
Abstract
This study is the first of its kind to offer evidence that the suicide risk posed by postconcussive symptoms (PCS) may in part be explained by participation restrictions. Occupational therapy practitioners may mitigate veterans’ suicide risk by directly managing PCS and enabling participation despite such symptoms.
Veterans are 1.5 times more likely to die by suicide than their nonveteran counterparts, with a rate of 16.8 deaths by suicide per day (U.S. Department of Veterans Affairs [VA], 2019). Moreover, this trend appears to be worsening: The age- and sex-adjusted rates of veteran deaths by suicide have risen from 18.5 per 100,000 in 2005 to 27.7 per 100,000 in 2017 (VA, 2019). Emerging evidence indicates that disability secondary to service-connected injuries (e.g., mild traumatic brain injury [mTBI]) may contribute to veterans’ heightened suicide risk (Khazem, 2018; Reger et al., 2018). Evidence supporting disability as a risk factor for suicide suggests an important role for occupational therapy within multidisciplinary suicide prevention efforts, but this role remains poorly defined (Kashiwa et al., 2017). Building empirical support for intervention targets within the scope of occupational therapy practice can inform the development and evaluation of suicide prevention services for at-risk veterans.
A history of mTBI heightens risk for suicide (Fralick et al., 2019) and is a “signature injury” among veterans of Operations Enduring Freedom, Iraqi Freedom, and New Dawn (i.e., post–9/11 veterans; Tanielian et al., 2008). Compared with veterans without traumatic brain injury (TBI), veterans with mTBI are 1.62 times as likely to die by suicide, even after accounting for other risks for suicide, such as psychiatric conditions (Hostetter et al., 2019). Emerging evidence indicates that postconcussive symptoms (PCS)—the physical, emotional, and cognitive symptoms associated with mTBI (Bahraini et al., 2018)—pose a risk for suicide-related outcomes. In a study of military personnel, Campbell-Sills et al. (2020) revealed that more severe PCS increased risk for future suicide attempts. Similarly, in a sample of veterans with mTBI, Crocker et al. (2019) highlighted a link between PCS and suicidal ideation. Nonetheless, the mechanisms underlying the purported relationship between PCS and suicidal thoughts and behaviors remain poorly understood (Campbell-Sills et al., 2020).
Participation restrictions may in part explain the relationship between PCS and suicidal thoughts and behaviors. Although participation lacks a definitional consensus, it can be considered to be the involvement in activities that fulfill socially and culturally defined roles (e.g., parent), foster connections with others, and elicit subjective meanings (e.g., perceived competence; Cogan & Carlson, 2018). More severe PCS have been associated with reduced participation in veterans with TBI (Cogan et al., 2020; O’Rourke et al., 2019). Participation restrictions associated with PCS may, in turn, pose a risk for suicidal thoughts. A recent study found that participants with self-reported participation restrictions were 3.5 times as likely to experience suicidal ideation relative to those without such restrictions, even after psychiatric conditions had been taken into account (McConnell et al., 2016). However, little is known regarding whether participation restrictions help explain the relationship between PCS and suicidal thoughts and behaviors among veterans with mTBI.
The purpose of this study was to examine direct and indirect effects of PCS on risk for suicidal thoughts among post–9/11 veterans with mTBI. The evidence supports a relationship between (1) PCS and participation restrictions (Cogan et al., 2020; O’Rourke et al., 2019) and (2) participation restrictions and suicidal ideation (Lutz & Fiske, 2018; McConnell et al., 2016). Thus, we hypothesized that the relationship between PCS and suicidal ideation would be mediated by participation (i.e., role performance). An understanding of the potential mechanisms (i.e., participation restrictions) by which PCS and suicidal ideation are related may inform suicide prevention strategies for veterans with mTBI.
Method
Participants and Procedure
Recruitment and study procedures were approved by the local institutional review board and VA committees. Veterans eligible for Veterans Health Administration (VHA) care at a single VHA health care site were recruited to participate using flyers, referrals from providers, and intake appointments of new veterans. Interested participants were screened for eligibility using brief questions and a review of electronic medical records (all records before the screening period of February 2014–October 2015). The three inclusion criteria were as follows: (1) age 18 yr or older, (2) deployed after 9/11, and (3) a history of mTBI. Those with a history of moderate or severe TBI, other neurological disease, inability to provide informed consent, and current involvement in the criminal justice system were excluded. Three hundred sixty-six veterans were screened, of whom 147 were eligible, and 145 completed the study measures during a single in-person session (2 eligible participants did not complete the consent process and study measures).
Measures
Mild Traumatic Brain Injury
Lifetime TBI history and severity were assessed with the Ohio State University TBI Identification Method (Corrigan & Bogner, 2007). Mild TBI was operationalized as a blow or jolt to the head producing an alteration of consciousness, posttraumatic amnesia ≤24 hr, and/or loss of consciousness ≤30 min. We also assessed whether the mTBI had occurred during deployment.
Covariates
We included age, gender, and lifetime diagnosis of posttraumatic stress disorder (PTSD) as covariates. Lifetime PTSD diagnosis was evaluated by trained researchers using the PTSD module of the Structured Clinical Interview for DSM–IV (Spitzer et al., 1995).
Postconcussive Symptoms
We used the 22-item Neurobehavioral Symptom Inventory (NSI; Cicerone & Kalmar, 1995) to measure PCS. Participants rate severity of symptoms on a scale that ranges from 0 (none) to 4 (very severe). Three subscales were constructed by summing items corresponding to domains from a recent study of post-9/11 veterans (Mood–Behavioral, Vestibular–Sensory, and Cognitive; Bahraini et al., 2018). The Mood–Behavioral domain contains 7 items (scores range from 0 to 28), the Vestibular–Sensory domain contains 11 items (range = 0–44), and the Cognitive domain contains 4 items (range = 0–16).
Participation
To measure participation, we used two subscales of the Medical Outcomes Study Short Form–36 (SF–36; Ware & Sherbourne, 1992): (1) Role Limitations Due to Physical Problems (four items) and (2) Role Limitations Due to Emotional Problems (three items). We selected this measure because it assesses role functioning, a critical dimension of participation after veterans return to the community (Resnik et al., 2012). Participants are asked to report whether physical or emotional problems (yes or no) had limited daily participation in role-fulfilling activities in the past 4 wk (e.g., “cut down on the amount of time you spent on work or other activities”). We used procedures outlined by Ware et al. (1993) to aggregate the items and derive continuous summary scores for the two subscales, with higher scores indicating greater participation.
Presence of Suicidal Ideation
We used the Beck Scale for Suicide Ideation (Beck & Steer, 1991) to assess the presence of suicide-related thoughts. This 21-item self-report scale measures the suicidal intensity of current attitudes, behaviors, and plans on a scale ranging from 0 (e.g., I have a moderate to strong wish to live) to 2 (e.g., I have no wish to live). A response of >0 for initial screening items can be used to identify suicidal ideators (Beck & Steer, 1991); this dichotomous variable was used in our analyses (i.e., no suicidal ideation vs. presence of suicidal ideation).
Data Analysis
Bivariate correlations between observed study variables were derived, and descriptive statistics were calculated, both for the total sample and for the sample stratified by presence of suicidal ideation. We tested differences across suicidal ideation status regarding categorical and continuous observed study variables using χ2 and independent-samples t tests, respectively. No missing data were encountered during this study. We estimated structural equation models (SEMs) using a robust maximum likelihood estimator (MLR) and logit link (i.e., logistic regression) in Mplus (Version 8.1; Muthén & Muthén, 1998–2017) to investigate our hypothesis. The SEMs included two latent variables: (1) PCS and (2) participation. We used item parcels to identify latent constructs because of the small sample size (Little et al., 2013). We identified latent constructs using facet-representative parceling, which aggregates individual items on the basis of shared content with the aim of combining items that share specific variance (Little et al., 2002, 2013). We used facet-representative parceling for two reasons: (1) it is ideal for identifying multidimensional constructs with well-defined domains, and (2) it tends to reduce bias in parameter estimation (Hall et al., 1999; Little et al., 2013).
The PCS latent variable consisted of three parcels, each representing the summary score for the Mood–Behavioral (7 items), Vestibular–Sensory (11 items), and Cognitive (4 items) domains of the NSI (Bahraini et al., 2018). The participation latent variable comprised two parcels, each representing the summary score for the Role Limitations Due to Physical Problems (4 items) and Role Limitations Due to Emotional Problems (3 items) domains of the SF–36 (Ware & Sherbourne, 1992; Ware et al., 1993). We estimated factor loadings and constrained the factor variance to 1 to identify latent variables. Consistent with default procedures in Mplus, latent variable means/intercepts were fixed at 0.
We examined two SEMs to test our hypothesis. First, we specified a model (Model 1) that estimated (1) the relationship between the latent PCS variable and the latent participation variable and (2) the relationship between the latent participation variable and suicidal ideation. Because modeling categorical outcomes with MLR does not yield typical goodness-of-fit measures for SEMs, we compared the Bayesian information criterion (BIC) of Model 1 with the fully saturated model to evaluate initial model fit. We specified a second model (Model 2) that additionally estimated the direct relationship between PCS and suicidal ideation while adjusting for participation. We used the Satorra–Bentler χ2 difference test (Satorra & Bentler, 2010) and the BIC to compare model fit, thus determining which of the competing models was most consistent with the data. We estimated the indirect effect of PCS on suicidal ideation to test our hypothesis using the Model Constraint command in Mplus. The indirect effect was derived using the product-of-coefficients method, which yields more precise estimates for categorical dependent variables (MacKinnon et al., 2007). The ratio of observations to number of parameters for both models (>10) indicates that our sample size could achieve accurate parameter estimates (Jackson, 2003; Kline, 2011). Estimates were adjusted for age, gender, and presence of PTSD; statistical significance was evaluated at α = .05.
Results
Among the 145 veterans who completed the study measures, the majority were men (92.4%), and the average age was 33.1 (SD = 7.7). The majority (76.6%) met criteria for a lifetime diagnosis of PTSD, and 90.4% had sustained a deployment-related mTBI. Veterans who endorsed suicidal ideation had more severe PCS and lesser role performance relative to those without suicidal ideation (Table 1). Descriptive statistics for all observed indicators are presented in Table 1; bivariate correlations are given in Table 2.
Descriptive Statistics
Note. N = 145. df = degree of freedom; PTSD = posttraumatic stress disorder.
For categorical study variables stratified by suicidal ideation status, percentages were derived using variable characteristic totals (i.e., row values) as the denominator.
p < .05.
p < .01.
Bivariate Correlations Between Observed Variables
Note. N = 145. PCS = postconcussive symptoms.
Point-biserial correlations.
p < .05.
p < .01.
p < .001.
Parameter Estimates for Model 1
Note. N = 145. Dash = data not applicable; b = unstandardized parameter estimate; β = standardized parameter estimate; CI = confidence interval for standardized parameter estimates and odds ratios (ORs); PCS = postconcussive symptoms; PTSD = post traumatic stress disorder.
We examined measurement model fit first. Standardized factor loadings for the Mood–Behavioral (β = .90, SE = .02), Vestibular–Sensory (β = .80, SE = .04), and Cognitive (β = .89, SE = .03) domain item parcels were high, indicating a good fit for the postconcussive latent variable. Similarly, item parcels reflecting role limitations due to physical (β = 0.78, SE = 0.05) and emotional health (β = .79, SE = .05) exhibited good fit for the latent participation variable.
Model 1, which excluded the estimated effect of PCS on suicidal ideation, was then specified, and model fit was evaluated. Compared with the saturated model (BIC = 4,963.18), Model 1 exhibited better fit (BIC = 4,887.91). The BIC difference of 75.27 represents “very strong” evidence in favor of Model 1 relative to the saturated model, indicating acceptable model fit (Raftery, 1995). We then compared model fit for Models 1 and 2. The results of the Satorra– Bentler χ2 difference test indicated that adding the direct effect of PCS on suicidal ideation (odds ratio [OR] = 0.96, p = .746, 95% confidence interval [CI] [0.76, 1.22]) did not significantly change model fit, scaled Δχ2(1) = 0.11, p = .740. Indeed, examination of the BIC for Model 2 (BIC = 4,892.76) indicated a nontrivial reduction in model fit compared with Model 1 (ΔBIC = 4.85; Raftery, 1995). Accordingly, Model 2 was rejected, and Model 1 is interpreted next (Figure 1).
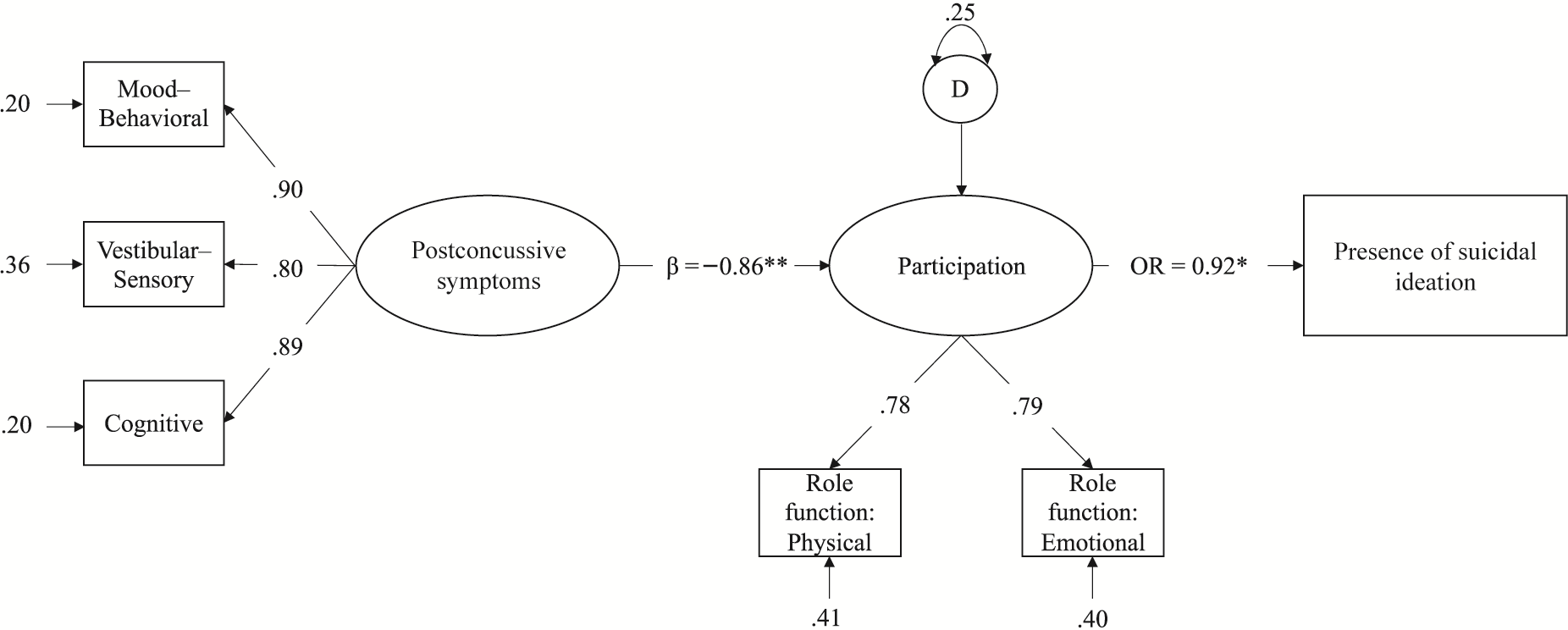
Diagram illustrating Model 1.
Model 1 supported our hypothesis that participation mediated the relationship between PCS and suicidal ideation. The indirect effect indicated that for every one-unit increase in PCS, veterans had 9% greater odds of endorsing suicidal ideation, as mediated by participation (OR = 1.09, p = .011). More severe PCS were associated with less successful participation (β = –.86, p < .001), and lesser participation was in turn associated with an increased likelihood of endorsing suicidal ideation (OR = 0.92, p = .007). Table 3 presents parameter estimates.
Discussion
In this study, we examined whether participation explained the purported relationship between PCS and suicidal ideation among veterans with mTBI. As hypothesized, the relationship between PCS and suicidal ideation was mediated by participation. More severe PCS were associated with lesser participation, and lesser participation increased risk for suicidal thoughts. Although further investigation is warranted, our results can inform a research agenda that bolsters suicide prevention efforts for veterans with mTBI by leveraging the distinct perspective of occupational therapy.
Previous studies have supported the link between PCS and suicidal thoughts or behaviors among veterans (Crocker et al., 2019) and service members (Campbell-Sills et al., 2020), but ours is the first to offer evidence that the risk posed by PCS may in part be explained by participation restrictions. This suggests that, instead of directly increasing the risk for suicidal ideation, PCS may increase risk by undermining experiences (i.e., participation) that afford reasons for living, defined as beliefs that reflect a meaningful and satisfying life (e.g., satisfactory relationships) that mitigate suicide risk (Kleiman & Beaver, 2013; Linehan et al., 1983). Indeed, prior studies of veterans have indicated that greater participation is associated with a more meaningful and satisfying life (Kinney, Graham, & Eakman, 2020; Kinney, Schmid, et al., 2020). To be clear, participation restrictions are not the only explanatory mechanism underlying the relationship between PCS and suicidal thoughts, and additional factors should be accounted for in future research. For example, neuropsychological function (e.g., processing speed) may also drive suicidal thoughts in veterans with mTBI (Crocker et al., 2019). Moreover, although our data do not support an effect of PCS on suicidal ideation that operated independently of participation, this finding may be an artifact of our relatively small sample (Kline, 2011). Future studies with larger sample sizes should further explore the direct and indirect effects of PCS on suicidal thoughts. Nonetheless, the evidenced role of participation begs for the continued advancement of research investigating participation restrictions as a risk for suicide among veterans.
Participation is central to occupational therapy practice, and thus the profession is uniquely situated to advance an understanding of participation restrictions as a risk for suicide. For example, an occupational therapy perspective on participation tends to emphasize its multidimensional nature (Hemmingsson & Jonsson, 2005), which should be explored in relation to suicide risk. In particular, the relationship between suicide risk and the meaningfulness of participation, or the extent to which it aligns with veterans’ values and interests (Cogan & Carlson, 2018; Eakman et al., 2018), should be examined. Studies of participation restrictions as a risk for suicidal thoughts, including the current study, tend to emphasize the observable aspects of participation (e.g., successful engagement) and overlook its subjective qualities. Meaningful participation reflects experiences that align with factors considered to reduce suicide risk. According to the interpersonal theory of suicide (Joiner, 2005), suicidal behavior emerges from the simultaneous presence of two states: (1) perceived burdensomeness (i.e., a belief that one burdens or is reliant on others) and (2) thwarted belongingness (i.e., lack of social connection). Meaningful participation elicits experiences such as autonomy and social connection (Eakman et al., 2018), potentially buffering against suicidality by minimizing perceived burdensomeness and thwarted belongingness, respectively. Reduced participation in meaningful activities should be further explored in relation to veteran suicide risk.
Kashiwa et al. (2017) proposed that occupational therapy practitioners can support suicide prevention efforts by enabling veterans’ engagement in daily activities; yet, before the current study was conducted, empirical support for this proposition has been scant. By revealing that participation restrictions may confer suicide risk, our study offers a foundation on which continued scientific investment can develop occupational therapy’s distinct role in multidisciplinary suicide prevention efforts. In particular, occupational therapy practitioners are adept at crafting meaningful and health-promoting experiences for clients through activity (Eakman, 2015); interventions that apply this skill set to suicide prevention should be explored. For example, Lifestyle Redesign® is an occupation-based preventive intervention that modifies older adults’ habits and routines to enable healthy patterns of time use, thereby reducing depression and improving life satisfaction (Clark et al., 1997, 2012). Suicide prevention interventions could be developed that mitigate suicide risk among veterans by embedding meaningful and health-promoting time use into their daily habits and routines.
Moreover, research indicates that PCS indirectly heighten risk for suicidal thoughts, offering empirical support for the development of prevention efforts for veterans with mTBI that manage symptoms and associated participation restrictions. Occupational therapy practitioners may mitigate suicide risk by applying compensatory approaches, thereby enabling successful engagement in role-fulfilling activity despite PCS. For example, practitioners can facilitate successful participation despite postconcussive headaches by adapting elements of the environment to avoid headache triggers (Sahai‐Srivastava et al., 2017). Moreover, occupational therapy practitioners can operate in multidisciplinary teams to directly manage PCS. For example, they can safely and effectively deliver cognitive–behavioral therapy for insomnia (Eakman et al., 2022), a recommended treatment for postconcussive sleep disturbances that are prevalent among veterans with mTBI (Cogan et al., 2019; VA/Department of Defense, 2016).
Last, our study substantiates prior calls to implement strategies to detect suicide risk in rehabilitation settings serving people with TBI (Fisher et al., 2016). Indeed, a recent study found that 16.3% of suicide decedents had received outpatient specialty care in the VHA (e.g., PCS management) within 7 days prior to the event, highlighting the need to detect suicide risk in settings beyond those that address behavioral health (Ahmedani et al., 2019). Accordingly, the VHA recently mandated a national suicide risk identification strategy: VA Risk ID (VA, 2018). Risk ID mandates universal suicide risk screening and subsequent assessment as appropriate among patients receiving VHA care, thereby facilitating appropriate follow-up evaluation and treatment as needed (Matarazzo et al., 2020). With the influx of veterans receiving care outside the VHA system (Mattocks & Yehia, 2017), and the growing rates of suicide among the U.S. population more generally (VA, 2019), it is crucial that similar strategies are adopted across health care and rehabilitative settings.
Limitations and Directions for Future Research
The cross-sectional design of this study precludes an understanding of the directionality of relationships, and the relatively small sample size diminishes the generalizability of our findings. The relationships under study should be substantiated using longitudinal designs with larger and more representative samples. Moreover, because of the small sample size, we were unable to explore the unique influences of specific PCS domains on participation restrictions and suicidal thoughts. Future research using larger sample sizes should also investigate the relative contributions of specific PCS clusters (i.e., Mood–Behavioral, Vestibular–Sensory, Cognitive). Moreover, we used a measure of participation that does not capture the multidimensionality of the construct. Using multidimensional participation measures may reveal different results and should be explored in future research. We were unable to account for all potentially confounding variables in analyses (e.g., depression diagnosis, physical conditions). It is important to note that we were able to adjust models by PTSD diagnosis, a risk factor for veteran suicide (Cooper et al., 2020). Nonetheless, future work should account for the influence of other potentially confounding variables, such as depression, or physical diagnoses, such as chronic pain (Blakey et al., 2018). In addition, this study focused on explaining suicidal ideation. Future studies should investigate other suicidal behaviors (e.g., attempts) and their relationship with PCS and participation restrictions to reveal potentially differential results. Finally, our cohort included only veterans with mTBI. Future research should include more heterogeneous samples (e.g., healthy controls) to examine differential relations among PCS, participation restrictions, and suicidal thoughts. Such research could also explore the interactive effects of mTBI and PTSD on participation and suicidal thoughts.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: Preventive interventions should be developed and tested to specifically mitigate veterans’ suicide risk by embedding meaningful and health-promoting participation into their daily routine. Occupational therapy practitioners may mitigate veterans’ suicide risk by directly managing PCS and enabling participation despite such symptoms. Settings within which veterans with mTBI are treated should adopt strategies to detect suicidal thoughts, enabling follow-up evaluation of risk factors (e.g., PCS) and appropriate treatment.
Conclusion
In this study, we examined whether participation explained the purported relationship between PCS and suicidal ideation among veterans with mTBI. The results indicate that more severe PCS are associated with lesser participation, which is in turn associated with an increased likelihood of suicidal thoughts. Given the centrality of participation to occupational therapy practice (Hemmingsson & Jonsson, 2005), our results suggest that occupational therapy practitioners can serve a distinct role in veteran suicide prevention efforts.
Footnotes
Acknowledgments
Lisa Brenner reports grants from the U.S. Department of Veterans Affairs, the U.S. Department of Defense, the National Institutes of Health, and the state of Colorado; editorial remuneration from Wolters Kluwer; and royalties from the American Psychological Association and Oxford University Press. In addition, she consults with sports leagues via her university affiliation. We report no additional conflicts of interest. We thank Paul Allison for his consultation regarding analyses. This article is based on work supported by the Veterans Health Administration, Rocky Mountain Mental Illness Research Education and Clinical Center, but it does not necessarily represent the views of the U.S. Department of Veterans Affairs or the U.S. government.