
Abstract
The LDCDQ–TW demonstrated sound reliability and validity and can support the early identification of young children at risk of developmental coordination disorder in Taiwan.
Developmental coordination disorder (DCD) is characterized by motor difficulties that result in physical and social participation limitations at home and school and in the community (American Psychiatric Association, 2013; Bart et al., 2011; Izadi-Najafabadi et al., 2019; Jasmin et al., 2018; Miyahara et al., 2017; Smits-Engelsman et al., 2003; Smyth & Anderson, 2000). The reported prevalence of DCD ranges from 4% to 19% of school-age children, depending on the test and criteria used (Zwicker et al., 2012). Early childhood motor impairments associated with DCD may persist into adulthood (Kirby et al., 2013; Rasmussen & Gillberg, 2000), leading to higher rates of emotional and behavioral difficulties (Cairney et al., 2010; van den Heuvel et al., 2016), increased risk of obesity (Cairney et al., 2005; Hendrix et al., 2014), and other health-related risks (Faught et al., 2005). Given the pervasive and long-term effects of DCD, early identification of children with suspected motor difficulties is essential to prevent secondary sequelae. In Taiwan, children ages 3 and 4 yr are a key group referred for early intervention support, and access to culturally suitable and age-appropriate assessment tools for this age group is of high importance.
Occupational therapy evaluations rely on many different types of instruments, with the use of reliable and valid screening questionnaires a particularly time- and cost-effective strategy (Green et al., 2005). It has been suggested that parent questionnaires may be more valid than those completed by teachers (Blank et al., 2012), in particular for preschoolers. A number of motor screening questionnaires are available, such as the Developmental Coordination Disorder Questionnaire (Wilson et al., 2009), the DCDDaily (van der Linde et al., 2013), and the Movement Assessment Battery for Children–2 Checklist (Schoemaker et al., 2012); however, these were mainly designed for use with children over age 5 yr. The Little Developmental Coordination Disorder Questionnaire (LDCDQ; Rihtman et al., 2011) is the only motor screening questionnaire designed for children ages 3 to 4 yr.
Information gained through parent questionnaires is consistent with a family-centered perspective (Fingerhut et al., 2013; Green et al., 2005; Kuhaneck & Case-Smith, 2019; Wilson et al., 2000). The LDCDQ was designed to gain parent ratings of their children’s participation in ball, balance, and fine motor activities across home and play environments, and it has good reliability and validity (Rihtman et al., 2011). Therefore, the LDCDQ has the potential to be a highly appropriate screening tool as a first step in identifying preschoolers at risk of DCD.
Watson (2006) noted that “concepts and information that emanate from a foreign source cannot simply be transported for use in another country, where different cultural norms exist” (p. 154). Because cultural and environmental factors influence human behavior and performance (Mendonça et al., 2016), people from different cultural groups may differ in their response to, or performance on, the same assessment instrument. For example, whereas the original Hebrew LDCDQ did not reveal sex differences (Rihtman et al., 2011), a Canadian validation study did (Wilson et al., 2015). Therefore, researchers from more than 20 countries have translated the LDCDQ following a standard protocol and have examined its psychometric properties to obtain culturally specific norms (Cantell et al., 2019; Rihtman et al., 2011, 2015; Venter et al., 2015; Wilson et al., 2015). This initiative is in line with recommendations of the World Health Organization (WHOQOL Group, 1995) noting that cross-cultural translations of existing instruments provide the advantages of faster and more cost-effective instrument development processes while facilitating the connection of research findings from different countries. Thus, our aims in this study were to translate and cross-culturally adapt the LDCDQ into Mandarin Chinese and evaluate its psychometric properties in regard to Taiwanese preschoolers.
Phase 1: Translation of the LDCDQ Into Mandarin Chinese
In Phase 1 of this study, we translated the original LDCDQ into a Mandarin Chinese version suitable for use with Taiwanese preschool-age children.
Instruments
The LDCDQ is a parent screening questionnaire for children ages 36–59 mo. Originally developed in Hebrew on the basis of the Developmental Coordination Disorder Questionnaire (Wilson et al., 1998), the LDCDQ asks parents to rate their children’s performance on 15 positively phrased motor activities as compared with other children of the same age and sex. Items are rated on a Likert scale that ranges from 1 (not at all like my child) to 5 (extremely like my child). Total scores range from 15 to 75, with higher scores indicating better performance. The LDCDQ yields three subscores/factors, which were identified through an exploratory factor analysis: (1) Control During Movement (CDM), (2) Fine Motor (FM), and (3) General Coordination (GC). The original LDCDQ has good test–retest reliability (intraclass correlation coefficients [ICCs] = .84–.98) and internal consistency (Cronbach’s α = .93; Rihtman et al., 2011).
Procedure
This study received ethical approval from the National Taiwan University Hospital. As part of an ongoing cross-cultural comparison study initiated by the original authors of the LDCDQ, the questionnaire was translated into Mandarin Chinese following established guidelines (Beaton et al., 2000). Four pediatric occupational therapists undertook the translation, evaluated it for accuracy, and amended it accordingly. Two English teachers fluent in Mandarin Chinese and English, but without knowledge of the LDCDQ, performed a back-translation into English. The back-translation was then compared with the original version for semantic and conceptual equivalence. The forward–backward translation procedure was repeated until a consensus was reached. The English text was sent to the lead researcher (Tanya Rihtman) for further feedback as to whether item meanings had been preserved. After confirmation, this version was pretested for item meaning and clarity with 10 preschool children, and final revisions were made on the basis of parents’ feedback. The psychometric properties of this final Mandarin Chinese–Taiwan version, referred to as the LDCDQ–TW, were examined in this study.
Phase 2: Reliability of the LDCDQ–TW
In Phase 2, we evaluated the internal consistency, test–retest reliability, and interrater reliability of the LDCDQ–TW.
Method
Participants
Because there is no DCD screening tool for children younger than age 72 mo in Taiwan, and because face validity would suggest that the activities of the LDCDQ are appropriate for children up to 71 mo, the age range was extended to include children ages 36 to 71 mo. Children with neurological damage, physical or behavioral problems, a diagnosis of a pervasive developmental disorder, or cerebral palsy (based on parent report) were excluded, as were any questionnaires with data missing for three or more items, date of birth, or sex. The final sample comprised 1,124 valid questionnaires (boys: 52.8%; northern Taiwan, n = 750; central Taiwan, n = 298; southern Taiwan, n = 76). Participants were divided into 6-mo age bands (Table 1).
Demographics and LDCDQ–TW Scores of the Community Sample (N = 1,124)
Note. LDCDQ–TW = Little Developmental Coordination Disorder Questionnaire–Taiwan.
Procedure
Directors of 14 kindergartens and eight nursery schools in Taiwan provided gatekeeper approval (northern Taiwan, n = 15; central Taiwan, n = 4; southern Taiwan, n = 3). With the directors’ consent, 1,500 questionnaires and informed consent forms were distributed to parents; 1,197 questionnaires were returned (response rate of 79.8%), with 73 questionnaires excluded, resulting in a sample size of 1,124. To assess the instrument’s test–rest reliability, parents or caregivers of 115 children from three kindergartens completed the LDCDQ–TW a second time, 2 wk after its initial completion. To examine interrater reliability, we randomly selected 7 kindergarten teachers to complete the LDCDQ–TW for 48 children. Data were collected between April and November 2010.
Data Analysis
A full data set was achieved for 11 items. Data were missing for four items (ranging from 0.09% to 1.2%) and were imputed using sample means. We used SPSS (Version 17.0) and LISREL (Version 8.54; Scientific Software International) software. A two-sided p of ≤.05 was considered statistically significant. Demographic data related to sex and age were analyzed using descriptive statistics. Two-way analyses of variance (ANOVAs) were used to explore the effects of sex, age, and their interaction (fixed factors) on the LDCDQ–TW Total score (dependent variable). Cronbach’s α coefficients were computed for the LDCDQ–TW and for each factor to examine internal consistency, with values >.70 considered acceptable (Portney, 2015). Test–retest and interrater reliability were calculated using two-way mixed-effects models of ICCs; values of >.75, .50–.75, and <.50 indicated good, moderate, and poor reliability, respectively (Portney & Watkins, 2000).
Results
Sex and Age Comparisons
A two-way ANOVA revealed that the interaction effect of sex and age was not significant, F(5, 1112) = 0.602, p = .698, but age, F(5, 1112) = 2.971, p = .011, and sex, F(1, 1112) = 5.312, p = .021, were. Girls (n = 530; M = 68.37 ± 9.61) had higher scores on the LDCDQ–TW than boys (n = 594; M = 67.08 ± 9.52), and older children scored higher than younger ones. Descriptive statistics for the LDCDQ–TW scores by age groups are shown in Table 1.
Internal Consistency
Cronbach’s α values were .95, .90, .92, and .86 for the LDCDQ–TW Total, CDM, FM, and GC scores, respectively, indicating good internal consistency. The corrected item–total correlations of the CDM, FM, and GC factors ranged from .65 to .82, .67 to .81, and .60 to .74, respectively (Table 2).
Item–Total Correlation Coefficients (N = 1,124)
Test–Retest Reliability
Good test–retest reliability was found for the LDCDQ–TW Total score (ICC = .97).
Interrater Reliability
Interrater reliability between the children’s (n = 48) teachers and parents was poor (ICC = .47). A paired-samples t test revealed statistically significant differences between parent (M = 69.31 ± 8.14) and teacher (M = 64.77 ± 13.75) ratings.
Phase 3: Validity of the LDCDQ–TW
In Phase 3, we evaluated the construct validity, discriminant validity, concurrent validity, and sensitivity and specificity of the LDCDQ–TW.
Method
Participants
Participants were recruited from the sample of 1,124 children from Phase 2. A total of 162 children participated in Phase 3.
Instruments
In addition to the LDCDQ–TW, the Movement Assessment Battery for Children (2nd ed., MABC–2; Henderson & Sugden, 2007) was used. This is a performance-based assessment for children ages 3–16 yr that addresses eight motor tasks in three categories: (1) Manual Dexterity, (2) Aiming and Catching, and (3) Balance. Test–retest reliability values ranged from .48 to .92, and interrater reliability values ranged from .52 to 1.00. The MABC–2 categorizes children according to their level of motor competence: Children who score above the 15th percentile are considered to have no movement difficulty, those who score between the 5th and 15th percentiles are considered at risk of having a movement difficulty, and those who score below the 5th percentile are considered to have considerable movement difficulty.
Procedure
Kindergarten and nursery school directors acted as gatekeepers. Children who scored at or below the 15th percentile on the LDCDQ–TW (n = 167) were invited for further motor testing by qualified occupational therapists at the child’s school; parents of 74 of the children agreed. Eighty-eight randomly selected typically developing children were also invited to complete the MABC–2. All participants (n = 162) were divided into three groups on the basis of their MABC–2 scores (regardless of LDCDQ–TW scores): DCD (≤5th percentile), suspect-DCD (5th–15th percentiles), non-DCD (>15th percentile).
Data Analysis
The original LDCDQ is based on a three-factor model, reflecting the three CDM, FM, and GC subscores. To explore construct validity, we conducted a confirmatory factor analysis (CFA) to determine whether the three-factor model applied to the LDCDQ–TW. We examined the χ2 goodness-of-fit (GOF) test statistic and GOF indices using LISREL 8.5: comparative fit index (CFI) and root mean square error of approximation (RMSEA). The values—CFI >.95 and RMSEA ≤.06—indicate good fit (Hu & Bentler, 1999).
We investigated discriminant validity using a one-way ANOVA, with Scheffé post hoc analyses (Scheffé, 1959), to compare the total LDCDQ–TW scores of the DCD, suspect-DCD, and non-DCD groups. To explore concurrent validity, we computed Pearson correlation coefficients to measure relationships between the LDCDQ–TW and MABC–2 Total scores, with values of 0–.30, .30–.70, and .70–1.0 indicating weak, moderate, and strong correlations, respectively (Saha & Paul, 2010).
Sensitivity refers to the proportion of children identified as scoring below the 15th percentile on the LDCDQ–TW who were also classified as having DCD or suspected DCD on the basis of MABC–2 scores below the 15th percentile. Specificity refers to the proportion of children identified by the LDCDQ–TW as having cause for concern yet not classified with motor problems because of MABC–2 scores above the 15th percentile. Desirable sensitivity and specificity values are 80% and 90%, respectively (American Psychiatric Association, 2013).
Results
Construct Validity
As shown in Figure 1 and Supplemental Table 1 (available online with this article at https://research.aota.org/ajot), the CFA of the 15-item LDCDQ yielded a model with three first-order factors and one second-order factor with good fit (CFI = 0.980, RMSEA = 0.056, χ2(76) = 342.563, p < .05). The measurement structure was slightly different from that of the original LDCDQ.
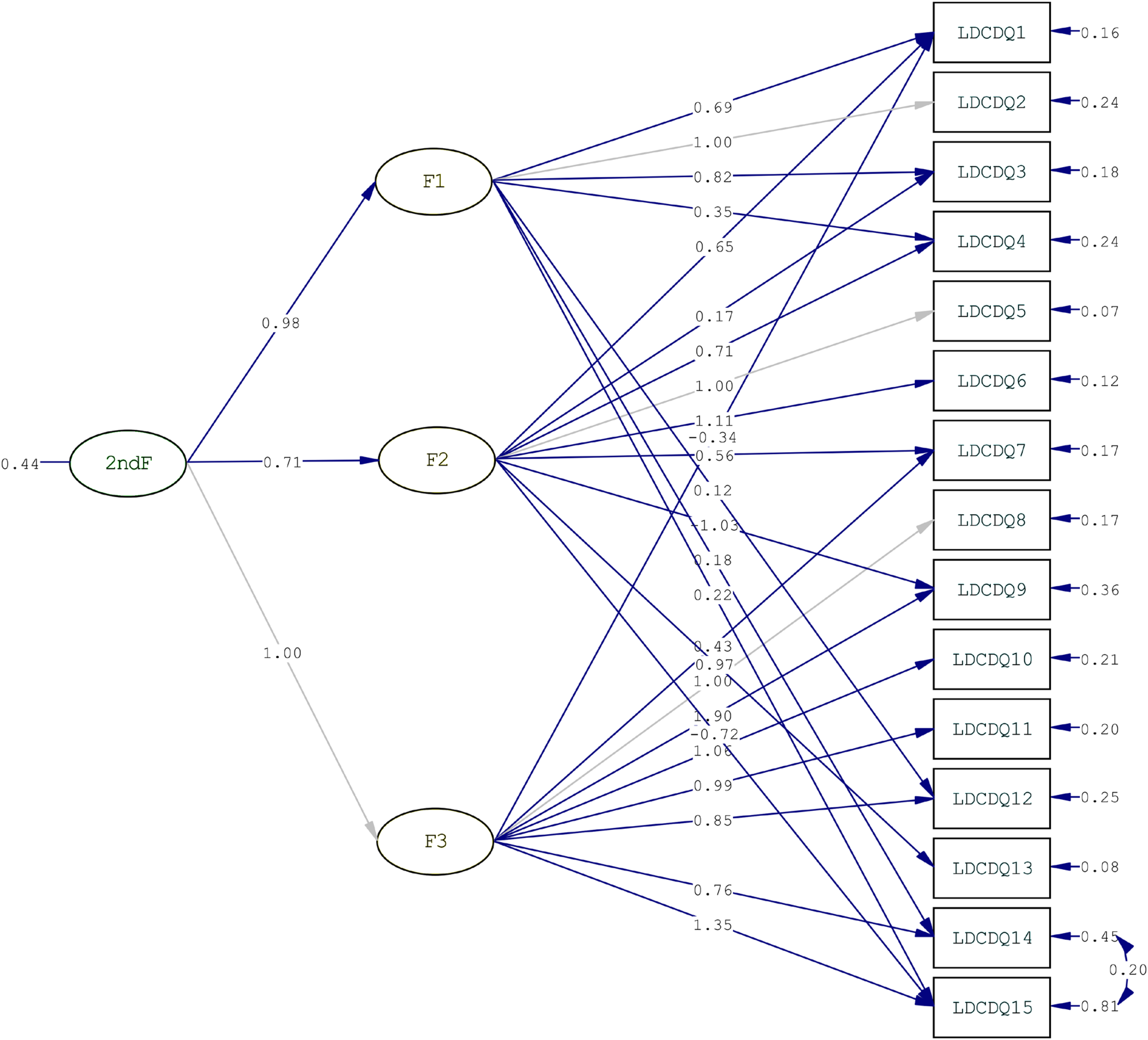
The final confirmatory factor analysis model of the LDCDQ–TW.
Discriminant Validity
Children were grouped on the basis of their MABC–2 scores (DCD, n = 28; suspect-DCD, n = 20; non-DCD, n = 114). Mean Total LDCDQ–TW scores of the DCD, suspect-DCD, and non-DCD groups were 50.57 (SD = 7.82), 48.25 (SD = 7.39), and 63.08 (SD = 12.44), respectively. One-way ANOVA revealed statistically significant group differences in total LDCDQ–TW scores, F(2, 159) = 24.41, p < .001, with post hoc Scheffé tests revealing that the non-DCD group scored notably higher than the DCD (p < .001) and suspect-DCD groups (p < .001), yet indicating no statistically significant differences between the DCD and suspect-DCD groups (p = .781, M difference = 2.32).
Concurrent Validity
The Total LDCDQ–TW scores showed a positive moderate correlation with the Total MABC–2 scores (n = 162, r = .52, p < .001).
Sensitivity and Specificity
The criterion for DCD in our study was a score below the 15th percentile on both the MABC–2 and the LDCDQ–TW (Tseng et al., 2010; Wilson et al., 2000). With this criterion, sensitivity was .96 and specificity was .68.
Discussion
In this study, the LDCDQ was translated into Mandarin Chinese and adapted for use with Taiwanese children following rigorous procedures. We then examined the psychometric properties of the LDCDQ–TW and observed sound validity, reliability, and sensitivity.
Although the instructions on all versions of the LDCDQ ask respondents to compare the child’s performance with that of other children of the same age and gender, implying that no age or gender differences would be expected, this study did indeed reveal differences among groups. This finding reflects those of an earlier study of younger children in Taiwan that revealed that parents perceive boys to be less coordinated than girls (Tseng et al., 2004) and is consistent with several studies that have used the Developmental Coordination Disorder Questionnaire with older children (Rivard et al., 2014). In contrast, Wilson et al. (2015) used the Canadian version of the LDCDQ, the LDCDQ–CA, with Canadian preschoolers and found that boys scored higher than girls. The sex differences in these studies, although statistically significant, were small (1–2 points).
Our findings indicate that older children scored significantly higher than younger children, a finding similar to that of Cantell et al. (2019), who used the Dutch version of the LDCDQ, the LDCDQ–NL. Some activities in the LDCDQ–TW are newly learned at age 3, and children’s performance may be influenced by subsequent practice. It is also possible that opportunities to practice the activities, as well as parental perceptions and expectations regarding competent performance, differ between cultures.
The internal consistency of the three factors was good to excellent (αs = .86–.92), similar to that found with the original Hebrew-language LDCDQ (αs = .84–.89; Rihtman et al., 2011). There were no negative or near-zero values of corrected item–total correlations, indicating that all LDCDQ–TW items contribute positively to factor scores and confirming homogeneity of items, consistent with other versions of the questionnaire (Wilson et al., 2015). CFA supported the original three-factor model of the LDCDQ (Rihtman et al., 2011) with Taiwanese preschoolers.
Although there was poor parent–teacher agreement on the LDCDQ–TW Total score (r = .45), this finding was not surprising because it is common across many assessments (Hartman et al., 2007) and may reflect observations of different types of behavior. Activities in which a child engages at home—often individually—are likely to differ from those expected at school in a group of peers. Interrater reliability is best assessed when all raters measure a response at the same time but independently (Portney, 2015). In this study, raters asynchronously observed different samples of behavior.
Consistent with the results of several other studies (e.g., Rihtman et al., 2011; Wilson et al., 2015), the LDCDQ–TW identified young children at risk of a later DCD diagnosis; however, it did not distinguish between those with more or less severe motor difficulties. Because the LDCDQ is an early screening tool used to identify children who require monitoring of motor development in relation to a diagnosis not usually given before age 5 yr (Blank et al., 2019), this is not a major concern and does not detract from the questionnaire’s intended use. As with many screening tools, further standardized performance-based assessments should be administered to confirm diagnoses and degrees of severity (American Psychiatric Association [APA], 2013).
The LDCDQ–TW showed statistically significant yet moderate correlations with the MABC–2 (r = .52), indicating that parent observations and professional assessments of children’s motor development are related (Wilson et al., 2000). However, other studies that have compared the LDCDQ and MABC–2 did not find relationships of this magnitude (r = .29; Venter et al., 2015; Wilson et al., 2015), suggesting that this is an area for monitoring as further versions of the LDCDQ are published.
Using the 15th percentile cutoffs of both the MABC–2 and the LDCDQ–TW, we noted that the latter’s specificity (68%) did not meet the preferred standard (APA, 2013), yet sensitivity (96%) did, indicating that children at risk of DCD are identified by the LDCDQ–TW with 96% accuracy. In this instance, given the importance of early identification, and because of the intended purpose of the LDCDQ–TW, higher sensitivity is preferred. Despite a false positive rate of 32%, it is crucial not to miss children with motor impairment who may subsequently develop social, emotional, and academic problems (Cairney et al., 2010).
This study has some limitations. Parent and teacher respondents may have had a limited understanding of movement development; however, we hope this concern was ameliorated through the instruction to compare the child with other children of the same age and sex. In addition, the questionnaire was designed for parents, so assuming similarities on the basis of teacher reports may be erroneous. Future interrater reliability studies should recruit informants from the same context, such as two different family members. Moreover, the relatively low specificity, which suggests a high rate of false positive identification, is a further limitation and is an important area to explore in further validation studies. Considering the intended use of the LDCDQ–TW (an inexpensive first-step screening), though, higher sensitivity could be claimed to be more important than higher specificity. The identification of children potentially at risk of DCD using the LDCDQ–TW as a first step, followed by a clinician-administered motor assessment, is recommended as part of a wider needs-identification process.
Implications for Occupational Therapy Practice
This study has several implications for occupational therapy practice: Early identification of children at risk of a later DCD diagnosis can facilitate early intervention, thus preventing secondary sequelae. Occupational therapy practitioners have a central role to play in the assessment and treatment of this clinical population. Our study demonstrates that the LDCDQ–TW is a valid and reliable tool to identify young children who may be at risk for a DCD diagnosis. The assessment thus has the potential to support the provision of timely intervention for young Taiwanese children with motor difficulties before secondary sequelae develop. The findings of our study contribute to a wider international collaborative effort to understand cultural influences on the motor development of young children. The LDCDQ is currently being standardized in more than 20 countries around the world following similar procedures. An initiative of this nature has implications for occupational therapy practice across all stages of the occupational therapy process.
Conclusion
The aims of this study were to translate and cross-culturally adapt the LDCDQ into Mandarin Chinese and evaluate its psychometric properties when used with Taiwanese preschoolers. Our findings revealed sound validity, reliability, and sensitivity and borderline specificity and parent–teacher agreement. The LDCDQ–TW can identify young Taiwanese children at risk of a DCD diagnosis and thus is a useful tool to support early identification and intervention.
Supplemental Material
Supplementary material for Psychometric Properties of the Little Developmental Coordination Disorder Questionnaire–Taiwan
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.047159.pdf for Psychometric Properties of the Little Developmental Coordination Disorder Questionnaire–Taiwan by Chung-Pei Fu, Mei-Hui Tseng, Sharon Cermak, Tzu-Han Chung, Yu-Lan Chen, Lu Lu, Jeng-Yi Shieh and Tanya Rihtman in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This study was supported through funding to Mei-Hui Tseng from the Department of Health, Executive Yuan, Taiwan (DOH92-TD-1035, DOH93-TD-M-113-038, and DOH94-TD-M-113-007). We gratefully appreciate Shula Parush for granting authorization to translate the LDCDQ into Mandarin Chinese. We also acknowledge Shih-Heng Sun from China Medical University for providing us the first draft of the LDCDQ–TW. We are also grateful to the directors and teachers of the nursery schools and kindergartens for their help with recruiting participants, as well as all the parents and children who participated in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.