
Abstract
Medical record review of patients who received acute occupational therapy services found that higher frequency of therapy was linked with lower odds of readmission.
Readmissions after inpatient hospitalization are costly; the estimated annual cost to Medicare because of readmissions is $26 billion (Boozary et al., 2015). Readmissions are also associated with poor patient outcomes, including higher risk for mortality, nutritional concerns, and deconditioning (Fernandez et al., 2015; Krumholz, 2013; Luan et al., 2014; McIlvennan et al., 2015). To reduce readmissions, Medicare initiated the Hospital Readmissions Reduction Program (HRRP). HRRP is a value-based program that reduces reimbursement by up to 3% for hospitals that have excessive readmissions for patients with one of the following diagnoses: acute myocardial infarction, chronic obstructive pulmonary disease (COPD), heart failure (HF), pneumonia (PN), coronary artery bypass graft, and elective primary total hip arthroplasty (THA) or total knee arthroplasty (TKA; Centers for Medicare & Medicaid Services [CMS], 2021). The HRRP affects three-quarters of the hospitals in the United States (American Hospital Association, n.d.). Because reducing readmissions continues to be a top priority in the U.S. health care system, health care professions need to identify their role in this quality-focused environment. Occupational therapy has yet to clearly demarcate its role in reducing hospital readmissions. In this study, we aimed to help fill this gap.
Evidence thus far on the role of occupational therapy in reducing hospital readmissions has been minimal and somewhat fragmented. In the acute care setting, studies have linked higher spending on and use of occupational therapy services with reduced readmissions; however, a lack of quantifiable definitions of higher spending and use of occupational therapy services makes translation of the findings into practice difficult (Andrews et al., 2015; Burke et al., 2014; Rogers et al., 2017). In the clinical acute care setting, duration and frequency of services can be based on patient volume, clinician judgment, and department guidelines, which are unique to each rehabilitation department. This varied and unsystematic clinical approach to delivery of patient care results in an unknown impact on quality outcomes, including readmissions.
In contrast, evidence demonstrates that more physical therapy, defined as longer sessions (i.e., duration) and extra sessions (i.e., frequency), can reduce length of hospital stay, improve functional outcomes, and increase quality of life for patients with acute and subacute conditions (Peiris et al., 2011). Evidence in the acute care setting has also shown that longer durations (i.e., minutes) of physical therapy services for hospitalized patients after an ischemic stroke lead to lower risk of readmission (Kumar et al., 2019). Lang et al. (2015) suggested that occupational therapy service delivery factors (i.e., duration and frequency) could account for up to one-third of the variance in patient outcomes, creating a high priority area for research in the profession.
In addition, the effect of the types of occupational therapy services delivered on quality outcomes also remains relatively unexplored. There has been considerable debate about what goes on during rehabilitation sessions, giving rise to the concept of the “black box” of rehabilitation practice (DeJong et al., 2004). Evidence is limited on what goes on inside the black box and how it relates to outcomes. The current system that all acute occupational therapy practitioners use to identify, organize, and bill for the types of acute occupational therapy services delivered is Current Procedural Terminology® (CPT®) codes (American Medical Association, 2021). CPT codes are a broad representation of all the tasks and services provided by occupational therapy practitioners during a session with a patient.
In this study, we aimed to identify the impact of occupational therapy services receipt, duration, and frequency on readmissions and to compare the types of occupational therapy services delivered to patients who were readmitted versus not readmitted on the basis of CPT codes. It was hypothesized that Medicare patients with a HRRP-qualifying diagnosis who received higher duration and frequency of occupational therapy services and greater amounts of activities of daily living (ADL)/self-care training, as indicated by CPT codes, would have significantly lower odds of readmission.
Method
Design and Data
A cross-sectional, retrospective study of a large urban hospital’s data in southeastern Wisconsin was used to examine the relationship between acute occupational therapy service delivery factors and readmission as well as the differences between CPT codes for readmitted and not-readmitted patients. The source of the data was the hospital’s electronic medical record, Epic. The data were transferred from Epic to Epic Clarity, a data warehouse that allows data-intensive reports to be completed without interfering with the user-facing Epic platform (see https://www.med.upenn.edu/dac/epic-clarity-data-warehousing.html). The sampling time frame for the study was January 2014 to February 2020. The study was approved by the Medical College of Wisconsin’s institutional review board and reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (see the Supplemental Appendix, available online with this article at https://research/aota.org/ajot).
Participants
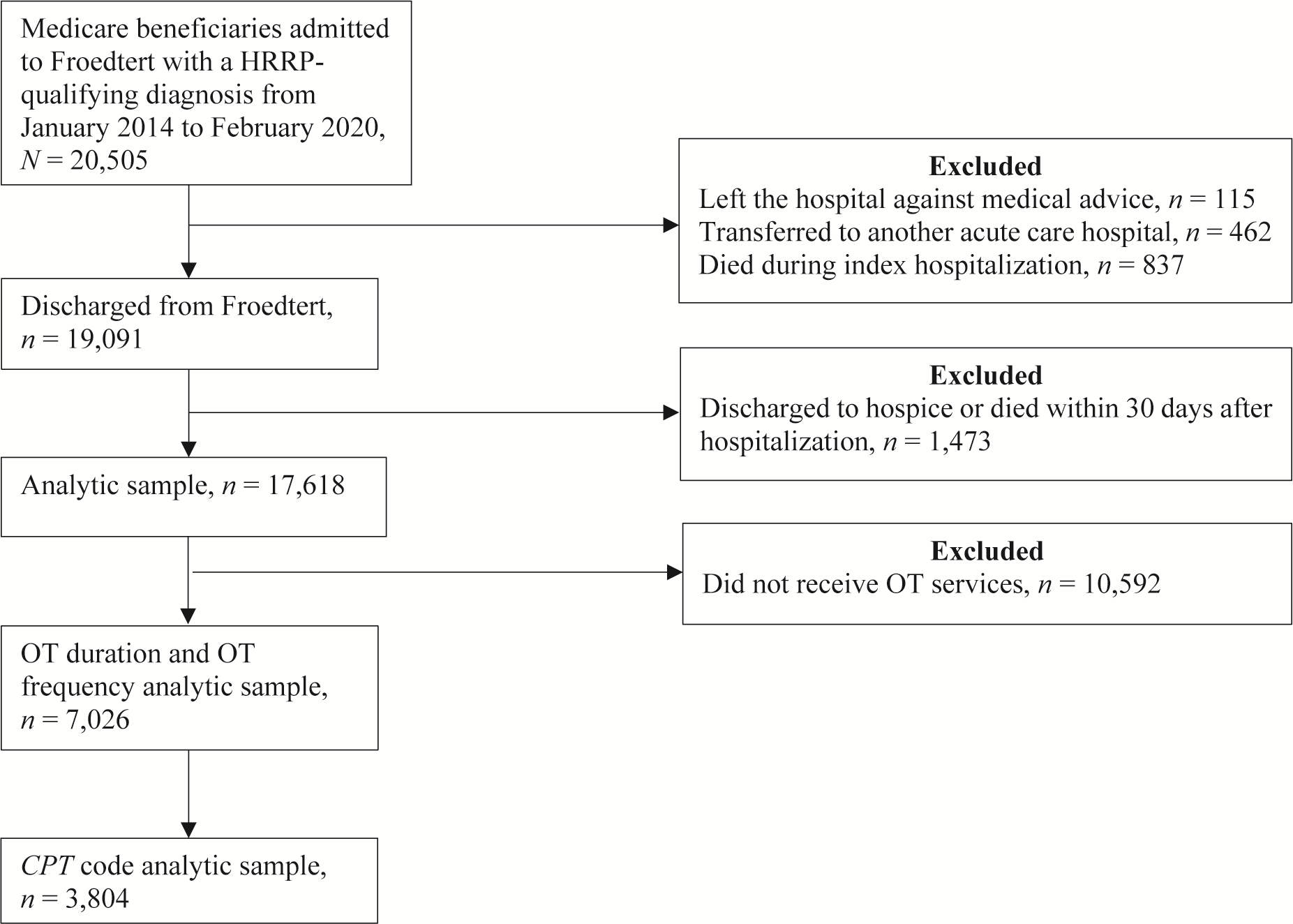
The study sample consisted of 17,618 Medicare patients with a HRRP-qualifying diagnosis. We identified HRRP diagnoses in Epic using International Statistical Classification of Diseases and Related Health Problems 10th Revision (World Health Organization, 2019) codes. Only acute care patients who were enrolled in Medicare were included. Patients who left the hospital against medical advice, transferred to another acute care hospital, died during the index hospitalization, were discharged to hospice, or died within 30 days of discharge were excluded from the sample (Figure 1). These exclusion criteria minimized the competing risk of readmission related to death because this indicator does not reflect quality of care (Kumar et al., 2019).
Cohort creation.
Key Variables
The key variables of interest were occupational therapy service delivery factors and types of occupational therapy services delivered, including (1) receipt of services, (2) duration of services, (3) frequency of services, and (4) CPT billing codes. Receipt of occupational therapy services was logged as a dichotomous (yes–no) variable and was determined by the documentation of any occupational therapy CPT treatment code. The duration variable was calculated as the mean minutes per day of occupational therapy services as follows: the total number of minutes of services during hospitalization divided by the number of days that services were delivered. Occupational therapy minutes were calculated by assigning 15 min to each treatment CPT code. Frequency of occupational therapy services was defined as the percentage of days per stay that a patient received services. The variable was calculated by dividing the number of days that services were delivered by the number of days between initiation of services, as indicated by documentation of occupational therapy CPT evaluation codes and the last day of services. The standardization of the duration and frequency variables allowed for meaningful comparisons between patients who had different lengths of stay and removed the need to control for length of stay.
We consolidated the CPT codes available for documentation into six categories using the CPT code definitions provided by the American Medical Association: (1) therapeutic exercise, (2) therapeutic procedures, (3) development of cognitive skills, (4) therapeutic activities, (5) ADL/self-care training, and (6) other (see the Supplemental Appendix, available online with this article). To isolate the effect of each intervention, we excluded patients who received interventions from more than one of the six categories of CPT codes from the analyses of CPT codes. A patient could receive multiple charges from the same CPT code category, but not different CPT code categories, and still be included in the sample used for CPT code analysis.
Covariates
To control for patient characteristics and random effects, we included the following covariates in the adjusted analyses: age, sex, race–ethnicity, postacute discharge destination, number of comorbidities, intensive care unit (ICU) stay, HRRP diagnosis, and social support (Horney et al., 2017; McIntyre et al., 2016; Pedersen et al., 2017; Silverstein et al., 2008). Age was included as a continuous variable. Sex was classified as male or female. White or Caucasian, Black or African-American, and other were the categories for race– ethnicity. Postacute discharge destinations were home health care and self-care, assisted living, intermediate care facility, nursing facility, rehab and psychiatric, and other. The variable was consolidated to create the following categories: home health care and self-care, nursing facility, and other. The Elixhauser comorbidity measure was used to create the comorbidity variable, which was presented as a continuous variable (Quan et al., 2005). The ICU stay variable was dichotomized into yes or no. The HRRP diagnoses created a categorical variable. Lastly, the social support variable was defined by whether someone was living with the patient. It was dichotomized into alone or not alone.
Outcome
The primary outcome was 30-day all-cause hospital readmission. All-cause readmissions are defined by CMS as any unplanned readmission that occurs for any cause within 30 days of discharge from the hospital. All-cause readmission is the measured outcome in HRRP. Confirmation that each readmission met CMS criteria was done by the external company Vizient (Irving, TX). The readmission variable was dichotomized into yes or no.
Statistical Analyses
Descriptive statistics were organized by readmitted or not readmitted. Three logistic regression models were estimated to examine the association between occupational therapy service delivery factors and readmission. Each logistic regression model had unadjusted and adjusted results. Adjusted models controlled for age, sex, race–ethnicity, postacute discharge destination, comorbidity count, ICU stay, HRRP diagnosis, and social support. A χ2 test compared the differences between CPT codes billed for patients who were readmitted versus not readmitted. A Fischer’s exact test compared CPT codes between groups that had small sample sizes. We performed all statistical analyses using R (Version 4.0.0; R Project for Statistical Computing, Vienna, Austria).
Results
The 30-day readmission rate for the total sample was 13% (Table 1). Patients with COPD had the highest readmission rate (14.9%), followed by patients with HF (14.8%) and PN (13.8%). Patients who were readmitted were younger (M ± SD = 69.8 yr ± 12.8 yr vs. 71.9 yr ± 12.7 yr), were more likely to be Black or African-American (31.1% vs. 25.1%), were more likely to discharge to a nursing facility or other location (i.e., assisted living facility, intermediate care facility, rehab and psychiatric, or other; 24.6% vs. 21.0%), had a higher comorbidity count (5.9 ± 3.2 vs. 4.4 ± 3.3), and were more likely to have an ICU stay (37.7% vs. 27.2%). Patients who were readmitted also had a lower duration of occupational therapy services (27.1 ± 8.3 min per day vs. 29.6 ± 10.8 min per day) and a lower frequency of services (74% ± 26% treatment days vs. 82% ± 24% treatment days).
Characteristics of Participants by Readmission Status
Note. N = 17,618. EMR = electronic medical record; HRRP = Hospital Readmissions Reduction Program; ICU = intensive care unit; OT = occupational therapy.
Of the 17,618 patients included in the analytic sample, 17,518 patients had race–ethnicity documented in the EMR.
Of the 17,618 patients included in the analytic sample, 7,026 patients received occupational therapy services.
Of the 17,618 patients included in the analytic sample, 17,729 patients had social support documented in the EMR.
Adjusted results from the receipt of the occupational therapy services model, occupational therapy duration model, and occupational therapy frequency model with the primary outcome of readmission are presented in Table 2. Patients who received occupational therapy services had significantly higher odds of readmission (odds ratio [OR] = 1.18, 95% confidence interval [CI] [1.07, 1.31]). Patients who received higher frequencies of services had significantly lower odds of readmission (OR = 0.99, 95% CI [0.99, 1.00]). Patients who received higher durations of services did not have significantly higher or lower odds of readmission.
Estimated Adjusted Models of the Association Between OT Received, OT Duration, and OT Frequency and 30-Day All-Cause Hospital Readmission
Note. CI = confidence interval; HRRP = Hospital Readmissions Reduction Program; ICU = intensive care unit; OR = odds ratio; OT = occupational therapy; ref = reference category.
Only the adjusted results are presented.
p < .05.
p < .01.
p < .001.
Younger age and higher comorbidity count were both significantly associated with increased odds of readmission across all three models (see Table 2). Conversely, patients who had the diagnoses of THA and TKA had significantly lower odds of readmissions across all three models. Patients who were discharged to a nursing facility; had an ICU stay; or had a primary diagnosis of COPD, HF, or PN had significantly higher odds of readmission in the occupational therapy received model. ICU stay was also significantly associated with increased odds of readmission in the occupational therapy duration model. Race, sex, and social support were not statistically significant in any of the three models.
Results of the χ2 analyses and Fisher’s exact tests comparing the occupational therapy CPT codes for readmitted versus not-readmitted patients with HRRP-qualifying diagnoses are presented in Table 3. A higher proportion of not-readmitted patients received ADL/self-care training (80.6% vs. 74.9%; p = .005). Conversely, a higher proportion of readmitted patients, in comparison with patients who were not readmitted, received therapeutic exercise (4.3% vs. 1.7%; p < .001).
Comparison of CPT Codes Billed for Patients Who Were Readmitted Versus Not Readmitted
Note. N = 3,804. ADL = activities of daily living; CPT = Current Procedural Terminology ®.
Discussion
Reducing readmissions and the associated poor patient outcomes and high costs is a top priority in the U.S. health care system and, accordingly, is the target of HRRP (McIlvennan et al., 2015). In this study of more than 17,000 Medicare patients with HRRP-qualifying diagnoses, we found that receipt of occupational therapy services in the hospital was associated with higher odds of readmission; however, patients who received acute occupational therapy services had reduced odds of readmission if they received higher frequencies of those services while hospitalized. In addition, patients who were not readmitted to the hospital received more ADL/self-care training than patients who were readmitted to the hospital. These results provide important guidance on how occupational therapy services can be leveraged to reduce readmissions.
It is not surprising that the isolated examination of receipt of occupational therapy services was associated with higher odds of readmission. Patients who receive occupational therapy services while hospitalized appear to be older, have a higher number of comorbidities and chronic conditions, and be discharged to a location other than home (Andrews et al., 2015). All of these demographics are known to be associated with higher readmission risk (Horney et al., 2017; Pedersen et al., 2017; Silverstein et al., 2008). Including functional status in the analyses would have helped to clarify the relationship between receipt of occupational therapy services and readmissions. Impaired functional status is known to be associated with higher risk of readmission and consequently is the reason that occupational therapy services are used in the acute care setting (Middleton, Downer, et al., 2018; Middleton, Graham, & Ottenbacher, 2018). However, large amounts of data on functional status were missing at the study site, making it impossible to include functional status as a variable in the analyses.
This barrier is common when investigating the relationship between acute occupational therapy services and outcomes. In the acute care setting, no universal or required standardized measure of functional status exists. As a result, documentation on functional status is at the discretion of individual occupational therapy practitioners and facilities. Future studies should consider implementation of a standardized measure of functional status at the study site to ensure that all potentially confounding variables can be included in the study.
Higher frequencies of occupational therapy services, but not higher durations of services, were associated with reduced odds of readmission for the patients in our study. Our findings are novel because the unique impact of frequency of services on outcomes has yet to be evaluated. Only the combined impact of frequency of occupational therapy and physical therapy services has been shown to reduce readmissions and death (Freburger et al., 2020). Our findings indicate that for each 10% increase in the frequency of treatment days, the odds of readmission were 1% lower. The insignificant finding on duration of services is consistent with the limited literature on the topic. Kumar et al. (2019) found that only higher durations of acute physical therapy services, not acute occupational therapy services, were significantly associated with reduced readmission risk. Our findings suggest that frequency of occupational therapy services may play a more important role in improving patient outcomes than duration of services.
The ORs for comorbidity count (OR = 1.12), as well as for THA and TKA (OR = 0.42), demonstrated a stronger association with readmission than the occupational therapy frequency variable (OR = 0.99). However, the importance of our findings should not be diminished. Comorbidity count and the diagnosis of THA or TKA are not modifiable factors, but occupational therapy frequency is a modifiable service delivery factor. To reduce readmissions, actionable items must be identified and leveraged. Our findings demonstrate that when patients are seen by occupational therapy practitioners more frequently while hospitalized, their odds of readmission are lowered. Future studies may want to explore exact dosage for frequency of services to identify the optimal frequency associated with reduced readmission risk for patients. Evidence on exact dosage would lead to best practice guidelines that optimize patient outcomes in the acute care setting.
In our study, we found that patients who received occupational therapy services and who were not readmitted received a significantly higher amount of ADL/self-care training while hospitalized compared with patients who were readmitted, according to CPT codes. Identifying the importance of ADL and instrumental activities of daily living (IADL) interventions, not only impairments with ADLs and IADLs, in preventing readmissions is a notable finding for the occupational therapy profession because ADLs and IADLs are uniquely within the scope of occupational therapy practice. The occupational therapy CPT code for ADL/self-care training includes interventions focused on ADLs, IADLs, and fall prevention education. In the postacute setting, impairments with ADLs/self-care, increased dependency in IADLs, and experiencing a fall after hospitalization have been shown to be associated with increased likelihood of readmission (DePalma et al., 2013; Galet et al., 2018; Greysen et al., 2015; Middleton, Downer, et al., 2018; Middleton, Graham, & Ottenbacher, 2018; Pisani et al., 2018).
Future studies should seek further clarification of the exact occupational therapy activities and interventions provided by occupational therapy practitioners according to CPT codes because the American Medical Association’s definitions for CPT codes allow for wide interpretation by clinicians. Last, more complex intervention profiles for patients organized by CPT codes are needed to accurately reflect acute care practice. In future studies, researchers should consider examining the interaction effects of different occupational therapy services on readmission risk or focus on investigating the specific impact of ADL/self-care training on readmission risk.
Study Limitations
Our study had several limitations. First, the occupational therapy services provided variable only included patients who had one service provided (i.e., one type of CPT code billed) for the entirety of the patient’s hospital stay. This approach reduced the sample size (n = 3,804) for the analyses by 54%. In addition, it may not be truly reflective of practice because multiple occupational therapy services can be provided to a single patient during their hospital stay. However, this approach allowed us to isolate the impact of a single occupational therapy service on readmission risk and minimize the confounding effects of receiving multiple services.
Second, because of the broad nature and lack of standardized guidelines available for occupational therapy practitioners to use when submitting CPT codes, it is unclear which specific occupational therapy interventions occurred when the ADL/self-care training CPT codes were submitted.
Third, each treatment CPT code was assigned the value of 15 min for the analysis of duration of occupational therapy services, producing only an estimate of minutes spent by practitioners in delivering services.
Fourth, generalizability of our study is limited by the data source and sample characteristics. The data originated from a single hospital and included only Medicare patients. Therefore, findings may not be generalizable to all settings where acute occupational therapy services are provided, non-Medicare patients, or Medicare patients who do not have a HRRP diagnosis.
Fifth, only within-system hospital readmissions were captured. Out-of-system readmissions were not available in the data source.
Finally, several covariates that could have confounded results were not included in the analyses because of data limitations, including patients’ functional status, dual eligibility for Medicare and Medicaid, additional therapy received in postacute care settings, cognitive status, and housing instability. These covariates may be options for future studies.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice: Occupational therapy practitioners in the acute care setting may consider delivering higher frequencies of occupational therapy sessions for patients while hospitalized to improve their outcomes, including reduced risk of readmission. Occupational therapy practitioners in the acute care setting may want to focus sessions on ADL/self-care training for patients who are at high risk for readmission.
Conclusion
The findings of our study indicate that patients with HRRP-qualifying diagnoses who received occupational therapy services at higher frequencies had lower odds of readmission. In addition, patients who received occupational therapy services and who were not readmitted received more ADL/self-care training during sessions than patients who were readmitted. These findings help to further define occupational therapy’s unique role in reducing readmissions and may contribute to future work on evidence-based practice guidelines for improving patient outcomes.
Supplemental Material
Supplementary material for Higher Frequency of Acute Occupational Therapy Services Is Associated With Reduced Hospital Readmissions
Supplementary material, sj-docx-1-aot-10.5014_ajot.2022.048678.docx for Higher Frequency of Acute Occupational Therapy Services Is Associated With Reduced Hospital Readmissions by Jessica Edelstein, Rebekah Walker, Addie Middleton, Timothy Reistetter, Kelli Williams Gary and Stacey Reynolds in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This article was written as part of the requirements for Jessica Edelstein’s doctoral degree at Virginia Commonwealth University. We thank Sneha Nagavally (Medical College of Wisconsin) for her assistance with creating the analytical data set and statistical support for this project as part of her regular employment. In addition, we thank Erin DeJarlais (Froedtert Hospital) for her expertise in navigating the Froedtert Hospital health system when conducting research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.