
Abstract
This review advances knowledge about how clinical reasoning has been conceptualized in occupational therapy and has been applied in a range of practice contexts.
Clinical reasoning is recognized as an essential dimension of competent practice across all the health professions (Higgs et al., 2019). In occupational therapy, it is a phenomenon studied since the 1980s, when the first empirical study was published (Rogers & Masagatani, 1982). At that time, a group of researchers met with Donald Schön (known for his work on reflective practice) “to discuss and begin to outline research designed to investigate clinical knowledge and expertise” (Mattingly & Fleming, 1994, p. ix). This meeting gave rise to the Clinical Reasoning Study, resulting in the most cited book on this topic in occupational therapy: Clinical Reasoning: Forms of Inquiry in a Therapeutic Practice (Mattingly & Fleming, 1994).
Since then, the number of clinical reasoning studies in occupational therapy has grown, with aims to better understand clinical reasoning (Leicht & Dickerson, 2002; Mattingly, 1991); identify factors influencing clinical reasoning (Shafaroodi et al., 2014, 2017); examine differences between novice and expert practitioners’ reasoning (Unsworth & Baker, 2016); and examine reasoning in specific fields of practice, such as community (Carrier et al., 2010) and mental health (Chaffey et al., 2010; Ward, 2003), among other purposes.
Clinical reasoning is variously defined in occupational therapy as “a largely tacit, highly imagistic, and deeply phenomenological mode of thinking” (Mattingly, 1991, p. 979); as “the process used by practitioners to plan, direct, perform, and reflect on client care” (Schell, 2014 p. 384); and as a mode of thought that “involves all the thinking processes of the clinician as s/he moves into, through and out of the therapeutic relationship and therapy process with a client” (Unsworth & Baker, 2016, p. 5). These definitions notwithstanding, no one definition captures “the subtlety of how therapists think in the midst of practice” (Mattingly & Fleming, 1994, p. 9). Another contemporary conversation concerns whether professional reasoning may be a more encompassing term, given the growth of nonclinical occupational therapy practice environments (Schell & Schell, 2018). Nonetheless, given its predominant use, the term clinical reasoning was adopted for this scoping review and encompasses both clinical and professional reasoning.
Recent reviews have indicated that most published studies on clinical reasoning in occupational therapy are qualitative, and a large proportion are conceptual articles. Unsworth and Baker (2016) reviewed 140 studies, of which 59 were qualitative, 43 were conceptual or reviews, 20 were quantitative, and 18 were mixed methods. Their review focused on what is known about the development of professional reasoning among students through literature exploring differences between novices and experts. Márquez-Álvarez et al. (2019) reviewed 208 articles and found 149 empirical studies (of which 72 were qualitative, 50 were quantitative, 13 were mixed methods, and 14 were reviews) and 59 nonempirical studies (of which 35 were theoretical). Márquez-Álvarez et al. proposed that the predominance of qualitative research “is likely because qualitative techniques are appropriate to the nature of research questions about clinical reasoning” (p. 6). Nonetheless, the presentation of results in Márquez-Álvarez et al.’s large-scale review focused on description of the bibliographic information, such as the number of articles, historical trends, and methodological aspects, with no description of trends or themes in the process of clinical reasoning itself. Thus, the following elements are still missing: a detailed examination of how clinical reasoning is qualitatively and conceptually depicted in the literature, emergent trends in types of and approaches to clinical reasoning, and discussions of the ways it is enacted.
Despite the prevalence of qualitative and conceptual articles, a gap exists in terms of in-depth analyses of this body of work. This literature contributes rich descriptions of complex phenomena that have not been represented in a meaningful way to date. Therefore, the purpose of this scoping review was to examine how the qualitative and conceptual literature addresses clinical reasoning in occupational therapy. To focus on current scholarly conversations, contemporary shifts in conceptualizations, and emergent perspectives, and to enable a data set that would allow for detailed description of thematic findings, we adopted a 10-yr time frame and included only peer-reviewed literature. Our aim was to thematically map key findings to render a more comprehensive and nuanced picture of the ways clinical reasoning is being conceptualized and applied in occupational therapy.
Method
Drawing on Arksey and O’Malley (2005), we adopted a scoping review methodology “to examine the extent, range and nature of research activity” and “to summarize and disseminate research findings” (p. 21). The five-step methodological framework includes (1) identification of the research question, (2) identification of relevant studies, (3) study selection, (4) data extraction, and (5) data synthesis.
Identification of the Research Question
Two team members (Angelica da Silva Araujo and Elizabeth Anne Kinsella) developed the initial question, which was iteratively refined over time in dialogue with the team members to “What is the current state of knowledge about how clinical reasoning in occupational therapy has been addressed in the peer-reviewed qualitative and conceptual literature?” In this scoping review, qualitative refers to studies that use qualitative methodologies. For mixed methods, only the qualitative dimensions were included. The term conceptual refers to articles that discuss practical, applied, or reflective or philosophical, theoretical, or conceptual propositions.
Identification of Relevant Studies
In early December 2019, Araujo and Kinsella conducted two pilot searches to test the proposed search terms and databases. The inclusion and exclusion criteria, search terms, and databases were iteratively refined by Araujo, Kinsella, Laysla Demonari Gomes, and Tais Quevedo Marcolino through consideration of pilot test results and consultation with a librarian. We conducted the official search in January 2020 across five databases (Scopus, Web of Science, PsycINFO, Embase, and MEDLINE) using the combined search terms clinical reasoning or professional reasoning and occupational therap*; to be included, articles needed to be peer reviewed, published between January 2010 and December 2019, and written in English.
Study Selection
Included studies addressed clinical or professional reasoning in occupational therapy practice, used qualitative methodologies or conceptual/theoretical approaches, focused on occupational therapy practitioners, were published between January 2010 and December 2019, were published in English, and were peer reviewed. Excluded studies focused on students, did not focus primarily on clinical reasoning, were not available in English, were gray literature, or were reviews.
Data Extraction
An Excel data extraction form was iteratively developed by team members according to the research aims. It was pilot tested on five articles and revised until agreement was reached. Final extraction categories included title; author(s); publication year; journal; study objectives, purpose, and research question; type of article; methodology and methods; country of study; number of participating therapists; practice area; definitions and descriptions of clinical reasoning; and main focus and findings. Data were extracted from included articles.
Data Synthesis
Descriptive and thematic analyses were undertaken. The descriptive analysis was used to collate, summarize, and present key information concerning the year, country, methodologies, participants, practice contexts, terminology, and definitions used across studies (see Table A.1 in the Supplemental Appendix, available online with this article at https://research.aota.org/ajot). The thematic analysis involved an iterative and inductive process of identifying qualitative themes through review of the extracted data, rereviewing articles, engaging in dialogue among team members, and mind mapping emergent themes (Davies, 2011). Araujo and Gomes completed independent reviews, identifying study features and emergent themes, followed by meetings and discussions with Kinsella, Marcolino, and Aliki Thomas to iteratively cross-check and critically discuss thematic representations. These processes continued until consensus was reached.
Trustworthiness
Trustworthiness, truth value, and confirmability of data collection and analysis were established through pilot tests of search terms, repetition of searches, hand searches of reference lists, multiple team members involved in each stage, multiple readers to decide inclusion and exclusion of articles, frequent team meetings, and an audit trail.
Results
The initial search generated 554 articles, which were imported into Mendeley reference management software (Mendeley Ltd., London). After deleting duplicates, 189 articles remained. The titles and abstracts of 189 articles were screened according to inclusion and exclusion criteria (by Araujo and Gomes) and were cross-checked (by Kinsella and Marcolino). Through application of inclusion and exclusion criteria, 131 articles were excluded. Full-text screening of the remaining 58 articles was undertaken (by Araujo and Gomes) with disagreements or ambiguities adjudicated by team members (Kinsella and Marcolino), resulting in 26 articles identified for inclusion (Figure 1).
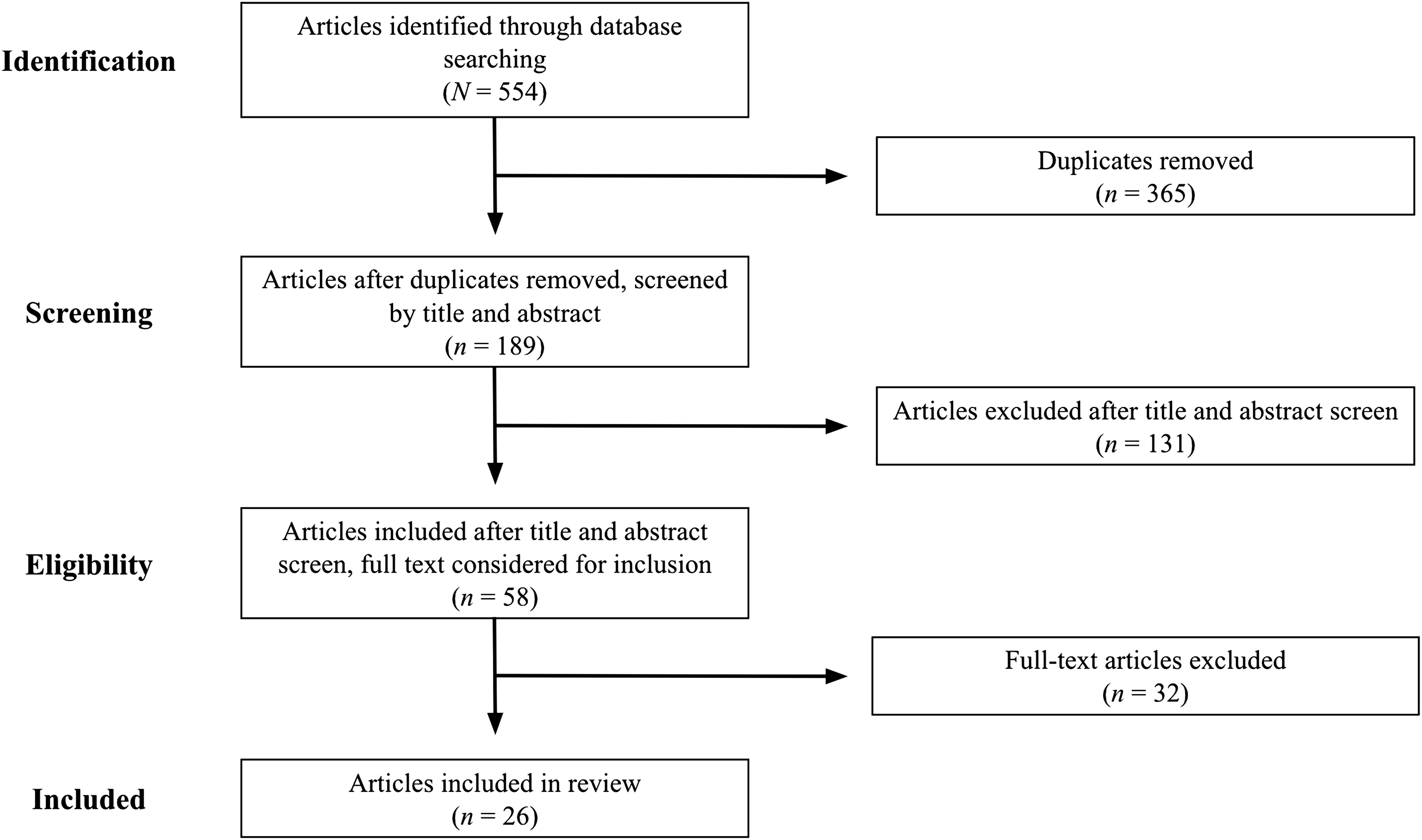
Flow diagram for inclusion and exclusion of peer-reviewed studies in the scoping review.
Description of Articles
The majority of studies were published in 2015 (n = 7) and 2014 (n = 5); most studies were published in the Canadian Journal of Occupational Therapy (n = 4), the American Journal of Occupational Therapy (n = 3), and Occupational Therapy in Health Care (n = 3). In addition, most studies were conducted in the United States (n = 11) and Canada (n = 3). The types of articles included 18 qualitative and 8 conceptual. The methodologies were conceptual/theoretical (n = 8), grounded theory (n = 7), generic qualitative (n = 4), case study (n = 4), qualitative content analysis (n = 1), hermeneutic phenomenology/participatory action research (n = 1), and collaborative research (n = 1). The 18 qualitative studies took place in diverse practice areas. The number of participating occupational therapy practitioners in these studies ranged from 1 to 25.
The majority of the articles (n = 23) used the term clinical reasoning, whereas 5 articles used decision making (Doyle et al., 2014; Faller et al., 2016; Schaaf, 2015; Skubik-Peplaski et al., 2015; Vachon et al., 2010), 3 used professional reasoning (Crowe, 2014; Dennis et al., 2015; DuBroc & Pickens, 2015), 1 used therapeutic reasoning (Bowyer et al., 2019), and 1 used theoretical reasoning (Ikiugu et al., 2019). Seven articles used more than one term (Dennis et al., 2015; Doyle et al., 2014; DuBroc & Pickens, 2015; Faller et al., 2016; Schaaf, 2015; Skubik-Peplaski et al., 2015; Vachon et al., 2010). Most of the articles included definitions or descriptions of clinical reasoning, referring predominantly to publications by the following clinical reasoning theorists: Cheryl Mattingly, Maureen Fleming, Barbara Schell, Carolyn Unsworth, and Joy Higgs.
Thematic Analysis: Clinical Reasoning Themes
The thematic analysis identified four major themes: clinical reasoning processes, factors influencing clinical reasoning, new models or frameworks to guide clinical reasoning, and emergent perspectives on clinical reasoning.
Clinical Reasoning Processes
Clinical reasoning processes were predominantly addressed according to types of clinical reasoning, steps of clinical reasoning, and client centeredness in clinical reasoning.
The classic types of clinical reasoning—procedural, conditional, interactive, pragmatic, narrative, ethical, and scientific—were most frequently adopted (15 articles) and are elaborated in Table A.2. Three other types of reasoning, less known in the literature, were used by 1 or 2 studies each: generalization, whereby therapists use reflection to reframe current cases in light of their broader clinical experiences (Shafaroodi et al., 2017; Unsworth, 2011); political reasoning, which examines power relations to promote occupational justice (Hess & Ramugondo, 2014); and diagnostic reasoning, which focuses on the cause or nature of conditions (Arntzen, 2018). Some articles showed how occupational therapy practitioners used one type of reasoning (Ikiugu et al., 2019; Kristensen et al., 2012; Skubik-Peplaski et al., 2015), two types together (Park, 2012), or various types independently or in combination (Unsworth, 2011).
Steps of clinical reasoning were identified in 4 studies. Carrier et al. (2012) described three phases and eight stages of clinical reasoning that community occupational therapy practitioners used with older adults; these stages evolved from a generic to a personalized mode. Hess and Ramugondo (2014) identified three steps that therapists could use to address spirituality in mental health. Shafaroodi et al. (2017) found that occupational therapy practitioners from diverse fields applied a dynamic process of clinical reasoning using four steps. In addition, Cheung et al. (2018) highlighted that therapists working on ergonomic education for women with repetitive strain injury made clinical decisions based on three stages of clients’ behavior change. In these studies, the steps described were unique, context specific, and nonlinear. Carrier et al. highlighted reasoning as circular, extremely fast, and constant, whereas Hess and Ramugondo described it as complex, dynamic, multilayered, complicated, and iterative.
Client centeredness in clinical reasoning was a primary central focus in 4 studies, and a secondary focus in 5 studies. Carrier et al. (2012) stated that therapists’ reasoning was consistent with client-centered practice with a focus on relationships with clients and the social environment. Crowe (2014) reported that therapists selected multiple sensory environments for interventions with people with dementia on the basis of their assumptions that these settings favored client-centered care. Hess and Ramugondo (2014) described mental health therapists’ clinical reasoning as considering clients’ views and perspectives about their occupations. Finally, Kristensen et al. (2012) outlined how therapists’ reasoning focused on client centeredness in stroke rehabilitation by considering patients’ experiences. A secondary focus on client centeredness was depicted in studies that proposed resources to support client-centered reasoning processes (Ashburner et al., 2014; Faller et al., 2016; Matthews et al., 2017; Schaaf, 2015; Yancosek & Howell, 2010).
Factors Influencing Clinical Reasoning
A predominant theme addressed how factors related to therapists, clients, and practice contexts influenced clinical reasoning. Factors related to therapists were identified in 10 articles. Several articles focused on therapists’ level of experience, education, or knowledge as influencing expertise, competence, or capabilities in clinical reasoning (Bowyer et al., 2019; Carrier et al., 2012; DuBroc & Pickens, 2015; Kristensen et al., 2012; Shafaroodi et al., 2014, 2017; Stark et al., 2015). Other influential factors identified were therapists’ self-confidence (Shafaroodi et al., 2014, 2017), attitudes and preferences toward patients and diagnoses (Shafaroodi et al., 2014), beliefs about the setting’s support for client-centered care (Crowe, 2014), professional habits (Skubik-Peplaski et al., 2015), personal habits (Cheung et al., 2018), and personal features such as emotional availability and personality (Carrier et al., 2012).
Client factors that influence clinical reasoning were highlighted in 6 studies. These factors included diagnosis, level of impairment, coexisting medical conditions, rate of recovery, clinical course of the health condition, and functional characteristics (Carrier et al., 2012; Doyle et al., 2014; Shafaroodi et al., 2014; Stark et al., 2015); beliefs, knowledge, understandings, openness, motivation, honesty, and acceptance of their situations (Carrier et al., 2012); cooperation with the therapist (Shafaroodi et al., 2014; Stark et al., 2015); abilities to implement changes (Cheung et al., 2018); cognitive capacities and personality characteristics (Stark et al., 2015); educational level and learning style (Carrier et al., 2012; Shafaroodi et al., 2014); preferences regarding human assistance, architectural modifications, adaptive equipment, and aesthetic preferences (Stark et al., 2015); and financial resources (Shafaroodi et al., 2014, 2017; Stark et al., 2015).
Factors related to the practice context were identified as influencing clinical reasoning in 9 studies (Carrier et al., 2012 ; Cheung et al., 2018 ; Doyle et al., 2014 ; Hess & Ramugondo, 2014 ; Kristensen et al., 2012 ; Shafaroodi et al., 2014, 2017 ; Skubik-Peplaski et al., 2015 ; Stark et al., 2015). The type of setting was highlighted as influencing clinical reasoning. In hospitals, acute care, and inpatient settings, occupational therapy practitioners were reported to adopt a medicalized perspective (Shafaroodi et al., 2014); consider the doctor’s goals, diagnosis, and symptoms more than client preferences (Shafaroodi et al., 2017); and prioritize patient independence to relieve workload, even when it worked against client-centered practice (Kristensen et al., 2012). In contrast, in day centers, community-based centers, and outpatient settings, therapists reportedly assessed the effect of illness on clients and their environment, facilitated change in clients’ occupational performance and environment, organized information according to clients’ preferences (Shafaroodi et al., 2017), viewed clients from a holistic perspective (Shafaroodi et al., 2014), and focused more on activities of daily living (Doyle et al., 2014).
Other environmental characteristics identified as directing, facilitating, or challenging clinical reasoning were rules of the workplaces (Hess & Ramugondo, 2014); physical facilities, noise, crowd levels, financial constraints, and limited community services (Shafaroodi et al., 2014); availability of space and time (Cheung et al., 2018); organization of equipment in the workplace (Skubik-Peplaski et al., 2015); structural conditions of the home, housing type, available space, layout, and housing condition in the field of home modifications (Stark et al., 2015); and workplaces’ organizational elements (Carrier et al., 2012).
Factors in the social context were social attitudes or stigma (Shafaroodi et al., 2014, 2017; Stark et al., 2015), level of caregiver involvement (Stark et al., 2015), absence of caregivers (Carrier et al., 2012), neighborhood safety (Stark et al., 2015), unrealistic expectations by managers and colleagues (Shafaroodi et al., 2014, 2017), and collateral information provided by coworkers (Hess & Ramugondo, 2014).
New Models or Frameworks to Guide Clinical Reasoning
New models, frameworks, guidelines, or combinations of theories to guide clinical reasoning were proposed in 7 studies (Ashburner et al., 2014 ; Carrier et al., 2012 ; Faller et al., 2016 ; Matthews et al., 2017 ; Schaaf, 2015 ; Stark et al., 2015 ; Yancosek & Howell, 2010). Matthews et al. (2017) proposed the Matthews model of clinical reasoning, which draws on the occupational profile and analysis of occupational performance to guide reasoning from an occupation-based, holistic, and client-centered approach. Ashburner et al. (2014) proposed a clinical reasoning framework to guide therapists in selecting strategies to optimize participation of children with autism spectrum disorder experiencing sensory challenges. Information sharing with families is the basis of this framework, which attends to research, family centeredness, practice contexts, occupation centeredness, and risks. Emphasizing the integration of evidence, theory, and context, Schaaf (2015) proposed the Data-Driven Decision Making framework to guide occupational therapy practitioners to reason systematically, use assessment data to tailor client-centered intervention, and measure and report outcomes. Faller et al. (2016) conducted a case study of this framework and reported that it facilitated a systematic reasoning process whereby therapists describe their reasoning and the data-based rationale for decisions, use a client- centered approach, tailor interventions, and clearly document outcomes.
For rehabilitation contexts, Yancosek and Howell (2010) proposed a combination of a theory (dynamic systems theory), a model of practice (task-oriented approach), and a framework (Occupational Therapy Practice Framework: Domain and Process [2nd ed.]; American Occupational Therapy Association, 2008) to guide occupational therapy practitioners’ clinical reasoning processes. They highlighted ideological similarities among these resources, including a focus on client centeredness, occupation, and interaction (among person, task, and environment). Carrier et al. (2012) proposed a three-phase clinical reasoning framework for community occupational therapy practitioners who teach transfer skills to older adults: development of the teaching plan, finalization of the choice of teaching plan, and adaptation in action of the teaching plan. In the field of home modifications, Stark et al. (2015) developed a guideline to support clinical reasoning containing 16 factors that expert therapists routinely assess.
Emergent Perspectives on Clinical Reasoning
Emergent perspectives on clinical reasoning were featured in 8 articles (Arntzen, 2018 ; Chaffey et al., 2010 ; Dennis et al., 2015 ; Hess & Ramugondo, 2014; Kristensen & Petersen, 2016; Park, 2012 ; Robertson et al., 2015 ; Vachon et al., 2010). Arntzen (2018) argued that clinical reasoning is comprehended mainly through scientific–analytic knowledge focused on cognition, metacognition, narrative, and sociocultural approaches, which tend to ignore how reasoning emerges through embodied aspects arising through contextualized interaction between patients and therapists. Arntzen proposed an embodied and intersubjective perspective based on Merleau-Ponty’s (1945/2012) phenomenology of the body. This approach involves reflecting on how shared intentionality shapes professional judgments, and it explores how judgments are generated from reciprocal embodied interactions among the therapist, patient, and surroundings.
Chaffey et al. (2010) found that therapists described intuition in their clinical reasoning as instinctive, a hunch, common sense, and a gut feeling. They reported that therapists attempted to hide their use of intuition from colleagues out of fear regarding perceptions of credibility, highlighting the use of intuition as an “underground practice.” Hess and Ramugondo (2014) identified that in mental health practice, therapists found it rewarding to consider spirituality in their reasoning processes. Therapists reported that attention to spirituality allowed them to better understand their clients and to acknowledge diversity in themselves, team members, and clients. However, attention to spirituality in the reasoning process was also described as an underground practice.
In the field of work rehabilitation, Vachon et al. (2010) named new modes of reasoning used in difficult practice situations and associated with therapists’ emotional states. Defensive mode, guided by legal and administrative constraints, was associated with feeling threatened and not wanting to be blamed for unsuccessful interventions. Repressed mode, guided by the systems of the work environment, was associated with feelings of powerlessness. Cautious mode, guided by acquired practical knowledge, was associated with feeling insecure about doing the wrong thing. Autonomous mode, guided by the desire to help clients overcome work-related disability, was associated with feeling curious and the wish to improve practice.
In a single case study, Park (2012) used resources drawing on narrative and aesthetic theory to provide a vocabulary to articulate how a therapist wove sensory integration procedures with procedural and narrative reasoning in her work with a child. Expressions such as bodily sensing, throwing breaches, and making scenes were created as embodied metaphors to show narrative aesthetic reasoning in practice.
Dennis et al. (2015) called for occupational therapy practitioners to include environmental sustainability in clinical reasoning, discussing how overpopulation, environmental degradation, global climate change, and extreme weather events can disrupt human occupations. They highlighted the importance of adopting more ecologically and socially based perspectives, calling for therapists to consider the rights of communities as well as occupational and social justice issues in their reasoning processes as an ethical obligation to build a sustainable and resilient future.
Kristensen and Petersen (2016) considered how occupational science can contribute to the development of clinical reasoning, highlighting how an occupational perspective connects to human development, well-being, and health; they also discussed the impact of cultural and social factors on occupations. Robertson et al. (2015), departing from the idea that the bulk of occupational therapy practitioners’ reasoning is intuitive, embodied, or subconscious, proposed a “critical occupational therapist” as a professional with highly developed conscious thinking skills used to produce rationally informed decisions. This stance incorporates critical reason, critical self-reflection, and critical action.
Discussion
The findings of this scoping review fill a gap in the peer-reviewed literature by mapping and examining the state of the qualitative and conceptual work on clinical reasoning in occupational therapy emerging over a recent 10-yr period. Concerning terminology, the term clinical reasoning was most frequently used, with only a few articles adopting the terminology of professional reasoning or decision making. This finding is consistent with Young et al.’s (2020) review of literature concerning health professionals’ clinical reasoning, which identified 110 terms, noting clinical reasoning as the term most frequently used in occupational therapy. It is interesting to note that Schell and Schell (2018) adopted both terms in the book Clinical and Professional Reasoning in Occupational Therapy. As occupational therapy practitioners continue to expand their scope of practice beyond traditional clinical contexts into more sociocultural and civic domains, the terminology used may continue to be a point of productive tension, evolution, and dialogue. The majority of the literature in this review drew on seminal theorists such as Mattingly, Fleming, Schell, Unsworth, and Higgs. Most sources are linked to seminal books and articles that have drawn on occupational therapy literature, with few conversations intersecting with distinct and robust bodies of clinical reasoning literature that have emerged in other fields (Merkebu et al., 2020; Young et al., 2018).
Procedural, conditional, interactive, pragmatic, narrative, and ethical reasoning were the types most frequently discussed. This predominance may be linked to the emergence of these types of reasoning in the field of occupational therapy itself, such as through Mattingly and Fleming’s (1994) three-track mind, and may reflect the popular uptake of these discourses in the profession over time. Other types, less frequently discussed, were approaches aligned with broader discourses linked to evidence-based practice and medical science, such as scientific and diagnostic reasoning. These types of reasoning, discussed more frequently in health and medical sciences, point to modest intersections of broader health sciences clinical reasoning scholarship in occupational therapy. Political reasoning discussed in one article links to broader ideological agendas oriented toward social justice, which are beginning to appear more frequently in occupational therapy literature (Kinsella & Durocher, 2016).
Various contextual dimensions emerged as important influences on clinical reasoning. Contextual factors were related to the environments of practice, to the occupational therapy practitioners, and to the clients; these findings are consistent with a body of evidence emerging in the clinical reasoning literature from other health professions, and they highlight the need for urgent attention to contextual dimensions in reasoning processes (Bucknall, 2003; Huhn et al., 2019; Rencic et al., 2020; Young et al., 2020). The significance of context, the unpredictability and complexity of practice-based situations, and the different people who come together in those contexts underline the importance of practitioner reflection in the reasoning process (Kinsella, 2010; Schön, 1983). The importance of ongoing reflection-in-action as a means to attend to contextual factors in clinical reasoning processes is an important area for attention.
Our findings show that discussions of clinical reasoning frequently focus on steps, stages, systematizations, frameworks, and models; yet, they also emphasize that reasoning is not linear. Clinical reasoning was regularly described as iterative, dynamic, circular, fast, and contextually based, with different types working together. This finding suggests that although frameworks may be practically useful, it is also important to look beyond linear or rote applications and to attune to dynamic elements of contextually based reasoning processes.
Moreover, a central focus on client-centered and occupation-based perspectives was frequently identified, shedding light on specific aspects for understanding clinical reasoning in occupational therapy. Although a client-centered focus has recently emerged as important in other disciplines (Eklund et al., 2019), the interrelation among client, context, and occupation has historically been a focus, and is deeply embedded, in occupational therapy. Unsworth (2004) highlighted that client centeredness is closely linked to the narrative/phenomenological mode of reasoning taken up in occupational therapy. Calls to center occupation in clinical reasoning are consistent with calls to focus on occupation as a central concern in occupational therapy education and practice (Fisher, 2013). This outlook parallels the placement of a disciplinary focus on occupation in the reasoning process, as in the profession of medicine’s emphasis on diagnosis through diagnostic reasoning. The emergence of an occupation-centered focus may signal a maturation of the discipline of occupational therapy and may indicate a positive direction for the profession.
Emergent perspectives also emphasize broader considerations related to social justice and rights of communities, particularly focusing on ecological sustainability and political considerations. In these times when a widespread recognition of structural oppression and social injustice is emerging, reasoning in which social and occupational justice are centered is crucial to the evolution of the profession (Kinsella & Durocher, 2016). An evocative range of articles discussed emergent perspectives, pointing to new and important trends and new ways of conceptualizing clinical reasoning as well as bringing to light less visible areas of reasoning. These articles highlighted dimensions beyond the strictly cognitive–rational aspects of clinical reasoning, focusing on embodiment, intuition, spirituality, emotion, and aesthetics. Some authors described these reasoning processes as underground practices and discussed how therapists may hide them out of a fear of not being taken seriously. Underground practices involve the concealment of aspects of practice from public discourse (Mattingly & Fleming, 1994). Making underground practices explicit is important for making tacit aspects of practice more visible and for legitimizing them.
Embodiment and the exploration of the body as a means of perception in clinical reasoning is an important and emerging area of scholarship in occupational therapy (Arntzen, 2018; Kinsella, 2018; Schell & Schell, 2018). One article focused on intuition (Chaffey et al., 2010), suggesting emerging interest in this area. It is interesting to note that a focus on intuition as part of clinical reasoning is gaining momentum in the health professions literature (Melin-Johansson et al., 2017; Vanstone et al., 2019), notably in dual-process theories (Evans, 2018). Spirituality, emotion, and aesthetics in the clinical reasoning process also represent emergent domains that have received little attention and may be regarded as taboo. To discuss reasoning in these domains and to make these processes more explicit may help therapists share experiences and grapple with the affordances and challenges of less tangible approaches. The need to develop a language to name complex and multifaceted aspects of reasoning in occupational therapy practice has been recommended as essential by Marcolino et al. (2019). In this scoping review, the naming of tacit reasoning processes was a central outcome of Hess and Ramugondo’s (2014) work describing how spirituality can be centered in therapists’ practices in mental health, Vachon et al.’s (2010) proposal to name particular modes of emotional reasoning, and Park’s (2012) descriptive evocative language to show narrative aesthetic reasoning in practice.
Study Strengths and Limitations
Strengths of this study include the rigor of the application of the scoping review methodology as well as the expertise of the team in clinical reasoning scholarship and scoping review methodologies. Our findings present a robust descriptive and thematic analysis of the contemporary conceptual and qualitative landscape of clinical reasoning, and they advance understandings of a decade of literature. Limitations include the exclusion of gray literature (where several writings that shaped the field were published) and the focus on English language (excluding scholarship published in languages other than English). Focusing on clinical reasoning and professional reasoning may have limited the search; other terms, such as decision making, may have elicited further relevant studies.
Future Research
Emergent perspectives on clinical reasoning that attend to embodiment and intuition, which are currently gaining traction in other fields, are potentially fruitful areas for further research. Investigations into underground practices in clinical reasoning are strongly recommended to increase their visibility, make tacit dimensions explicit, and develop a language to communicate about such practices. Explorations into the iterative nature of reasoning processes, and the intersections between reflection and clinical reasoning, would be fruitful, especially in the context of uncertainty, complexity, and indeterminancy in practice.
Research that continues to examine how unique factors related to contextual dimensions of practice—including institutional environments, clients, and therapists—shape reasoning processes is recommended. In addition, research into the identified models and frameworks is recommended, given that only one framework (Schaaf, 2015) has been tested in another study (Faller et al., 2016).
How ideological perspectives shape reasoning processes is an interesting line of inquiry. Investigations into how discourses of evidence-based practice, biomedical, and diagnostic rationalities shape clinical reasoning could shed light on important factors. Further investigations into how “client-centered practice” and “occupation” are considered in therapists’ reasoning processes are recommended. Reasoning informed by mandates of social justice or social responsibility, such as political reasoning, ecological reasoning, or reasoning oriented toward occupational justice, is an important direction at this moment of growing social consciousness in occupational therapy. Research into how implicit biases shape reasoning processes was not directly noted; however, biases may relate to reports of preferences for particular “types” of clients. This topic seems salient as issues of structural racism, structural oppression, and structural violence move to the forefront of therapists’ disciplinary consciousness.
None of the articles examined occupational therapy practitioners’ reasoning in interprofessional contexts or communities of practice; however, research into collaborative approaches to reasoning is an area that could advance practice. Educational approaches to improve clinical reasoning were not included but offer important avenues for future research. Research that draws on clinical reasoning scholarship from other disciplines, and that incorporates diverse epistemological and interdisciplinary perspectives, may also enrich scholarship in this area.
Implications for Occupational Therapy Practice
Clinical reasoning is portrayed in the qualitative and conceptual literature in a variety of ways that may be fruitful for practice. Occupational therapy practitioners may reflect on themes in this scoping review and consider potential implications for practice by recognizing established and emergent forms of clinical reasoning; testing out new models and frameworks; acknowledging iterative, dynamic, and contextualized reasoning processes; attuning to contextual features in the reasoning process; recognizing client centeredness and occupation-centered aspects of reasoning; working to make tacit underground clinical reasoning practices more explicit; and exploring tacit (embodiment, emotions, intuition, spirituality, and aesthetic) as well as cultural and social dimensions (political, sustainability) of reasoning processes.
Conclusion
This scoping review gives visibility to aspects already embedded in occupational therapy clinical reasoning scholarship and maps out key terminology and approaches. It also underlines the importance of contextual dimensions of reasoning, the dynamic and iterative nature of reasoning, new frameworks and models to guide reasoning, and innovative and emergent perspectives on reasoning. This review shows that the focus on client-centered approaches currently lauded in other health professions is well established in clinical reasoning in occupational therapy. Moreover, a disciplinary focus that centers occupation in the reasoning process is gaining some attention and may parallel disciplinary approaches such as diagnostic reasoning in medicine. This review suggests that “underground practices” in clinical reasoning may be important avenues for further research to bring tacit dimensions into view. Engagement with broader health sciences literature may be useful to advance understandings of some forms of reasoning, such as intuitive reasoning. In addition, emerging areas such as embodied reasoning, emotional reasoning, and ecological reasoning point to new avenues for exploration. Professional practice can be enriched by the findings insofar as they shed light on tacit and complex processes as well as open new conversations relevant to practice. Occupational therapy education, which maps approaches to clinical reasoning and highlights reflection as an important strategy requiring attention, can also benefit from this review.
Supplemental Material
Supplementary material for Clinical Reasoning in Occupational Therapy Practice: A Scoping Review of Qualitative and Conceptual Peer-Reviewed Literature
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.048074.pdf for Clinical Reasoning in Occupational Therapy Practice: A Scoping Review of Qualitative and Conceptual Peer-Reviewed Literature by Angelica da Silva Araujo, Elizabeth Anne Kinsella, Aliki Thomas, Laysla Demonari Gomes and Tais Quevedo Marcolino in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We acknowledge the following Brazilian research agencies for support of this research: Brazilian Federal Foundation for Support and Evaluation of Graduate Education (Grant 001) and São Paulo Research Foundation (Grant 2017/03195-8).
*
Indicates studies included in the scoping review.
Appendix. Supplemental Tables
Types of Clinical Reasoning and Corresponding Articles
| Type of Clinical Reasoning | Articles |
|---|---|
| Procedural reasoning involves identifying clients’ challenges and selecting the procedures that might be used to help people reduce the effects of those challenges. | Arntzen (2018); Chaffey et al. (2010); Ikiugu et al. (2019); Kristensen et al. (2012); Matthews et al. (2017); Park (2012); Shafaroodi et al. (2017); Skubik-Peplaski et al. (2015); Unsworth (2011) |
| Conditional reasoning moves beyond specific concerns about the person and their immediate challenges to consider the issues in a broader social and temporal context. | Arntzen (2018); Chaffey et al. (2010); Dennis et al. (2015); Hess & Ramugondo (2014); Kristensen et al. (2012); Matthews et al. (2017); Shafaroodi et al. (2017); Skubik-Peplaski et al. (2015); Unsworth (2011) |
| Interactive reasoning involves face-to-face encounters and exchanges between the therapist and client. It is a form of reasoning used to better understand the person. | Arntzen (2018); Chaffey et al. (2010); Hess & Ramugondo (2014); Kristensen et al. (2012); Matthews et al. (2017); Shafaroodi et al. (2017); Skubik-Peplaski et al. (2015); Unsworth (2011) |
| Pragmatic reasoning takes into account pragmatic dimensions such as the personal and practice contexts within practice environments. | Arntzen (2018); Dennis et al. (2015); Hess & Ramugondo (2014); Ikiugu et al. (2019); Matthews et al. (2017); Shafaroodi et al. (2017); Unsworth (2011); Vachon et al. (2010) |
| Narrative reasoning involves storied accounts that place events within a temporal historical context; it informs therapist’s actions in relation to the past and anticipated futures. | Arntzen (2018); Hess & Ramugondo (2014); Matthews et al. (2017); Park (2012); Shafaroodi et al. (2017); Unsworth (2011); Vachon et al. (2010) |
| Ethical reasoning is a systematic approach to ethical issues; it is directed toward analyzing ethical dilemmas, generating alternative solutions, and discerning action. | Arntzen (2018); Dennis et al. (2015); Hess & Ramugondo (2014); Kristensen & Petersen (2016); Matthews et al. (2017); Shafaroodi et al. (2017); Unsworth (2011) |
| Scientific reasoning involves the use of logical methods, such as hypothesis testing, pattern recognition, theory-based decision making, and statistical evidence. | Arntzen (2018); Dennis et al. (2015); Hess & Ramugondo (2014); Matthews et al. (2017); Unsworth (2011); Vachon et al. (2010) |
| Generalization is used when therapists reason about a particular client issue by reflecting on their broader experiences and integrating their thinking. | Shafaroodi et al. (2017); Unsworth (2011) |
| Political reasoning involves consideration of power dynamics within everyday occupations and collaboration with others to promote occupational justice. | Hess & Ramugondo (2014) |
| Diagnostic reasoning is the analysis of bio-medical causes or conditions that shape the need for occupational therapy intervention. | Arntzen (2018) |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.