) and who had at least one feeding goal related to sensory integration difficulties on a current treatment plan.
Five parents of children with ASD reviewed the program. Mothers made up 80% of the sample, and fathers made up 20%. Most (80%) ranged in age from 35 to 39, and some (20%) were older than age 45; 40% were White or Caucasian, 40% were Hispanic, and 20% were Asian. Eighty percent of participants reported having two dependents in the home (80%), and 20% had more than five dependents in the home. Twenty percent had completed high school, 60% had completed college, and 20% had completed graduate school.
Data Collection
This study was determined by the Thomas Jefferson Institutional Review Board to be exempt from review.
Instruments
Program-specific surveys were developed and reviewed by a survey expert for purposes of clarity and to ensure that the items were clear and relevant to the research area. Survey questions were rated on a Likert scale that ranged from 1 (strongly disagree) to 4 (strongly agree) and were distributed via Qualtrics. The expert survey was designed to evaluate program consistency with ASI (12 questions) and best practices in feeding (7 questions). The parent survey was designed to evaluate program acceptability, defined as adherence, reasonable time to complete, usability, clarity, and satisfaction, and program usefulness, defined as applicability and transferability (Burchett et al., 2013 ; Cooper et al., 2007; Kuschner et al., 2017). We also emailed a program link to parents for access to MealSense content and an anonymous survey link (13 questions) to evaluate acceptability and usefulness of MealSense. A table of revisions was developed to summarize expert and parent feedback and identify modifications.
Data Analysis
Data were analyzed by determining the mean score for each question. Because ratings of 3.0 and 4.0 indicated agreement, a mean score of 3.0 or higher was considered acceptable.
Results
Expert Reviews of Content for Consistency With Ayres Sensory Integration
The results from expert reviewers (n = 5) revealed a mean rating of ≥3.0 on each of the 12 questions related to adherence to ASI principles, indicating that MealSense content was consistent with the principles of ASI. As shown in Figure 1, experts indicated that MealSense content addresses sensory exploration during mealtime (M = 4.0), provides mealtime tasks at the just-right level for the child (M = 4.0), factors the child’s interests into mealtime-related experiences (M = 4.0), addresses mealtime factors related to posture (M = 3.8), encourages parent–child collaboration during mealtime (M = 3.8), and provides strategies that support the child’s ability to be successful during mealtime (M = 3.8). Survey items with the lowest mean score (3.0) but that still met criteria were related to MealSense modules that address ocular skills and bilateral motor control.
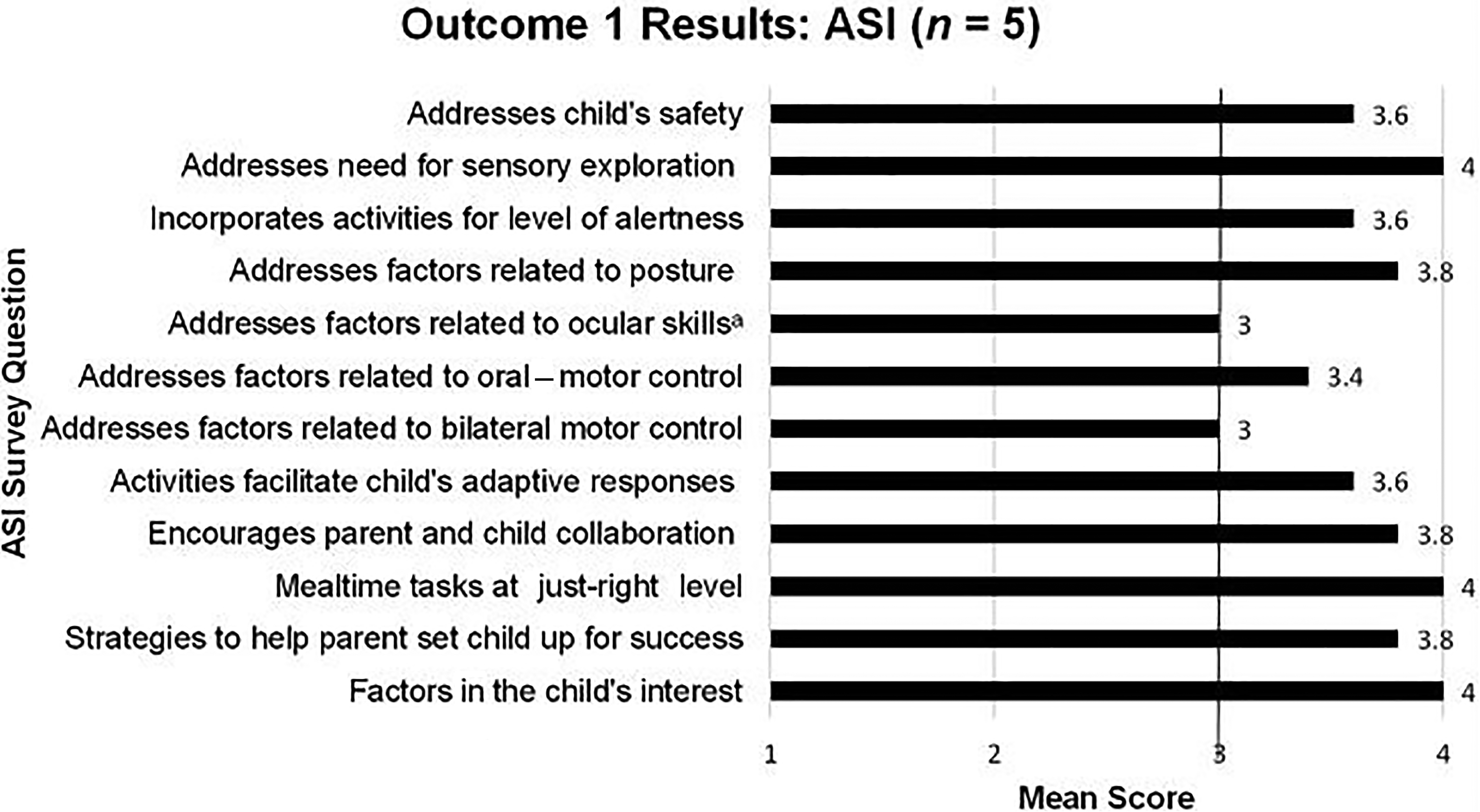
Expert data related to consistency with ASI.
Expert Reviews of Content for Inclusion of Best Practices in Feeding
The results from expert reviewers indicated a mean rating ≥3.0 on each of the seven questions related to best practices in feeding. As shown in Figure 2, the highest ratings were as follows: the modules teach feeding as a multifaceted occupation (M = 4.0), parent education is used to support the child’s feeding (M = 4.0), and environmental barriers to mealtime participation are considered (M = 3.8). Survey items with the lowest mean score but that still met criteria included those that addressed how MealSense incorporates behavioral strategies as appropriate (M = 3.4), addresses acquisition of feeding in a sequential way (M = 3.4), and directs parents to consider environmental strengths (M = 3.4).
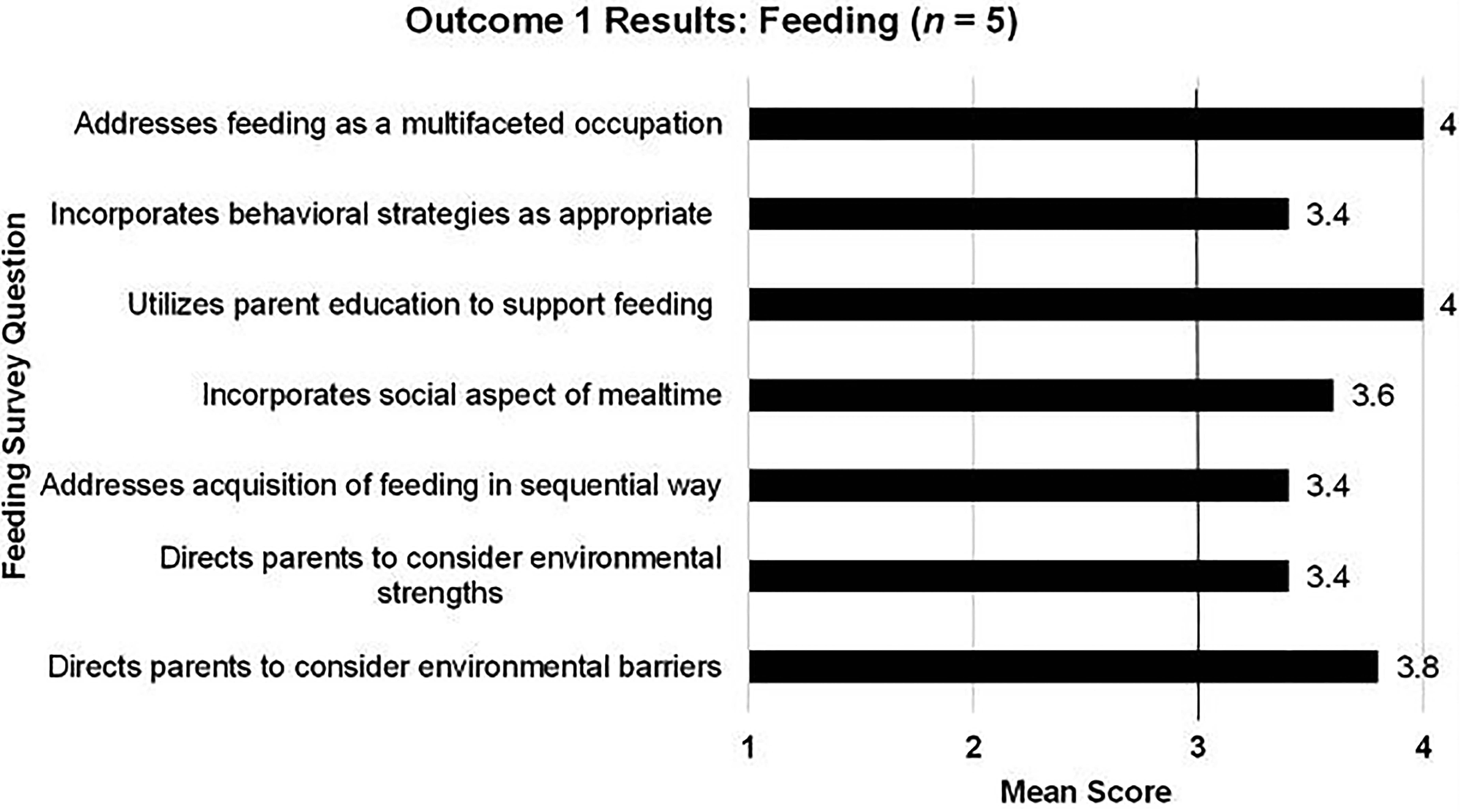
Expert data related to best practices in feeding.
Parent Reviews of Acceptability and Usefulness
The results from parent participants (n = 5) indicated a mean rating ≥3.0 on each question. As shown in Figure 3, the highest survey responses indicated that the modules could be completed in a reasonable amount of time (M = 4.0), that information is presented in a logical way (M = 4.0), and that modules were easy to understand (M = 4.0). High survey ratings were also obtained on the following questions: each module was easy to navigate (M = 3.8), entire website was easy to navigate (M = 3.8), am satisfied with the information (M = 3.8), would recommend the program (M = 3.8), and information applies to feeding needs (M = 3.8). The survey item with the lowest mean score (M = 3.0) but that still met criteria included those addressing whether MealSense parent activities were perceived to be completed in a reasonable amount of time.
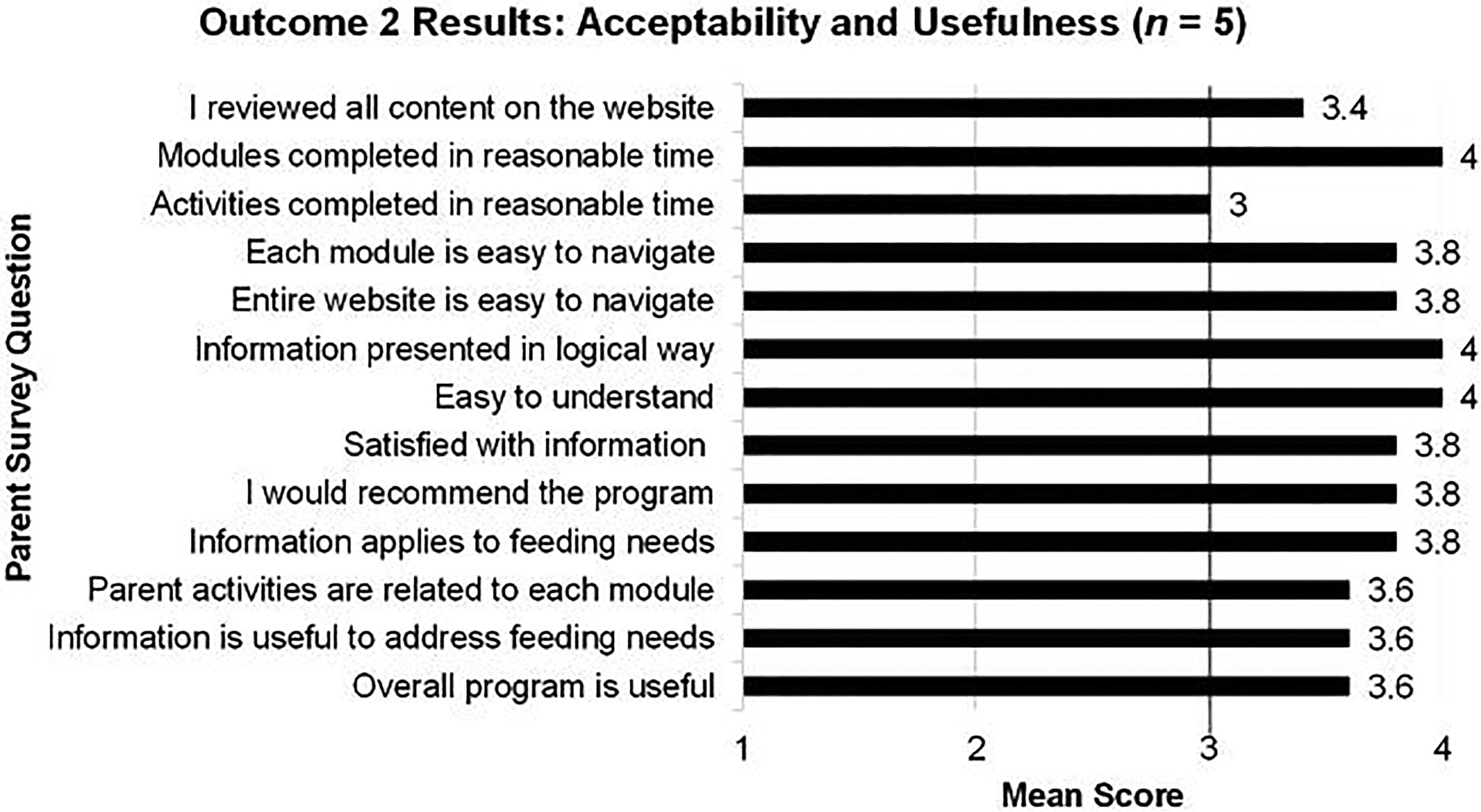
Parent data related to acceptability and usefulness.
Discussion
The findings from this study suggest that MealSense demonstrates consistency with ASI and best practices in feeding and that parents perceive it as acceptable and useful. To our knowledge, this is the first evidence-based, online parent feeding support program for children with ASD that emphasizes education about the sensory integration factors that can contribute to feeding difficulties.
Feeding is an important occupation that contributes to a child’s growth and development (American Occupational Therapy Association, 2017), and successful mealtime participation can enhance a family’s quality of life (Ausderau et al., 2019; Henton, 2018; Meral & Fidan, 2015). Family-centered feeding interventions that address feeding and mealtime behaviors for children with ASD, such as for the MealSense program presented here, are needed (Henton, 2018), and the findings from this study lend support to the MealSense program.
As a parent education program, MealSense is not intended to provide direct intervention that adheres to principles of ASI as designated by the ASI Fidelity Measure (Parham et al., 2007). However, our findings suggest that ASI principles were readily operationalized into the MealSense program, showing that these principles may be used outside of the traditional direct intervention, in an online parent education program.
One important aspect of the MealSense program is that it is an online parent education tool that supports the occupation of feeding in the home environment. Implementation of virtual interventions can become unexpectedly important, as has been the case during the COVID-19 pandemic. Because families often have not been able to participate in face-to-face interventions during this time, the need for innovative program delivery models in a virtual environment was even more salient (Jang et al., 2012; Steiner et al., 2012).
Potential benefits of implementing a program such as MealSense in this format include its cost-effectiveness and accessibility. Challenges may include the lack of ability to answer questions for parents in real time and parent completion of modules in a timely manner. Using MealSense as a supplement to direct intervention may help address these potential downsides of the program.
Descriptive feedback and quantitative data from expert reviewers identified principles of ASI that may benefit from further development, including addressing oral–motor skills and bilateral motor control. Similarly, best practices in feeding that may benefit from further emphasis include addressing behavioral strategies, sequential development of feeding skills, and considering environmental strengths. Future iterations of MealSense may benefit from more emphasis on these specific areas.
Limitations
Although the MealSense program showed strong adherence to ASI and best practices in feeding, more research is needed to evaluate its efficacy. Next steps will include pilot testing with parents to provide initial data about the efficacy of MealSense related to changing feeding behaviors and participation in mealtime in the home setting.
Limitations of this study include that both participant groups were convenience samples, which may limit our ability to generalize the findings to other populations. In addition, the sample size was small (n = 5) for both experts and parents, and response bias may have influenced reviewer feedback.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: Knowledge translation strategies may facilitate the usefulness of parent education programs related to sensory integration and feeding. MealSense provides an example of an online educational tool for parents of children with ASD and may be especially useful for times when in-person visits are not possible.
Conclusion
A need exists for parent education feeding programs for children with ASD that address the sensory integration factors that can affect feeding behaviors and facilitate the transfer of skills into the home. This study provides preliminary support for MealSense, a web-based program designed to educate parents about their child’s sensory integration related to addressing the feeding needs of children with ASD and for supporting the carryover of skills into home.
Footnotes
Acknowledgments
We thank Isabelle Beaudry Bellefeuille for reviewing the first iteration of MealSense and providing feedback related to feeding content. We also thank Amy Carroll for contributions in knowledge translation and Mary Cohen for feedback related to online instruction.