
Abstract
This scoping review summarizes the existing literature on CIMT for infants with hemiplegic CP.
Cerebral palsy (CP) is the most common physical disability of childhood, occurring in 1 in 323 children in the United States (Centers for Disease Control and Prevention, 2020). Historically, doctors gave a diagnosis of CP no earlier than the second year of life (Maitre et al., 2020; Novak et al., 2017; Sakzewski et al., 2019; Vitrikas et al., 2020). However, guidelines for early detection and accurate diagnosis of CP (Novak et al., 2017) have created a growing interest in determining the efficacy of interventions for infants with a diagnosis of CP and infants at high risk for CP.
These guidelines propose that a diagnosis of CP or being at high risk for CP can be determined before age 1 yr (Novak et al., 2017). Novak et al. (2017) suggested that early diagnosis should lead infants with CP or at high risk for CP to appropriate interventions that improve functional outcomes. It has been reported that children with CP achieve 90% of their motor progress by age 5 yr (Morgan et al., 2016; Vitrikas et al., 2020). However, the majority of their progress is made during the first 2 yr of life (Morgan et al., 2016). Early diagnosis is essential to initiate motor-based intervention and maximize an infant’s potential.
Constraint-induced movement therapy (CIMT) is a popular therapeutic approach used to treat children with hemiplegic CP. CIMT is an intervention that restricts the nonaffected upper extremity to increase functional use of the affected upper extremity. The current body of literature speaks to efficacy among children older than age 2 yr (Chamudot et al., 2018).
Constraint-Induced Movement Therapy and Early Intervention
For children with hemiplegic CP, CIMT has been proven to be an effective intervention approach. In a systematic review, Chiu and Ada (2016) found that CIMT was more effective than no intervention at improving the use of the affected hand. In a more extensive systematic review, Hoare et al. (2019) reinforced Chiu and Ada’s findings while also suggesting that CIMT is more effective than a low-dose comparison group, such as usual care or bimanual therapy. However, these findings cannot be generalized to the infant population because the randomized controlled trials (RCTs) reviewed in these studies included infants as part of a broad age range rather than looking at that specific age group.
In a systematic review, Morgan et al. (2016) found weak evidence to support motor interventions, including CIMT, for infants with CP. Similarly, Novak et al. (2020) determined that motor learning training–based interventions, such as baby–CIMT, baby–bimanual, and Goals–Activities–Motor Enrichment (GAME), are emerging interventions that collectively show promising evidence. More research is needed to determine the clinical efficacy of these infant motor interventions and, in particular, the efficacy of CIMT. To date, no studies have summarized research findings specific to CIMT for the infant population. As such, the purpose of this scoping review is to explore the existing evidence related to CIMT for infants with CP or at high risk for CP.
Method
The framework of Arksey and O’Malley (2005), later expanded on by Levac et al. (2010), was used to guide the methodology of this scoping review on infant CIMT. Arksey and O’Malley proposed five stages: (1) identify a research question, (2) identify relevant studies, (3) select studies, (4) chart the data, and (5) summarize the results.
Identifying Research Questions
The following research question directed this scoping review: “Does research show that it is feasible to implement a CIMT protocol for infants age 2 yr and younger with a diagnosis of CP or at high risk for CP?” In this scoping review, we consolidate available information regarding infant CIMT protocols and explore initial findings for this emerging area of practice.
Identifying Studies
The following databases were searched in August 2020: PubMed, CINAHL, Cochrane, and ProQuest. Key terms—such as infant constraint-induced movement therapy, infant CIMT, baby constraint induced movement therapy, and baby CIMT—were used. When possible, searches were filtered by the infant option under the age category to reduce the number of articles that included older children. Hand searching was also completed.
Selecting Studies
Only studies that looked explicitly at CIMT for infants at risk for hemiplegic CP or with a diagnosis of hemiplegic CP were selected for review. For this scoping review, infants are defined as children age 24 mo or younger. Additionally, studies were considered if they were published in English between 2000 and 2020, were peer-reviewed, and addressed changes in upper limb function of the hemiplegic upper limb. Articles that looked at other CP motor interventions, such as baby–bimanual, GAME, and small steps, were excluded. Studies with infants diagnosed with other types of CP (e.g., quadriplegic CP) were excluded. Nine articles were selected from abstract review. One study did not present clear information about the infant CIMT protocol and was excluded (Bollea et al., 2007). Figure 1 presents the study selection process. Ultimately, 8 articles that met these criteria were included in this review.
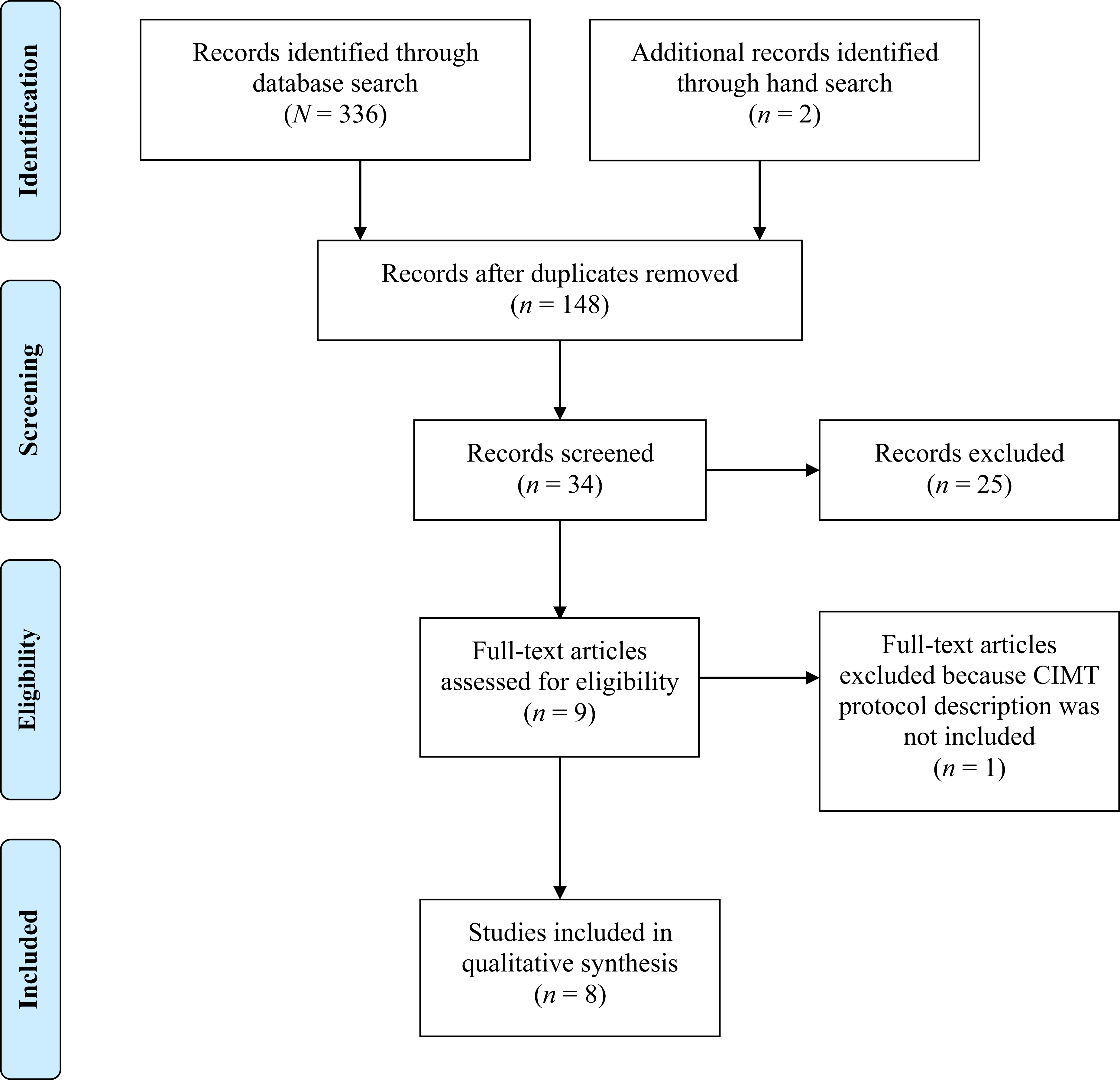
Flow diagram for inclusion and exclusion of peer-reviewed studies in the scoping review.
Charting Data
Information about the 8 studies can be found in Table A.1 in the Supplemental Appendix, available online with this article at https://research.aota.org/ajot. Established guidelines from the American Occupational Therapy Association (AOTA; 2020) and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Moher et al., 2009) were used to present the information about the 8 studies included in this review. Table 1 shows additional information about each study protocol. Two separate risk-of-bias tables were created. Table A.2 categorizes RCTs, whereas Table A.3 categorizes Level 3 studies and below. We evaluated levels of evidence using the Oxford Levels of Evidence (Oxford Centre for Evidence-Based Medicine [OCEBM] Levels of Evidence Working Group, 2011).
Infant CIMT Protocols
Note. CIMT = constraint-induced movement therapy; NS = not specified.
Results
The 8 articles included the following study designs: RCT (n = 2; Chamudot et al., 2018; Eliasson et al., 2018), retrospective cohort design (n = 1; Nordstrand et al., 2015), pretest–posttest study (n = 1; Lowes et al., 2014), single-subject study (n = 2; Coker et al., 2009; Cope et al., 2008), and case study (n = 2; Fergus et al., 2008; Reidy et al., 2017). Two of the researchers for Nordstrand et al. (2015; Nordstrand and Eliasson) were also involved in the RCT by Eliasson et al. (2018). However, studies did not involve the same participants. Overall, the collection of articles had a low risk of bias (see Tables A.2 and A.3), with the exception of the case study by Fergus et al. (2008), which had a moderate risk of bias.
Infant Constraint-Induced Movement Therapy Protocols
Dosage
The 8 studies described a range for protocol intensity, frequency, and duration (see Table 1). Two studies followed a protocol known as baby–CIMT with an intensity of 30 min per day over a duration of two 6-wk periods with a 6-wk break in between (Eliasson et al., 2018; Nordstrand et al., 2015). However, the frequency for both studies differed. Eliasson et al. (2018) had a frequency of 6 days per week, whereas Nordstrand et al. (2015) reported a frequency of 7 days per week.
Among the remaining 6 studies, intensity ranged from 1 hr per day (Chamudot et al., 2018) to 6 hr per day (Fergus et al., 2008); frequency ranged from 5 days per week (Lowes et al., 2014; Reidy et al., 2017) to 7 days per week (Chamudot et al., 2018; Coker et al., 2009); and duration ranged from 2 wk (Cope et al., 2008) to 8 wk (Chamudot et al., 2018).
Three protocols allowed the intensity to be separated into smaller increments during the day (Chamudot et al., 2018; Cope et al., 2008 ; Eliasson et al., 2018). It is important to note that even though participants in the studies by Cope et al. (2008) and Lowes et al. (2014) wore a nonremovable cast 24 hr per day, 7 days per week, CIMT theoretical principles were confined to the prescribed dosage established by each protocol. Additionally, Fergus et al.’s (2008) study had a high intensity, but it also included time spent doing less structured activities.
Constraints
A variety of constraints were used across all CIMT protocols. The most common were gentle restraints, such as mitts or gloves, which were used in 4 studies (Chamudot et al., 2018; Eliasson et al., 2018; Fergus et al., 2008; Nordstrand et al., 2015). Fergus et al. (2008) reported that gentle restraints blocked fine motor use of the nonaffected hand but allowed for gross motor movements, postural reactions, and protective responses. Only 1 study used a resting hand splint covered by a soft mitt (Coker et al., 2009). Three studies used casts: a nonremovable cast (Cope et al., 2008; Lowes et al., 2014) or a removable cast (Reidy et al., 2017). No adverse effects were observed in the nonaffected upper limb when a nonremovable cast was used and worn 24 hr a day, 7 days per week, during the CIMT protocol (Cope et al., 2008; Lowes et al., 2014).
Intervention Administration
CIMT protocols were administered in different environments and by various interventionists. The home environment allows the infant to learn new skills in their natural environment with their caregivers, allowing for easy generalizability of new skills in their everyday life (Lowes et al., 2014). All 8 articles included the home environment as the primary setting (Chamudot et al., 2018; Coker et al., 2009; Cope et al., 2008; Eliasson et al., 2018; Fergus et al., 2008; Lowes et al., 2014; Nordstrand et al., 2015; Reidy et al., 2017). Two of the 8 studies also provided CIMT treatment in the clinic setting for a combined setting approach (Coker et al., 2009; Reidy et al., 2017).
Seven studies included parents as the primary or one of the primary interventionists (Chamudot et al., 2018; Coker et al., 2009; Eliasson et al., 2018; Fergus et al., 2008; Lowes et al., 2014; Nordstrand et al., 2015; Reidy et al., 2017). Therapists were included as additional interventionists in 3 studies (Coker et al., 2009; Lowes et al., 2014; Reidy et al., 2017). Only Cope et al. (2008) had occupational therapists and physical therapists as the primary interventionists without tracking or formally prescribing parent involvement during the CIMT intervention period.
Parent Training
Parent training appears to be a vital component of the infant CIMT protocols presented in this scoping review. Seven articles included some form of direct parent training or specific home program (Chamudot et al., 2018; Coker et al., 2009; Eliasson et al., 2018; Fergus et al., 2008; Lowes et al., 2014; Nordstrand et al., 2015; Reidy et al., 2017). Parent training sessions were conducted either in the home or in the clinic. These sessions enabled therapists to monitor changes and guide parents on activities to be completed in subsequent sessions. Therapists reviewed motor learning principles, including task practice, repetition, and shaping (Chamudot et al., 2018; Lowes et al., 2014). Therapists also trained parents in activity staging and the use of positive reinforcement (Fergus et al., 2008). Home programs were individualized.
Objective Outcome Measures
Objective outcome measures that showed a change in hand use of the affected extremity varied. Developmental assessments, such as the Peabody Developmental Motor Scales–2 (PDMS–2; Coker et al., 2009; Cope et al., 2008) and the Bayley Scales of Infant and Toddler Development–Third Edition (BSID–3; Lowes et al., 2014), were used for their fine motor component. Video analyses were common in lower level studies. Video analysis, although nonstandardized, allowed researchers to look at the percentage of hand use for specific motor actions of the affected side (Coker et al., 2009; Fergus et al., 2008).
Assessments that examined upper limb movement and function for children included the Quality of Upper Extremity Skills Test (QUEST; Reidy et al., 2017), the Mini-Assisting Hand Assessment (Mini-AHA; Chamudot et al., 2018; Reidy et al., 2017), and the Hand Assessment for Infants (HAI; Eliasson et al., 2018). These were all designed specifically for the hemiplegic CP population. All outcome measures used in the eight studies showed either significant findings or positive clinical findings to support the use of CIMT for infants with CP or at high risk for CP.
Discussion
The primary objective of this scoping review was to synthesize research on infant CIMT. A total of 8 studies were included in this scoping review, from case studies to lower quality RCTs. The evidence provided by this scoping review has moderate strength because of the small number of studies included, low level of study design, and overall small sample size in most studies (AOTA, 2020). Nevertheless, this review provides preliminary support for an infant CIMT protocol and provides information that can guide future practice. Higher level studies are needed to make clinical recommendations as to the efficacy of CIMT for the infant population.
This scoping review highlights the wide variety of protocol designs and appropriate outcome measures found in the published studies. The lack of consensus in protocol design is also found in research for older children with CP who receive CIMT (Hoare et al., 2019). Research has shown that early intervention and disability-specific interventions are critical for infants age 2 yr and younger (Morgan et al., 2016; Vitrikas et al., 2020). Researchers may consider determining a minimum dose and a standard dose to get the greatest gains from infant CIMT. More important, future research may also investigate the ideal age at which to begin intervention to avoid learned nonuse or developmental disregard, a phenomenon that occurs when a child’s limited motor abilities lead to a decrease in spontaneous use and functional use of the upper extremity (Chamudot et al., 2018; Cope et al., 2008; Fergus et al., 2008).
Information is limited regarding the most appropriate form of constraint for infants. Studies in this scoping review used soft restraints and casts, both removable and nonremovable. Soft restraints were most commonly used. Fergus et al. (2008) found a mitt to be less restrictive and most safe for the infant. Eliasson et al. (2018) and Chamudot et al. (2018) reported that the soft restraints were well tolerated by the infants in their respective studies. No study was found that looked at the efficacy of different types of constraints during a CIMT protocol. This area should also be examined further to determine the most efficacious constraint for the infant population that promotes skill acquisition while minimizing both infant and parent frustration.
Early intervention services are typically provided at home, so it is not surprising that all 8 studies conducted their CIMT protocol primarily in the home environment. Lowes et al. (2014) found that home-based services (1) take into consideration a family’s personal culture, (2) offer a more comfortable setting, (3) support carryover outside of the prescribed intervention time with the infant’s toys, and (4) make it easy for the infant to generalize the newly acquired skills.
The CIMT protocols presented in this scoping review implement coaching strategies. Foster et al. (2013) stated that the goal of coaching is to “increase knowledge, skills, and competence of a client to enable participation in the context of the family’s daily life” (p. 254). Therapists take on the role of educator and facilitator. Therefore, parent participation through home programs, parent education, and parent training is also important to infant CIMT. In most studies, parents were educated on the principles of motor control and motor learning (Chamudot et al., 2018; Eliasson et al., 2018; Fergus et al., 2008; Lowes et al., 2014; Nordstrand et al., 2015). In the short term, this knowledge may have a positive impact on affected hand use during this critical neuroplastic stage if families continue to implement these strategies beyond prescribed treatment. Chamudot et al. (2018) suggested that parent training enables caregivers to integrate CIMT principles into the infant’s daily activities. Moreover, this knowledge is likely to be incorporated into daily routines and play interactions outside of the time frame of CIMT, and it may influence the functional development of the affected upper extremity among infants as they enter childhood.
In terms of outcome assessments, the HAI and the Mini-AHA are the most appropriate outcome measures to determine the effectiveness of an infant CIMT protocol because they are designed for this specific population and look at both unimanual skills and bimanual skills. The HAI was designed for infants ages 3 to 12 mo at risk for CP, and it assesses how the infant uses their hands together and separately (Krumlinde-Sundholm et al., 2017). The Mini-AHA, the infant version of the AHA, was designed for infants ages 8 to 18 mo and also looks at hand use separately and together (Chamudot et al., 2018). Both assessments are relatively new and were thus not commonly used in the studies included in this scoping review. Both assessments require administrators to complete extensive training for certification. Other CP-specific tests, such as the QUEST, need to be modified because they are not designed for the infant population (Reidy et al., 2017); thus, their validity for use with this population is affected. Developmental tests such as the PDMS–2 and the BSID–3 are designed to track fine motor development and are not comprehensive hand use assessments. A passing score can be achieved by using the nonaffected extremity without regard to the affected extremity. Therefore, these assessments are not sensitive to detect changes in hand use. However, Cope et al. (2008) attempted to solve this issue by administering the PDMS–2 twice, with both the nonaffected and the affected hand.
Limitations
This scoping review is not without its own limitations. By design, a scoping review includes lower level studies (Arksey & O’Malley, 2005; Levac et al., 2010). Half of the articles had Level 4 and Level 5 evidence. Because of the limited research in this area of practice, only 8 articles were found that met the inclusion criteria.
This collection of studies has additional limitations. First, the studies reviewed had a variety of comparison groups: bimanual therapy (Chamudot et al., 2018), care as usual (Coker et al., 2009; Cope et al., 2008; Lowes et al., 2014; Nordstrand et al., 2015), baby massage (Eliasson et al., 2018), and no intervention (Fergus et al., 2008; Reidy et al., 2017). Higher level research is needed to determine the effect of infant CIMT when compared with other infant motor interventions and care as usual.
Second, threats to internal validity exist in most studies, because 7 of the 8 studies included parents as primary interventionists (Chamudot et al., 2018; Coker et al., 2009; Eliasson et al., 2018; Fergus et al., 2008; Lowes et al., 2014; Nordstrand et al., 2015; Reidy et al., 2017). Of these 8 studies, only 2 (Eliasson et al., 2018; Lowes et al., 2014) discussed intervention fidelity. Even the study by Cope et al. (2008), which used therapists as the interventionists, indicated that parent participation outside of the therapist-led hours may have affected the positive changes observed in their single-subject research study. Not all studies had parents track hours spent using CIMT principles with their infants. In some cases, researchers attempted to control for this confounding variable by having parents keep a log of their hours (Chamudot et al., 2018; Eliasson et al., 2018; Fergus et al., 2008; Lowes et al., 2014).
Finally, infants with hemiplegic CP present differently, according to the level of impairment. Differences based on level of impairment can influence results and should be accounted for in future studies to determine effectiveness.
Implications for Occupational Therapy Practice
The findings of this scoping review have the following implications for occupational therapy practice: Occupational therapy practitioners can implement a CIMT protocol for infants with hemiplegic CP or at risk for hemiplegic CP. Home programs, parent education, and parent training are important components to promote new skill acquisition in the infant, and clinicians should incorporate these elements into a CIMT program for infants. Higher level research is recommended to determine best practices in regard to dosage, type of restraint, protocol administration, and appropriate outcome measure for occupational therapy clinicians to implement an evidence-based infant CIMT program into clinical practice.
Conclusion
In this scoping review, we aimed to explore the existing evidence related to CIMT for infants with CP and at high risk for CP. As infants are diagnosed at younger ages, occupational therapy practitioners must apply best practices when implementing treatment strategies for this population. However, the results of this review show that consensus on CIMT protocols is lacking. Although more empirical research is needed to define best practices when delivering CIMT to the infant population, recently published international practice guidelines recommend therapist-led, parent-delivered CIMT as part of a comprehensive multidisciplinary approach (Morgan et al., 2021). By organizing the current literature on CIMT for infants with CP, this scoping review lays the foundation for future research. Studies are needed that look at optimal dosage, best constraint, the impact of parent–child engagement, maintenance of newly acquired skills, and the long-term effects of CIMT for infants.
Supplemental Material
Supplementary material for Constraint-Induced Movement Therapy for Infants With or at Risk for Cerebral Palsy: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.047894.pdf for Constraint-Induced Movement Therapy for Infants With or at Risk for Cerebral Palsy: A Scoping Review by Monik Castillo Dionisio and Alexandra L. Terrill in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies included in the scoping review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.