
Abstract
Among women with breast cancer–related symptoms 5 years after diagnosis, this study highlights the value of a comprehensive assessment of daily participation in activity domains and individual meaningful activities to provide a deeper understanding of the associations among long-term symptoms, participation restrictions, and coping strategies.
Breast cancer (BC) is the most common type of cancer among women, but it has a high survival rate (American Cancer Society, 2020). After surviving BC, women cope with disease- and treatment-related medical, physical, cognitive, and emotional symptoms (Runowicz et al., 2016) that sometimes worsen over time (Chopra & Kamal, 2012). These symptoms directly affect their participation in meaningful daily activities and quality of life in the short (Loubani-Hawaita et al., 2016; Lyons et al., 2015) and long (Sleight, 2017) terms.
Research has documented post-BC participation restrictions in self-care, leisure, social activities (Fleischer & Howell, 2017; Sleight, 2017), and maintenance of working hours (Sun et al., 2017). However, studies that have comprehensively examined long-term changes in participation patterns for meaningful daily activities and routines, or symptoms associated with these changes, are scarce (Harrington et al., 2010; Sleight, 2017). Moreover, retaining participation in meaningful activities has been found to be important in enhancing BC survivors’ perceptions of being healthy and capable (Ashworth, 2014), mostly in the subacute phase (2 yr after diagnosis; Fleischer & Howell, 2017; Loubani-Hawaita et al., 2016). However, there is a lack of information regarding strategies women use to cope with these functional limitations (Sleight, 2017). Most studies that have examined women with BC addressed only one aspect—for example, the number of activities in which a person engages (Lyons et al., 2015), activity levels retained after a change in health status (Lyons et al., 2013), perceived performance and performance satisfaction (Newman et al., 2019), and the value women attribute to the activities (Keesing & Rosenwax, 2011).
Extending knowledge about BC survivors’ participation may contribute to the development of interventions that offer women tools to manage postdiagnosis short- and long-term restrictions in participation. Therefore, to deepen the understanding of long-term symptoms and participation restrictions of women with BC, in this study we used a comprehensive approach to measure participation. We had three aims: (1) compare women’s participation in daily activities during the subacute and chronic (5 yr after diagnosis) phases, (2) explore factors associated with participation in daily activities in the chronic phase, and (3) describe strategies women use to manage the effects of symptoms on daily participation.
Method
Design and Participants
Participants in this descriptive longitudinal study were 30 women in the chronic BC phase recruited from a cohort of 60 women who had taken part in a previous study (Loubani-Hawaita et al., 2016). Of the members of that cohort, 30 were excluded (8 had died, 11 had a BC recurrence, and 11 declined to participate). The inclusion criterion was a diagnosis of invasive ductal carcinoma Stages 1 to 3; exclusion criteria were a cancer recurrence or a diagnosis of an unrelated neurological or orthopedic condition that might affect participation in daily activities.
Measures
Personal and Breast Cancer Characteristics and the Perceived Symptoms Questionnaire
The Perceived Symptoms Questionnaire was developed on the basis of our clinical experience and qualitative research among people with cancer and has been used in other studies (Loubani-Hawaita et al., 2016; Loubani et al., 2022). The questionnaire inquires about the severity of physical (pain, fatigue, weakness, peripheral neuropathy) limitations in range of motion (LROM; upper extremity on the side of the affected breast) and cognitive (memory and attention deficit) and emotional (depression, anxiety, decreased self-perception) symptoms on a scale that ranges from 0 (no symptoms) to 4 (high severity).
Activity Card Sort
The Activity Card Sort (ACS; Baum & Edwards, 2001) assesses self-reported participation in 88 everyday activities in four domains: (1) instrumental activities of daily living (IADLs), (2) sociocultural activities, (3) leisure activities with low physical demands, and (4) leisure activities with high physical demands. We used the first version of the ACS that was adapted for use with Israeli populations (Katz & Hartman-Maeir, 2001). On the basis of data from a previous study (Loubani-Hawaita et al., 2016), women in the current study sorted each activity into one of three categories with different weighted scores: (1) Done Before Diagnosis (score = 1, from the previous study), (2) Not Done Before Diagnosis (score = 0, from the previous study), and (3) New Activity Since Diagnosis (score = 1, for the current study, i.e., an activity not done before diagnosis). In the current study, women further categorized activities in the Done Before Diagnosis category into Continued to Do During Illness (score = 1; we clarified to the women that “illness” relates to the period since the previous meeting during the subacute phase); Doing Less Since Illness (score = 0.5), reflecting reduced participation; or Given Up Due to Illness (score = 0). Each woman’s total and domain retained activity level (RAL) was calculated as the weighted sum of current activities assessed at the subacute or chronic phase (i.e., during the study) divided by past activities (i.e., prediagnosis) scores (reported by Loubani-Hawaita et al., 2016).
Canadian Occupational Performance Measure
The Canadian Occupational Performance Measure (COPM; Law et al., 1990) is a semistructured interview that measures self-perceptions of performance in self-care, productivity, and leisure. Respondents rate five meaningful daily activities on a 10-point scale to indicate their perceived performance capacity and satisfaction, producing two total average scores (Performance and Performance Satisfaction) for those activities. Higher scores indicate higher performance and satisfaction. For both measures, the cutoff score for clinically significant change is 2 points (Carswell et al., 2004). In this study, the women rated the same five meaningful activities they had identified in the subacute phase in Loubani-Hawaita et al.’s (2016) study.
Data Collection
The Ethics Committees (Helsinki Committee) of Clalit Health Services and the University of Haifa approved this study. All women provided informed consent, and all names presented herein are pseudonyms. They completed the questionnaires and answered one open-ended question: “How were you able to retain your participation in daily activities despite the long-term effects of BC?” We probed for elaboration on the responses, for example, regarding strategies used. An occupational therapist met with each woman privately in a location the woman chose. Each meeting lasted about 1 hr. Recruitment and data collection lasted 6 mo.
Data Analysis
We analyzed the data with SPSS (Version 25) and verified normal distribution with a Shapiro–Wilk test. The Wilcoxon signed-rank test was used to compare symptom severity and performance and satisfaction (COPM; 2 women did not report on their meaningful activities) in the subacute- and chronic-phase assessments. We used paired t tests to compare total RALs (ACS) in the subacute and chronic phases and a repeated-measures multivariate analysis of variance to make comparisons among the four domains in both phases (excluding one high-RAL outlier). Spearman’s ρ correlations between personal and BC characteristics, symptom severity, and participation were computed.
We transcribed the qualitative data verbatim while ensuring participant anonymity. We analyzed the interviews using the phenomenological content analysis method; specifically, we coded the data, categorized them into groups, and identified commonalities and differences among the women’s experiences with the aim of identifying major themes. Loubani and Schreuer performed the text analysis inductively and undertook thick description and validation by a few participants to ensure trustworthiness (Creswell & Poth, 2016). We then focused on the theme of coping strategies the women used.
Results
The personal and disease characteristics of the women, none of whom received occupational therapy during the study, are presented in Table 1. The data in Table 2 describe and compare symptom severity between women in the subacute and chronic phases. A statistically significant symptom reduction was seen only in the physical domains; more than 53% of the women reported that their emotional and cognitive symptoms increased or remained unchanged in the chronic phase.
Participants’ Personal and Disease Characteristics
Note. N = 30.
Some women received more than one type of therapy.
Symptom Severity Comparison: Subacute and Chronic Phases
Note. N = 30. IQR = interquartile range; LROM = limitation in range of motion of the upper extremity.
Range = 0–4.
Participation: Chronic Versus Subacute Phases
Significantly higher total RALs were found in the chronic phase (M = 0.93, SD = 0.27) compared with the subacute phase (M = 0.71, SD = 0.22), t(29) = 4.72, p = .0001. Significantly higher RALs for IADLs, F(1, 28) = 14.79, p = .001, ηp 2 = .35, and sociocultural domains, F(1, 28) = 27.92, p = .0001, ηp 2 = .50, were found in the chronic phase compared with the subacute phase. No differences were found for high RALs, F(1, 28) = 2.14, p = .154, ηp 2 = .07, or low RALs, F(1, 28) = 4.05, p = .054, ηp 2 = .13, in the physical demand leisure domains (Figure 1).
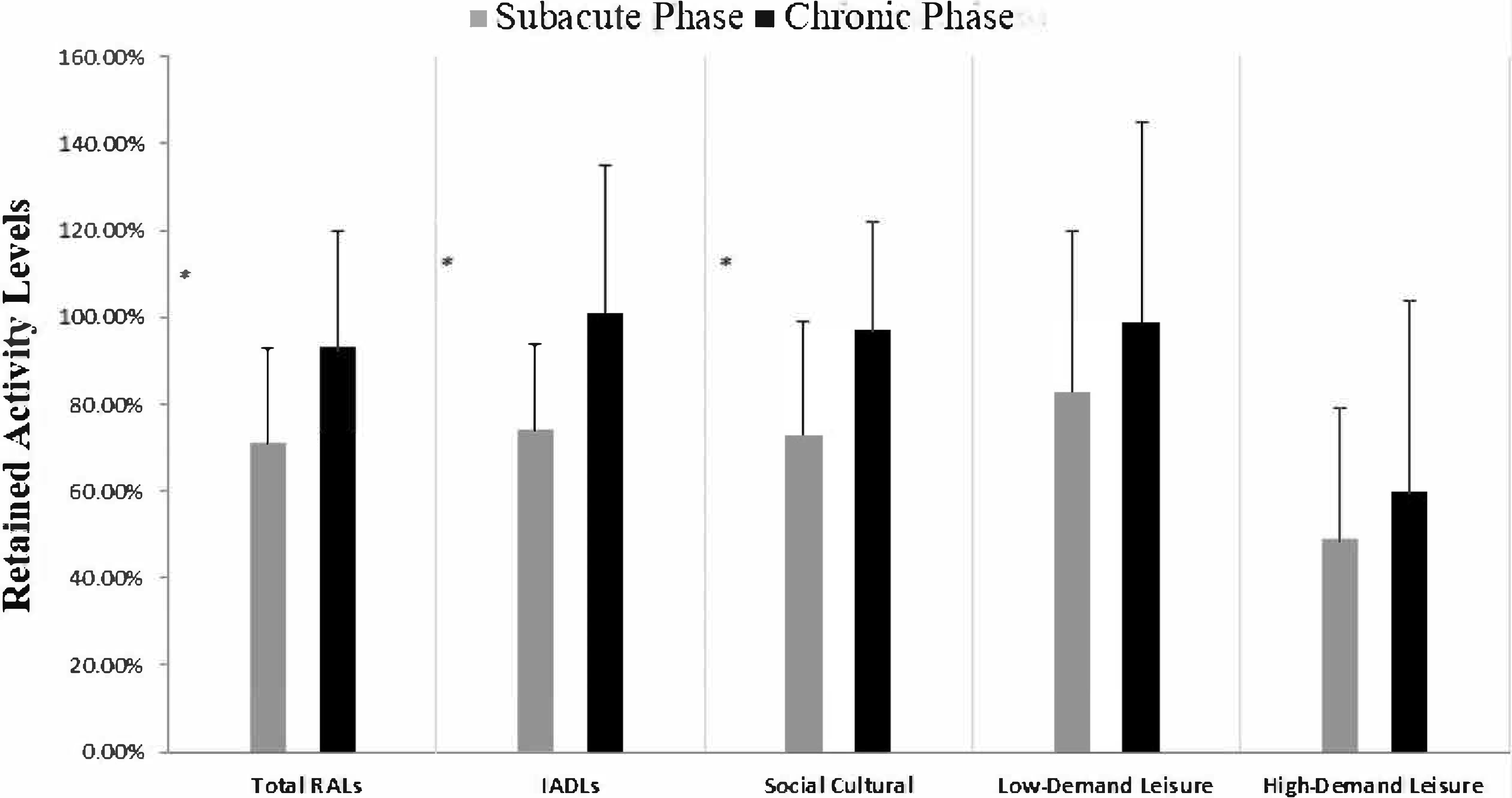
Retained activity level comparison: Subacute and chronic phases with prediagnosis phase.
We noted statistically significantly higher perceived performance of five activities in the chronic phase compared with the subacute phase (chronic phase, Mdn = 7.70, interquartile range [IQR] = 6.21–9.36; subacute phase, Mdn = 6.80, IQR = 4.85–8.00; z = –2.48, p = .013). Similar results were noted in performance satisfaction (chronic phase, Mdn = 7.90, IQR = 6.13–9.65; subacute phase, Mdn = 5.90, IQR = 4.70–7.85; z = –3.51, p = .0001). Eleven (39%) of the 28 women who reported on their meaningful activities women achieved clinically detectable improvement in their perceived performance; 10 (36%) improved, but without a clinically detectable change; 5 (18%) perceived a decrease; and 2 (7%) experienced no change. In regard to satisfaction, 12 (43%) achieved clinically detectable improvement; 12 (43%) others increased, but without clinically detectable improvement; and 4 (14%) perceived a decrease.
Factors Associated With Participation in the Chronic Phase
Lower symptom severity was associated with ACS: higher total RALs (LROM, r = –.43, p = .018; physical, r = –.71, p = .0001; emotional, r = –.44, p = .015; cognitive, r = –.51, p = .004), higher IADL RALs (LROM, r = –.53, p = .003; physical, r = –.67, p = .0001; cognitive, r = –.53, p = .003), higher low- physical-demand RALs (physical, r = –.56, p = .001; cognitive, r = –.42, p = .022), and higher high-physical-demand RALs (physical, r = –.58, p = .001). In addition, lower symptom severity was associated with higher performance on the COPM (cognitive, r = –.40, p = .036) and higher performance satisfaction (r = –.38, p = .045). Among BC characteristics, chemotherapy was associated with lower IADL RALs (r = –.50, p = .001). No other significant correlations were found between personal, demographic, or BC characteristics and ACS or COPM score in the chronic phase.
Qualitative Findings
The preliminary qualitative analysis revealed 49 codes, which we merged into 12 subcategories. We ended up with four main themes that reflected the women’s processes to manage daily activities in the chronic phase: (1) women’s perceptions of and coping with BC, (2) implications of difficulties for participation in routine activities, (3) importance of maintaining daily activities and routines, and (4) strategies to maintain meaningful activities. In this article, we focus on the fourth theme to demonstrate three strategies participants used to manage daily activities.
Reframing the Situation and Adopting Positive Thinking
Most of the women described using internal resources to choose to appreciate what they had, listen to their needs, and self-talk to put themselves in the center: I learned to place awareness above the situation, taking care of myself. . . . I have my own ways . . . I will not fall down; I will not break. I have children . . . I will not be led by misery. . . . It's not me. (Katy)
Ehlam added active and positive perception: “Why think negatively? I could die, get sick. . . . I gained a new perspective [on] life; I decided to continue my life and live the years that I have left with joy.”
For others, the threat of the BC’s recurrence that had affected their life perspectives and priorities also changed their behaviors and activities: “If I used to be afraid of missing something, I do not waste time worrying; now, I enjoy every moment” (Naama). Most of the women mentioned how engaging in meaningful activities, such as work and creative hobbies, helped them feel more vivid and healthier and helped distract them from the BC treatment and symptoms: “During the treatments, I didn’t stay home; I went to work to not think about the illness” (Gili).
Changing Schedules and Priorities
To save energy and maintain health, the women reported changing their weekly schedule and priorities: In my daily life, I learned to release, to delegate authority, what can be postponed [until] tomorrow . . . to postpone [until] the day after tomorrow. . . . My point of view has changed. . . . If I feel tired, then rest. . . . If I do not have the energy to meet people, I do not do this! [My] life [priorities changed] . . . family over work, health precedes all. (Caroline)
Others described how they changed their habits and strategy to manage housework but save energy. For example, Dina integrated rest periods into her housework activities: “I must rest after . . . pain appears, especially when performing housework.” Similarly, Amal said, “As for hard housework, I divided it into several stages or days.” Others reduced their weekly working hours, switched to less stressful jobs, or quit altogether: “I changed my workplace, listened to my heart, [went to] a place of work that has less stress, pressure, and responsibility” (Caroline). Tania retired from leading projects in a large company: “Retirement came after work required more time at the expense of [my] health, and I felt sucked back into the overload of work.”
Accepting Help
Another strategy the women used was to ask for and accept help from others at home and at work. Although it was not easy, most relied on their family or paid help to cope with domestic chores: “I found strategies, waiting for my daughter to prepare food, like slicing meat, distributing portions in advance, and a housemaid once a week” (Hadar). At work, the women accepted help from their colleagues, according to their current limitations, to share the physical and cognitive burden. Caroline, a kindergarten teacher, demonstrated this strategy to meet physical burdens: “I do not lift the children at work; I use the team or my left hand.” Others used such support to meet cognitive challenges: “At work, too, [I was] forgetting things but using a very thoughtful team, a very supportive and understanding work environment, [that] helped to divide the burden of work” (Amal).
In summary, the women adopted new strategies, habits, and support to continue carrying out their daily activities to suit their current needs and capabilities. Interestingly, they mentioned relying more often on informal, rather than formal, support.
Discussion
In this follow-up study, we aimed to examine women’s participation in daily activities during their chronic compared with subacute BC phase. An additional aim was to examine factors associated with chronic-phase participation. Overall, except in physical domains, the findings revealed notable improvements in RAL, performance, and satisfaction with performing meaningful activities. Improved participation occurred despite long-term physical, cognitive, and emotional symptoms. Nevertheless, symptom severity was associated with RAL.
These findings align with those of previous studies in that they highlight the associations of chronic physical (Chopra & Kamal, 2012), emotional (Saeedi et al., 2019), and cognitive (Selamat et al., 2014) symptoms with long-term restricted participation (Sleight, 2017). The women’s participation as reflected in their performance on the ACS (RAL) and COPM improved in the chronic phase; however, in some domains it remained lower than their pre-BC scores or did not reach maximal scores. The qualitative data showed that the women reframed their perceptions to emphasize appreciation, optimism, winning, and overcoming the disease and to avoid negative thoughts, which helped them maintain their participation. This approach, and perhaps the fact that the women in this study did not have active BC, enabled them to flexibly use adaptive coping strategies (Nes & Segerstrom, 2006) to manage symptom effects on their day-to-day activities. Despite residual symptoms, participants’ IADLs improved. This may be explained by the high value women attribute to being self-sufficient and productive and not being a burden on their families (Pergolotti et al., 2020). Moreover, successful participation in such an essential domain, as well as social participation, helps maintain a sense of normalcy (Keesing & Rosenwax, 2011). The activities women chose as meaningful (on the COPM) and the qualitative data—in which they focused on returning to care for their families, household, and jobs—reinforce this finding.
The women’s participation in the social activities domain improved, but in the chronic phase it did not correlate with any symptom. Among external factors affecting participation, especially in daily social activities, were family and informal social support (Manning-Walsh, 2005). Such support facilitates the posttraumatic recovery process and provides a strong sense of self-efficacy (Benight & Bandura, 2004). The women’s ability to return to their social activities and the finding that personal characteristics and symptoms were not barriers to participation may have two explanations. First, the qualitative data showed that the women in this study used compensatory strategies that involved their close family and work environment, which may indicate high social support. Such support helped them manage their difficulties and retain social participation (Manning-Walsh, 2005). Second, the sample’s high education level points to moderate or high socioeconomic status, which might affect their external resources to maintain activities. Indeed, the theory of fundamental causes can explain the association between socioeconomic status and mortality and indicates that socioeconomic resources such as money, knowledge, power, and social connections protect health and reduce mortality among women with BC (Phelan et al., 2010).
As in other studies, the women expressed particular difficulty in returning to activities that have a high physical demand (e.g., walking, sports, traveling) that may contribute to health generally and for cancer patients specifically (Kapoor, 2013; Rogers et al., 2017). This difficulty might relate to residual physical symptoms, such as pain and fatigue, that may hinder performance (van Weering et al., 2007). Qualitative data showed that the women chose to be active and manage their meaningful daily routines. Nevertheless, despite their strategies to prevent fatigue and damage to the hand on the side of the affected breast (e.g., splitting up daily tasks or accepting help), the women did not reach the same level of participation they had before BC, especially in activities with high physical demands (Kapoor, 2013).
The lack of improved participation in leisure activities with low physical demands (e.g., cooking as a hobby or reading) in the chronic phase may be explained by this domain’s relatively high RAL in the subacute phase. It also may be due to cognitive symptoms, such as memory or attention difficulties. Memory and attention deficits are known obstacles to returning to full participation in daily activities, especially those that rely on the ability to multitask, which often is required for in-home leisure activities (Selamat et al., 2014). This finding may also be attributed to both cognitive and physical symptoms because some activities in this domain rely on a combination of motor–cognitive abilities. The cognitive strategies women used in the current study seemed to enable them to overcome the cognitive difficulties, such as multitasking in several daily contexts; for example, in line with previous studies, women changed their life priorities, planned and balanced their daily activities according to their limitations, and used colleagues’ help to reduce the work burden (Lyons et al., 2015).
We were surprised to find that, unlike in other studies (Saeedi et al., 2019), the women in the current study mentioned only slight emotional difficulties dealing with BC: Five yr after diagnosis, most feared only a recurrence. Nevertheless, emotional difficulties did not correlate with their participation. Perhaps at this chronic stage they already had undergone a process of adjusting to their BC diagnosis and its implications and they coped more through active problem-focused than emotion-focused strategies (Fleischer & Howell, 2017).
Study Limitations
This study excluded women whose BC had recurred and women with other severe neurological or orthopedic medical conditions. We did not query about cardiovascular conditions, which are a known consequence of BC medical treatments. Therefore, the findings do not reflect the experiences of women with active cancer, poor health, or a lack of support. The sample was small, and some insignificant results with moderate to large effect size (e.g., leisure RALs with a low physical demand) may reach significance with a larger sample. In addition, this sample’s personal characteristics (e.g., high education level) do not represent all BC survivors. In accordance with Phelan et al. (2010), who discussed associations between inequalities and health outcomes, future studies should recruit larger samples with diverse socioeconomic status and examine the relationships of socioeconomic characteristics with participation. Moreover, future studies may wish to include standard assessments of emotional and objective executive function and combine them with physical assessments.
Implications for Occupational Therapy Practice
This study shows the trajectory of participation’s multidimensional aspects and the complexity of long-term BC-related symptoms. Our findings highlight the need for occupational therapy practitioners to integrate a comprehensive occupation-based assessment and intervention into current cancer treatment practice, which thus far has focused mainly on medical and psychological aspects. These assessments and interventions should recognize the need for functional– cognitive evaluations so cognitive difficulties can be managed with appropriate strategies and participation restrictions in the short and long term can be prevented (Joly et al., 2019). In addition, interventions should focus on adopting health-promoting habits, including physical activity (Rogers et al., 2017), to reduce symptoms (Lahart et al., 2018), prevent cancer recurrence (McTiernan, 2018), and promote meaningful daily participation. Evidence for the effectiveness of occupational therapy interventions (Lyons et al., 2015; Newman et al., 2019) is increasingly showing that occupational therapy practitioners play an important role in reducing disease consequences by focusing on active engagement in meaningful activities that improve quality of life (Petruseviciene et al., 2018).
Conclusion
Interactions among residual long-term symptoms (physical and cognitive) restricted women’s participation in daily activities 5 yr after diagnosis. Our use of quantitative and some qualitative data contributed to a deepened understanding of the coping strategies women use to maintain their daily activities after BC. Overall, the results reinforce the need for early occupational therapy intervention, which recent studies have shown is effective but was not part of the care any woman in the current study received. Such early intervention should focus on managing participation in daily activities by targeting the physical and cognitive symptoms associated with BC and its medical treatment.
Footnotes
Acknowledgments
We report no declarations of interest. Naomi Schreuer and Rachel Kizony contributed equally to this article. This study was supported by a research grant (20120072-C) from the Israeli Cancer Association. It received the approval of the ethics committee of the University of Haifa (No. 1503) and the ethics committee (Helsinki Committee) of Clalit Health Services (No. 0043-16-COM2).