
Abstract
This study demonstrates the utility of the Activity Measure for Post-Acute Care (AM-PAC) “6 Clicks” Daily Activity and Basic Mobility short forms in the discharge planning process to identify the next level of care for people who have had a stroke.
In standards of care guidelines, national associations recommend identification of the next level of care for the patient after acute stroke as a primary goal during acute hospitalization (Duncan et al., 2005; Winstein et al., 2016). In response to financial pressures to discharge patients from acute hospitalization quickly, length of stay (LOS) has been significantly reduced in the United States, with a national average LOS of 4.7 days for ischemic stroke (Benjamin et al., 2018). Because LOS in the acute care setting is short, determination of the next level of care needs to occur quickly, with an almost immediate discharge recommendation after initial assessment by the interdisciplinary team (Winstein et al., 2016). This recommendation has been shown to be extremely influential in the final discharge destination of the patient (Stein et al., 2020).
Prior work on determining discharge destination after acute stroke has highlighted the relationship among stroke severity, functional limitations, and discharge destination (Bohannon et al., 2002; Van der Cruyssen et al., 2015). People with more severe stroke have been shown to have more functional limitations and are more often discharged directly from acute hospitalization to inpatient rehabilitation settings rather than home (Winstein et al., 2016). Additional factors that affect discharge destination after stroke include patient preference, cognitive and perceptual ability, home and social support, and insurance coverage (Agarwal et al., 2015; Nguyen et al., 2015; Smith et al., 2017; Tanwir et al., 2014; Yeh et al., 2017). In the United States, patients can be discharged to two inpatient rehabilitation settings. In an acute inpatient rehabilitation facility (IRF), patients receive 3 hr of intensive therapy 6 days/wk for 2 to 4 wk. In subacute rehabilitation or a skilled nursing facility (SNF), patients receive less intensive therapy (1–2 hr for 5–7 days/wk) for longer stays. Patients discharged directly home from the acute care setting can receive therapy at home or attend outpatient therapy if needed (Winstein et al., 2016).
National guidelines also advocate the use of standardized assessments for the stroke population (Bland et al., 2015; Lang et al., 2011; Stein et al., 2015; Winstein et al., 2016). Standardized assessments during acute hospitalization for stroke can (1) assist in determining the plan of care by objectively measuring limitations in body structure and function as well as activities that affect the person’s ability to participate in home, social, or work life; (2) be useful in identifying the need for further inpatient rehabilitation services (Mees et al., 2016; Thorpe et al., 2018); and (3) direct rehabilitation intervention(s) and determine the efficacy of these interventions (McDonnell et al., 2018).
In the United States, neurologists use the National Institutes of Health Stroke Scale (NIHSS) as their standard measure to evaluate patients after stroke (Hov et al., 2019; Kasner, 2006). Although the rehabilitation field has numerous suitable outcome measures, they are not routinely used during acute stroke hospitalization (Jette et al., 2009; Van Peppen et al., 2008). The Activity Measure for Post-Acute Care (AM-PAC) “6 Clicks” Basic Mobility and Daily Activity short forms make up a standardized assessment tool that is gaining adoption in acute hospital settings because it is quick to administer and can be used with all patients regardless of diagnosis.
The 6 Clicks is an easily documented and succinct measure that encapsulates a patient’s basic mobility or performance in the acute care setting; in addition, it has been shown to be a clinically valid tool in identifying the need for further inpatient rehabilitation services (Jette et al., 2014a, 2014b). The 6 Clicks short forms have excellent test–retest reliability (intraclass correlation coefficient [ICC] = 0.96–0.97) and interrater reliability (ICC = 0.90–0.92; Jette et al., 2015). The initial 6 Clicks scaled scores of 42.9 for Basic Mobility and 39.4 for Daily Activity were determined to be the cutoff scores that predicted a home discharge. A lower initial score predicted discharge to an inpatient rehabilitation setting. These cutoff scores were identified in a mixed patient population in which only 12.8% of the population had a primary neurological diagnosis.
Thus, it is necessary to determine whether these values are applicable in the stroke population, in which recovery from neurological impairments may proceed at a slower rate than recovery from other medical conditions. Therefore, we examined the utility of the 6 Clicks Basic Mobility and Daily Activity short forms in determining discharge destination for people admitted to the hospital for an acute stroke. The purpose of our study was to determine whether 6 Clicks scores could assist in identifying the discharge destinations (home with or without services, IRF, or SNF) for people admitted to a stroke service in a large metropolitan teaching hospital.
Method
Participants and Procedures
In this cohort study, a retrospective data analysis was conducted using the New York-Presbyterian Hospital’s electronic medical records (EMRs). Data were extracted for all patients admitted to the stroke service in 2015 and 2016. Data were included if patients received a physical therapy or occupational therapy evaluation, had a 6 Clicks Basic Mobility or Daily Activity score at initial evaluation, and were discharged to one of three destinations: home, IRF, or SNF.
The 6 Clicks Basic Mobility short form was completed by physical therapists and included six items: rolling without bedrail, supine to sit, sit to stand, bed to chair, walking in the hospital room, and climbing a few stairs. The 6 Clicks Daily Activity scale was completed by occupational therapists and included six items of self-care: bathing, upper body dressing, lower body dressing, toileting, eating, and grooming. All items on the 6 Clicks are scored on a 4-point ordinal scale ranging from 1 (total assistance) to 4 (no assistance needed at all) on the basis of the amount of assistance needed for each item. Both short forms were completed on the basis of the original guidelines from the creators of the 6 Clicks at Massachusetts General Hospital (Jette et al., 2014b). Scores for the six items of the Basic Mobility and Daily Activity short forms were used to compute total raw and scaled scores for each short form. As stated earlier, the home discharge cutoff scores for a mixed medical–surgical population were 42.9 and 39.4 for Basic Mobility and Daily Activity, respectively. Minimal detectable change scores were 4.72 for Basic Mobility and 5.49 for Daily Activity (Jette et al., 2014a). Scaled scores were used in this study to mirror the original article by Jette et al. (2014a), which also investigated discharge destination in relation to AM-PAC “6 Clicks” scores. In addition, a scaled score was recommended for use in research because the 6 Clicks was originally designed to be used and compared across settings with the scaled scores by the creators of the measure (Jette et al., 2014b).
This study was approved by the Columbia University institutional review board. To ensure data accuracy, we manually confirmed both actual discharge destination and stroke diagnosis. Stroke diagnosis was specifically confirmed through a thorough chart review and comparison with neurology admission and follow-up notes. Of the 816 patients admitted to the stroke service, 112 were excluded because they (1) did not have a confirmed stroke; (2) died during hospitalization; (3) signed out against medical advice; or (4) were discharged to hospice or some other facility that was not home, IRF, or SNF. After exclusion, 704 patients remained in the final data set for analysis.
Outcomes
Demographic data collected included age, gender, hospital LOS, initial NIHSS score, and type of stroke (ischemic, hemorrhagic, or subarachnoid hemorrhage). Initial NIHSS scores were missing for 37% of patients in our data set. Independent variables included the initial scaled 6 Clicks scores for Daily Activity (6 Clicks Daily Activity) and Basic Mobility (6 Clicks Basic Mobility
Data Analysis
We conducted all data analyses using IBM SPSS Statistics (Version 26). No significant differences were found for age or LOS between 2015 and 2016; therefore, the data were collapsed across the 2 yr. Data were stratified by discharge destination, and descriptive statistics were calculated for all variables. One-way analyses of variance (ANOVAs) with Tukey’s honestly significant difference (HSD) post hoc comparisons were performed to analyze discharge destination by age and LOS; both of these variables are frequently reported in the literature and are of clinical importance in the hospital. Subsequently, one-way ANOVAs with Tukey HSD post hoc comparisons were conducted to examine differences in initial 6 Clicks Basic Mobility and Daily Activity scores by discharge destination (home, IRF, or SNF). In these analyses, we included age as a covariate to ensure that the effect observed was not confounded by age. A one-way ANOVA was also conducted to examine differences in discharge destination by NIHSS score because severity of stroke has been shown to affect functional status, and we sought to confirm this observation with our data set.
Receiver operating characteristic (ROC) curves were calculated for each 6 Clicks data set (Basic Mobility and Daily Activity scores) to determine the percentage of the variance explained by initial 6 Clicks scores in determining discharge destination. Curves were first obtained for the comparison between patients who were discharged to home and those who required any further rehabilitation services (IRF and SNF combined). A second set of ROC curves was then obtained to compare those patients discharged to IRF with those who were discharged to SNF for both 6 Clicks Basic Mobility and Daily Activity scores. ROC curves were used to select cutoff values for home versus further rehabilitation and for IRF versus SNF. Sensitivity, specificity, and positive and negative predictive values were calculated for the cutoff scores.
Results
Table 1 shows the data for age and gender by type of stroke. Our sample was composed of 51.21% women (M age range = 60.72–69.02 yr). Overall, 83.24% of patients had an ischemic stroke, 13.21% had a hemorrhagic stroke, and 3.55% had a subarachnoid hemorrhage stroke.
Demographic Characteristics of the Patients Who Had a Stroke
Note. NIHSS = National Institutes of Health Stroke Scale; SAH = subarachnoid hemorrhage.
A total of 259 patient records were missing an initial NIHSS score and thus could not be included.
Patients discharged to home or IRF were younger than those discharged to SNF (Table 2). A statistically significant main effect for age was seen, F(2, 701) = 27.19, p ≤ .0001, with pairwise comparisons yielding differences between SNF and home (p < .0001) and SNF and IRF (p < .0001). LOS was significantly different statistically across the three discharge destinations, F(2, 701) = 38.80, p < .0001. LOS was shortest for patients discharged to home and longest for those discharged to SNF (see Table 2; p < .05 for all comparisons).
Comparison of Age, LOS, and “6 Clicks” Basic Mobility and Daily Activity Scaled Scores by Discharge Destination
Note. Number of patients in each category is lower than the total because not every patient received both therapies or had an initial score recorded. CI = confidence interval; IRF = inpatient rehabilitation facility; LOS = length of stay; SNF = skilled nursing facility.
Statistically significant differences were seen for NIHSS scores among all three discharge destinations, F(2, 441) = 40.13, p < .0001. Patients discharged to home had the lowest mean NIHSS scores (M = 3.45, SD = 4.10)). Patients discharged to IRF had a lower average score (M = 7.57, SD = 6.77) than those discharged to SNF (M = 9.51, SD = 7.24; p = .0001). Scores for patients going home were lower than scores for patients who were discharged to IRF or SNF (p < .35).
A statistically significant difference was seen for 6 Clicks Basic Mobility scores by discharge destination, F(2, 639) = 143.46, p < .0001. Patients discharged to home had a higher initial 6 Clicks Basic Mobility score than those who were discharged to IRF (see Table 2). In addition, patients discharged to IRF had higher scores than those discharged to SNF (see Table 2). Statistically significant differences were seen among all three discharge destinations (p < .001) for initial Basic Mobility, with no overlap in the 95% confidence intervals between home and IRF and between IRF and SNF.
Similar results were observed for the initial 6 Clicks Daily Activity scores (see Table 2), with a main effect for discharge destination, F(2, 649) = 131.77, p < .0001. Patients discharged to home had a higher 6 Clicks Daily Activity score than those discharged to IRF, and these patients had higher scores than those discharged to SNF (see Table 2; p < .001 for all comparisons). In addition, no overlap in the 95% confidence intervals was noted among all three groups.
ROC results for both 6 Clicks Basic Mobility and Daily Activity scores were able to distinguish between home versus further inpatient rehabilitation, with close to acceptable levels for IRF versus SNF. Table 3 shows that the area under the curve (AUC) for the 6 Clicks Basic Mobility scores was .82 for distinguishing discharge home versus further inpatient rehabilitation settings (Figure 1A) and .64 for distinguishing between IRF and SNF (Figure 1B). Equivalent results were obtained for Daily Activity scores, with AUCs of .82 and .67 (Figures 1C and 1D, respectively).
“6 Clicks” Scaled Score Cutoff Values for Home Versus Any Further Rehab and IRF Versus SNF
Note. AUC = area under the curve; IRF = acute inpatient rehabilitation facility; NLR = negative likelihood ratio; NPV = negative predictive value; PLR = positive likelihood ratio; PPV = positive predictive value; Rehab = inpatient rehabilitation; SNF = subacute skilled nursing facility.
aFrom Jette et al. (2014a).
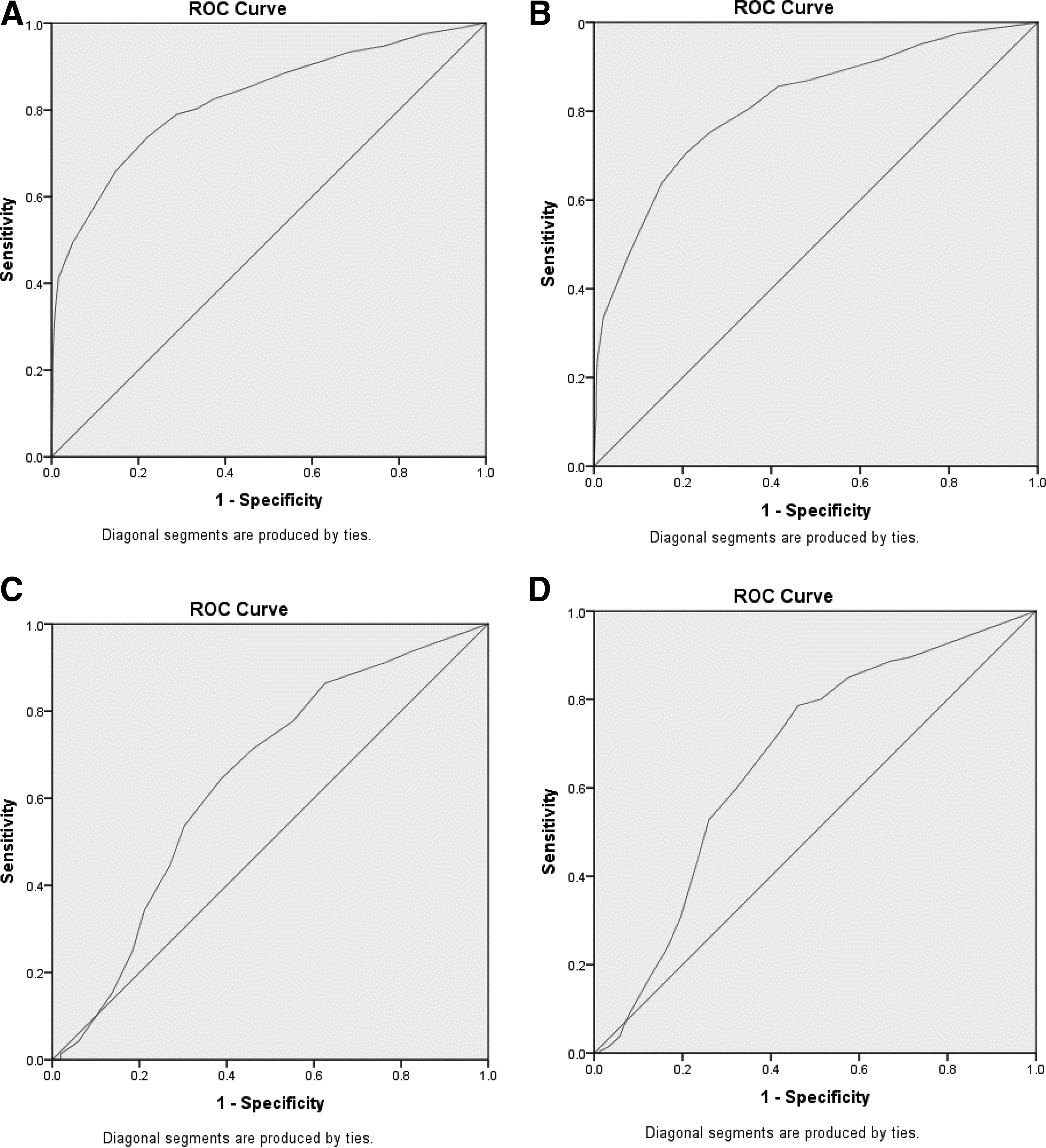
ROC curves for 6 Clicks Basic Mobility (Panels A and C) and Daily Activity (Panels B and D) short forms.
Cutoff scores were selected on the basis of high specificity in all four cases (home vs. rehabilitation and IRF vs. SNF for both Basic Mobility and Daily Activity). Specificity was chosen to err on the side of caution and to avoid decisions that sent patients home unsafely. High specificity ensures that patients who might be unsafe for discharge home are discharged to inpatient rehabilitation. As can be seen in Table 3, a score of 44.50 for Basic Mobility enabled discrimination between need versus no need for further inpatient rehabilitation services with a high degree of specificity. A Daily Activity score of 39.40 yielded similar results in discriminating between need versus no need for further inpatient rehabilitation services. Cutoff scores of 34.59 for Basic Mobility (specificity/sensitivity: 0.63/0.63) and 31.32 for Daily Activity (specificity/ sensitivity: 0.68/0.59) were used to distinguish discharge to IRF versus SNF. Table 3 also identifies the predictive values and likelihood ratios for Basic Mobility and Daily Activity scores. The positive predictive values for home were 89.88% for Basic Mobility scores and 85.88% for Daily Activity scores. For IRF versus SNF, they were 71.68% and 72.67% for Mobility and Daily Activity scores, respectively. The positive likelihood ratios for home versus further rehabilitation were 9.34 and 6.04 for Basic Mobility and Daily Activity scores, respectively. For IRF versus SNF, they were 1.68 and 1.84.
Discussion
The primary aim of our study was to examine the utility of the 6 Clicks in a stroke population to identify discharge destination early in the rehabilitative process. Our findings support the use of the 6 Clicks Basic Mobility and Daily Activity short forms for assessment of functional status and to assist with early discharge planning for the stroke population. The initial 6 Clicks scores from our data set were able to identify eventual discharge to all three destinations. Distinctions across the three discharge destinations have not been previously reported (Bland et al., 2015; Covert et al., 2020 ; Stein et al., 2015).
Our population’s Daily Activity cutoff score for home was similar to that reported by Jette et al. (2014b). However, the Basic Mobility cutoff score for discharge to home in our population was higher than the score reported for the mixed medical–surgical population (Jette et al., 2014b). When identifying cutoff scores, we maximized specificity rather than sensitivity values. Given the increased incidence of falls in the stroke population, erring on the side of better mobility appears to be critical for a safe home discharge in this patient population. Greater specificity resulted in a higher positive predictive value for both Basic Mobility and Daily Activity scores compared with the mixed population.
Although our results demonstrated that NIHSS scores were different for all three discharge destinations, the NIHSS should not be used in isolation to identify the need for further rehabilitation services. Occupational and physical therapists in the acute care setting generally do not use the NIHSS scale. It does not include information about a patient’s functional limitations, which is essential to develop a plan of care for communication with potential IRFs and for insurance reimbursement. Covert et al. (2020) found that NIHSS scores in combination with 6 Clicks Basic Mobility scores were predictive for distinguishing home versus further inpatient rehabilitation. However, Covert et al. (2020) did not examine 6 Clicks Daily Activity scores. We found that either the Daily Activity or the Basic Mobility score could accurately predict discharge destination. Because the NIHSS is primarily used by neurologists, using the NIHSS score in combination with 6 Clicks Daily Activity and Basic Mobility scores may improve predictive power and encourage an interdisciplinary approach to discharge planning.
Patients discharged to SNF were older than those discharged to IRF or home. Older adults with stroke have been shown to have reduced mobility levels, which limit their tolerance for a more intensive rehabilitation setting (Stein et al., 2015). In addition, the number or severity of comorbid conditions seen in older adults may also contribute to lower function (Yeh et al., 2017). The lower 6 Click scores seen in our data may indicate preexisting functional limitations or comorbid conditions before hospital admission. Because this topic was beyond the scope of our study, we cannot further elucidate the function–comorbidity– age relationships.
The LOS for patients discharged to IRF was significantly longer than for those discharged to home, and LOS for those going to SNF was the longest. Longer LOSs might be explained by greater medical complexity of the patients admitted, more comorbid conditions, or the insurance approval process. Further investigation is needed to elucidate the reasons for LOS differences in patients discharged to different inpatient rehabilitation destinations.
We recognize that additional factors may play a role in determining discharge destination. These factors include social situation, cognitive status, comorbid conditions, age, prior functional level, insurance status, bed availability, and existence of referral relationships between facilities (Mees et al., 2016; Nguyen et al., 2015; Rakesh et al., 2019; Smith et al., 2017; Stein et al., 2015; Tanwir et al., 2014; Van der Cruyssen et al., 2015). Ultimately, multifactorial models attempting to distinguish among the three discharge destinations for the acute stroke population should include the aforementioned factors with initial 6 Clicks Basic Mobility and Daily Activity scores. We advocate occupational and physical therapists’ use of the initial 6 Clicks scores as a first step in the discharge destination decision tree to guide a clinician’s decision-making process.
Using the initial 6 Clicks Basic Mobility and Daily Activity scores to determine ultimate discharge destination for a patient does not necessarily provide any information about whether that actual discharge destination was optimal for the patient. This determination would require long-term follow-up and measurement of patient outcomes after completion of their rehabilitation course, which was beyond the scope of our study.
We recognize that our investigation is not unique in attempting to determine discharge destination after acute stroke. What makes our investigation unique is the choice of tool (6 Clicks) and the fact that as part of routine patient care at our hospital, occupational and physical therapists document the scores in the EMR for each patient encounter. The outcomes examined in Thorpe et al.’s 2018 systematic review determining discharge to home versus institution after acute stroke were not easy to use or ideal for our acute setting. In our study, we specifically focused on the earliest possible determination of discharge destination during acute hospitalization after stroke. AM-PAC 6 Clicks scores are functional scales that can be used across all patients, are administered as part of routine care by occupational and physical therapists, and are easy to use.
Limitations
Our study limitations include that (1) a small sample size was used in comparison with prior work on 6 Clicks short forms (Jette et al., 2014a); (2) the study was conducted at one metropolitan hospital location, where discharge destination may have been influenced by environmental factors (e.g., presence of stairs, absence of elevator access, smaller living quarters, and heavier reliance on walking and public transportation for travel); (3) patients either too low or too high functioning may have been excluded from our data set because they were not evaluated by either physical or occupational therapy; (4) the use of scaled rather than raw scores for the AM-PAC 6 Clicks created the possibility of measurement error; and (5) the study lacked long-term follow-up and information about optimal discharge for individual patients. This study was the first step to examine whether the 6 Clicks, which is routinely used by occupational and physical therapists, can be useful in care planning. An important next step will be to prospectively examine whether patients were indeed optimally placed.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: The 6 Clicks Basic Mobility and Daily Activity short forms are valid and easily integrated into clinical practice. Both initial 6 Clicks Daily Activity and Basic Mobility scores can assist in determining discharge destination.
Conclusion
Our results highlight the utility of the initial 6 Clicks Basic Mobility and Daily Activity short forms as a valuable functional tool to use in early discharge planning. We were able to determine cutoff values from the initial scaled scores for home versus further inpatient rehabilitation settings. We were also able to differentiate between and provide cutoff values for patients who were discharged to IRF or SNF. The use of standardized assessments is an essential component of care in the rehabilitation setting even during acute hospitalization after stroke. Because the 6 Clicks is an easy-to-use functional measure that encompasses many facets of a patient’s functional status, its use and interpretation on the first therapy visit should be encouraged and may enable faster discharge destination decision making. Future work should examine the utility of the 6 Clicks with a larger and more heterogeneous population of patients from multiple stroke care centers and should include 6 Clicks scores in a multifactorial analysis to assist in predicting discharge destination.
Footnotes
Acknowledgments
This article was previously presented as a poster at the Combined Sections Meeting of the American Physical Therapy Association, January 23–26, 2019, Washington, DC.