
Abstract
This systematic review found that additional occupational therapy interventions can be effective in reducing readmissions among some adult hospitalized patient populations, including those admitted for surgery or management of acute medical conditions; stronger evidence supports transitional care interventions.
Hospital readmission is recognized as a problem because it affects the health and well-being of patients and represents a financial burden to the health system. Hospital readmissions have become a focus of policymakers in an effort to control costs and improve the quality of care (Kristensen et al., 2015). In recent years, policies have been developed with the aim of reducing readmissions (Centers for Medicare & Medicaid Services, 2021; Kristensen et al., 2015; NHS [National Health Service] England & NHS Improvements, 2017). In the United States, the Hospital Readmission Reduction Program was introduced to encourage hospitals to improve communication and care coordination to reduce avoidable readmissions (Centers for Medicare & Medicaid Services, 2021). Other initiatives have included moving from volume-based care (fee for service) to value-based care (fee for value) to provide incentives for health care providers to offer the best care at the lowest cost (Medicare Payment Advisory Commission, 2021). As preventable readmissions continue to gain attention as a key quality indicator for hospital care, health care providers need to better understand what contributes to minimizing risk of poor outcomes. As part of this effort, occupational therapy practitioners must recognize and link their specific contribution to facility and system outcomes (Lamb & Metzler, 2014).
Hospital readmission can have a substantial impact on both patients and the health care system. For patients, hospital readmissions have been associated with worsening prognosis, reduced quality of life, and increased mortality (Covinsky et al., 2003; Lum et al., 2012). For the health care system, readmissions are costly and involve use of resources that could have potentially been avoided. It has been estimated that 90% of readmissions are unplanned (Jencks et al., 2009). Unplanned all-cause hospital readmission rates among adults are approximately 15% to 20% across acute, postacute, and mental health settings (Benjenk et al., 2020; Jencks et al., 2009; Smith et al., 2017; Vashi et al., 2013). However, variations occur across hospitals and patient characteristics (Benjenk et al., 2020; Goodman et al., 2011). One study of Medicare recipients estimated that unplanned readmissions to the hospital within 30 days cost more than $26 billion per year (Jencks et al., 2009). Another study of patients with atherothrombotic disease found that readmissions within the first 12 mo after discharge cost $17 million and constituted one-third of total hospital costs in the 2-yr period after the index admission (Atkins et al., 2014).
Several studies in recent years have suggested that the combination of financial pressure, performance reporting, and research effort has contributed to a reduction in unplanned readmissions (Chen & Grabowski, 2019; Hoffman & Yakusheva, 2020; Lu et al., 2016; Westley-Wise et al., 2020; Zuckerman et al., 2016). Although many unplanned readmissions to the hospital are not preventable, one recent systematic review of 34 studies reported that the median proportion of readmissions deemed to be avoidable was 27% (van Walraven et al., 2011). However, within that study, a range of 5% to 79% was reported, suggesting the difficulty in determining the level of preventability. Nonetheless, understanding how to reduce avoidable hospital readmissions has the potential to support better health outcomes for patients, improve patient safety, and lead to greater efficiency in the health system.
With ongoing resource pressures on modern health services, it is important that professions understand and justify their contribution to clinical outcomes. An article by Roberts et al. (2020) highlighted key areas where occupational therapy practitioners can add value to the effort to keep people out of the hospital and participating in their lives by focusing on patients’ functional and social needs. Occupational therapy practitioners working with adult patients in hospital settings look broadly at whether they are safe and have the skills, abilities, and appropriate support in place as they transition to their prehospital environment. Practitioners’ aim is to achieve a successful community discharge by supporting a patient at home and keeping them there without a readmission to the hospital (Xian et al., 2015). Thus, the readmission rate of adult hospitalized patients after discharge is a relevant outcome measure for occupational therapy practitioners working in hospital settings.
A body of indirect evidence indicates that interventions by occupational therapy practitioners for adult hospitalized patients have the potential to reduce readmissions to the hospital. Large cohort studies based in the United States examined the relationship between occupational therapy interventions and readmissions to the hospital and found that higher use (Burke et al., 2014) and higher intensity (Andrews et al., 2015) of occupational therapy interventions were associated with reduced risk of 30-day readmission among patients with stroke. A study by Rogers et al. (2017) used Medicare claims data from more than 1 million patients with heart failure, pneumonia, and acute myocardial infarction across 19 spending categories. They found that occupational therapy for hospitalized patients was the only category in which additional spending had a statistically significant association with lower readmission rates for all three medical conditions. However, direct evidence is limited to support these claims. The effect of occupational therapy interventions on readmission rates among adults has not previously been synthesized. In this systematic review, we aimed to examine the published literature to determine the effects of occupational therapy interventions for adult hospitalized patients on readmission rates.
Method
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Moher et al., 2009) guidelines were used as a reference to guide reporting in this systematic review. The review protocol was registered prospectively on the International Prospective Register of Systematic Reviews (PROSPERO; CRD42017080779).
The electronic databases MEDLINE, CINAHL, Embase, PsycINFO, and OTseeker were searched from the earliest available date until May 2020. We developed the inclusion criteria for this systematic review using the PICO framework (Shamseer et al., 2015). The search strategy was based on three key concepts: occupational therapy, hospital, and readmission. The population of interest was hospitalized adults. No restrictions were placed on the setting because care delivered to patients in acute, postacute, and mental health settings was eligible. Interventions by either an occupational therapy practitioner alone or as part of an interprofessional team were eligible for inclusion. The initial search was broadened from studies focusing only on occupational therapy interventions given the limited research conducted on occupational therapy practitioners alone.
Interventions were included that (1) were delivered in the hospital environment or (2) were initiated in the hospital as part of an inpatient hospital stay to ease the transition from an inpatient setting to a community setting or to prevent or alleviate problems after hospital discharge (Braet et al., 2016; Eisenberg, 2016). The primary outcome of interest was readmissions to the hospital. The term readmission was used broadly and defined as a second admission to a hospital within a specified period of time after a primary or index admission (Kristensen et al., 2015). No time frame for monitoring readmissions was applied to the search. Synonyms for each concept were combined with the “OR” operator. We then combined the search results of the three concepts using the “AND” operator.
Randomized controlled trials, controlled trials, comparative studies, and observational studies were eligible if they reported readmission data on adult hospitalized patients who received additional occupational therapy interventions compared with the comparison group. No language restrictions were applied. The full search strategy is provided in Supplemental Appendix Figure A.1, available online with this article at https://research.aota.org/ajot.
Two reviewers independently assessed the title and abstract of the articles identified in the initial search using the inclusion criteria (Table 1). In cases of disagreement, consensus was reached via discussion. Full-text copies of studies that met the inclusion criteria or studies that could not be clearly included or excluded from the title and abstract were reviewed independently by the same reviewers using the inclusion criteria. Any disagreements were resolved by a third reviewer. In addition, one author inspected reference lists of included articles to identify any others that might be eligible. We conducted citation tracking using Google Scholar for all articles meeting the inclusion criteria to identify additional articles not identified in the initial search.
Inclusion and Exclusion Criteria
A customized data extraction tool was developed and tested. Data were extracted by one reviewer and checked by a second reviewer. Two reviewers assessed methodological quality using the Downs and Black checklist (Downs & Black, 1998) for measuring the quality of randomized and nonrandomized studies. This tool comprises 27 questions divided into 5 subsections, including reporting (10 items), external validity (3 items), internal validity bias (7 items), internal validity confounding (6 items), and power (1 item). The question relating to power was scored out of 5 applying the guidelines described by Speed and Harding (2013) so that a score of 5 represented a clearly powered study, a score of 3 indicated a marginally powered study, and a score of 0 meant that the study was not sufficiently powered. On the basis of Downs and Black checklist scores, the quality of the included studies was classified as excellent (>25), good (20–25), fair (15–19), or poor (≤14; Samoocha et al., 2010). Articles were not included or excluded on the basis of methodological quality; instead, these results were considered during the interpretation of results.
A meta-analysis was conducted with clinically homogeneous data. Results of 1-mo (including 28 and 30 days) readmission rates of adult hospitalized patients who received general medical and surgical care as well as occupational therapy interventions compared with standard care were analyzed by meta-analysis. In the case of moderate–high levels of statistical heterogeneity (I 2 ≥ 50%), subgroup analysis was used to evaluate whether interventions in specific domains were more effective. We performed meta-analyses using Review Manager (Version 5.3; Cochrane Collaboration, London, England). We calculated a 95% confidence interval (CI) between groups using a random effects model; this model was selected because of the different protocols and participant groups in included studies. The results were expressed as risk ratios (RRs). The I 2 statistic was used to interpret heterogeneity between studies.
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was applied to the meta-analysis to determine the quality of the evidence across the included studies (Table 2; Schünemann et al., 2013). The GRADE approach results in an assessment of the quality of a body of evidence in one of four grades: high, moderate, low, and very low. Evidence was downgraded on the basis of predetermined criteria by one level from “high” if (1) the majority of the studies in the meta-analysis had Downs and Black checklist scores <20; (2) greater than low levels of statistical heterogeneity were found between studies (I 2 > 25%); and (3) CIs for estimates of RRs were wide, indicating a lack of precision. If combining data was not appropriate, results were described narratively.
GRADE of Evidence for Additional Hospital-Based Occupational Therapy Interventions and Hospital-Based Occupational Therapy Interventions Provided Across Hospital and Community Settings Versus Standard Care for 1-Month Hospital Readmissions
Note. CI = confidence interval; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; RR = risk ratio.
Reason for downgrade: statistical heterogeneity (I 2 > 25%) and wide CI.
Reason for downgrade: wide CI.
Results
Study Characteristics
The electronic database searches yielded 2,839 results. Eight additional studies were identified and reviewed against the inclusion criteria. After duplicates were removed, 2,314 studies remained and were screened by title and abstract. Full-text copies of 39 articles were assessed for eligibility against the inclusion criteria, and a further 27 studies were omitted, leaving a final yield of 12 articles (Figure 1). One article by Haines et al. (2017) reported data from two separate trials. Only data from Trial 1 were included in this systematic review because the amount of service provided by occupational therapy staff was clearly described. In this study, Trial 2 presented data on a transprofessional model of practice, but it was not clear whether an occupational therapy practitioner was part of the treating team; as a result, Trial 2 was excluded.
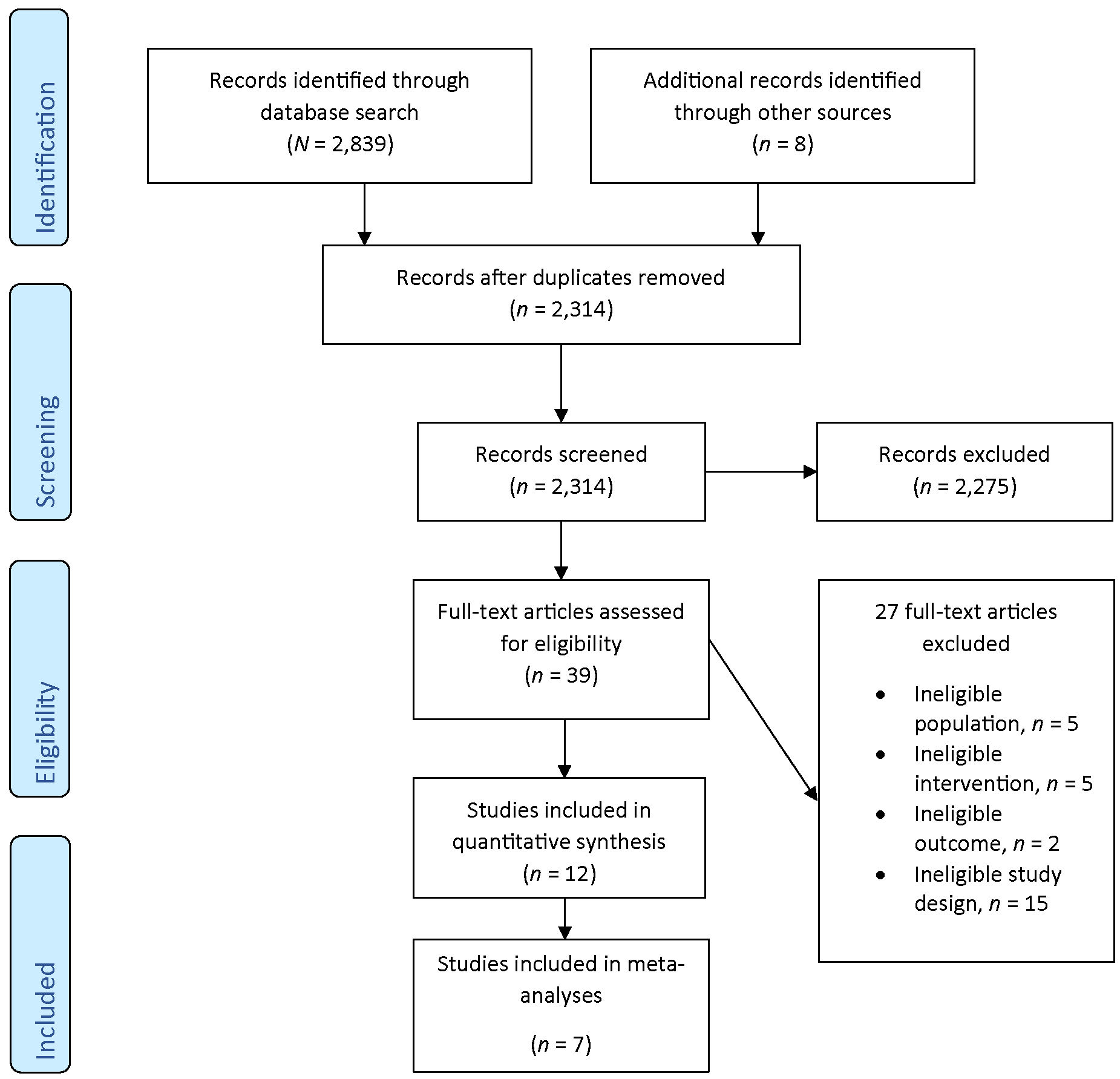
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
The mean score on the Downs and Black checklist was 25.2 of the maximum 32 points, and the range was 20 to 29 across all included studies. Four studies were of excellent quality (Brusco et al., 2014; Haines et al., 2017; Lockwood et al., 2019; Mudge et al., 2006), and the remaining studies were of good quality. The majority of studies had an absence of blinding of participants because of the nature of the study; they also scored low in relation to power because of relatively small sample sizes (see Supplemental Appendix Table A.1).
Supplemental Appendix Table A.2 summarizes the characteristics of the included studies. Of the 12 studies, 7 were randomized controlled trials (Brusco et al., 2014; Drummond et al., 2013; Eyres & Unsworth, 2005; Haines et al., 2017; Lannin et al., 2007; Lockwood et al., 2019; Pardessus et al., 2002), 2 were prospective controlled trials (Mudge et al., 2006; Nielsen et al., 2018), 2 were observational studies (Ip et al., 2004; Shimada et al., 2019), and 1 was a matched case–control study (Simpson et al., 2019).
The included studies involved a total of 18,533 patients. However, the sample sizes ranged from 10 participants (Lannin et al., 2007) to 14,834 participants (Haines et al., 2017). The mean age of the participants ranged from 42.1 yr (Shimada et al., 2019) to 83.2 yr (Pardessus et al., 2002). All the studies were carried out within the hospital environment, with 4 studies completed in general postacute care settings (Brusco et al., 2014; Lannin et al., 2007; Lockwood et al., 2019; Pardessus et al., 2002), 3 studies completed in an acute general medical or surgical setting (Eyres & Unsworth, 2005; Haines et al., 2017; Mudge et al., 2006), 1 study completed in a stroke rehabilitation unit (Drummond et al., 2013), 2 studies completed across both acute and postacute settings (Ip et al., 2004; Simpson et al., 2019), 1 study completed in an acute short stay unit (Nielsen et al., 2018), and 1 study completed in a mental health facility (Shimada et al., 2019). Six studies were completed in Australia (Brusco et al., 2014; Eyres & Unsworth, 2005; Haines et al., 2017; Lannin et al., 2007; Lockwood et al., 2019; Mudge et al., 2006), 1 in the United States (Simpson et al., 2019), 1 in Hong Kong (Ip et al., 2004), 1 in France (Pardessus et al., 2002), 1 in Denmark (Nielsen et al., 2018), 1 in England (Drummond et al., 2013), and 1 in Japan (Shimada et al., 2019).
Interventions
Variation was found in the study protocols. Four studies explored the impact of the addition of a predischarge home assessment visit by an occupational therapy practitioner (Drummond et al., 2013; Lannin et al., 2007; Lockwood et al., 2019; Pardessus et al., 2002). Two studies explored the effect of weekend therapy services (Brusco et al., 2014; Haines et al., 2017). Two studies investigated the addition of a comprehensive assessment and discharge planning model (Mudge et al., 2006; Nielsen et al., 2018). Three studies investigated the effect of increasing access to occupational therapy interventions (Eyres & Unsworth, 2005; Ip et al., 2004; Shimada et al., 2019), whereas 1 study compared different funding models incorporating different levels of therapy interventions (Simpson et al., 2019). All studies compared receiving standard care occupational therapy interventions to receiving additional occupational therapy interventions. None of the studies included a comparison in which occupational therapy care was not received.
Rate of readmission to the hospital was used as a primary or secondary outcome in all the included studies. However, the time point specified for monitoring readmissions to the hospital varied. Thirty-day readmission rate was the most commonly reported outcome measure (Brusco et al., 2014; Drummond et al., 2013; Lannin et al., 2007; Lockwood et al., 2019; Nielsen et al., 2018). However, other studies reported a variety of different time points, including 28 days (Haines et al., 2017; Ip et al., 2004), 12 wk (Eyres & Unsworth, 2005), 100 days (Ip et al., 2004), 6 mo (Mudge et al., 2006; Nielsen et al., 2018), 12 mo (Pardessus et al., 2002), and 2 yr (Shimada et al., 2019).
Readmission Rates
The meta-analysis of 7 studies with 16,718 participants provided low-quality evidence that 1-mo readmission rates were reduced among adult patients hospitalized for general medical and surgical care receiving occupational therapy interventions compared with standard care (RR = 0.77, 95% CI [0.60, 0.97], I 2 = 54%; Figure 2). The study by Haines et al. (2017) was attributed 34.7% weight within the meta-analysis because of its large number of participants.
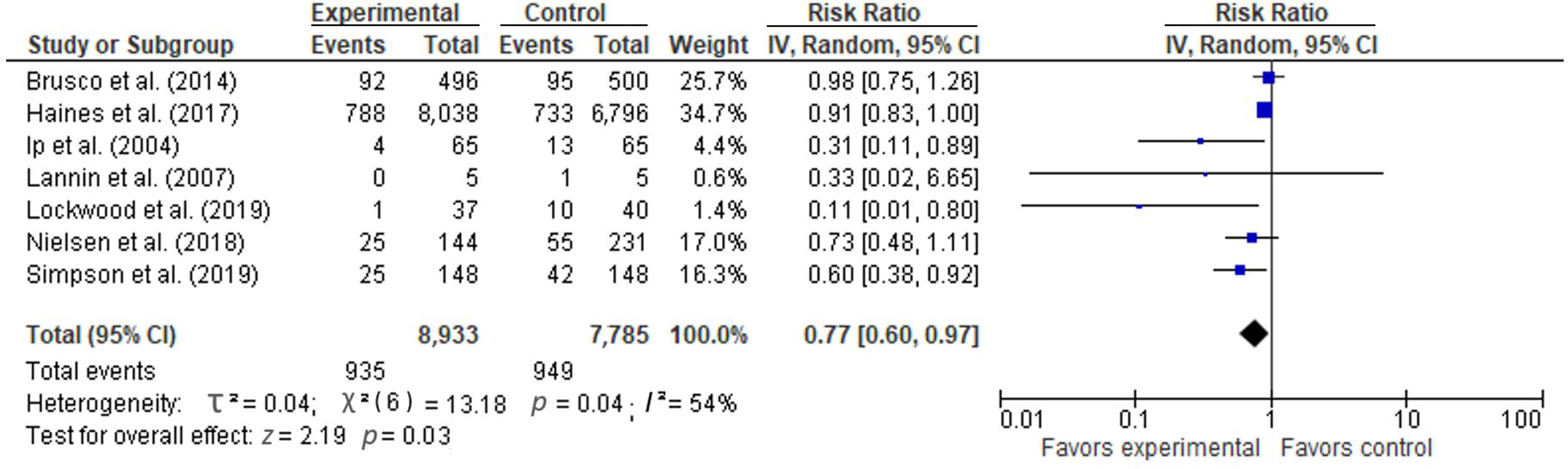
Forest plot of comparison: Hospital-based occupational therapy interventions versus standard care, outcome: 1-mo readmission rates.
Because of moderate levels of heterogeneity (I 2 = 54%), a subgroup analysis was performed to investigate the effect of occupational therapy interventions initiated during the inpatient hospital stay and focused on the transition back to community settings. Subgroup analysis of 4 studies with 758 participants provided moderate-quality evidence that occupational therapy transitional care interventions reduced 1-mo readmissions to the hospital among adult general medical and surgical patients compared with standard care (RR = 0.61, 95% CI [0.42, 0.89], I 2 = 18%; Figure 3).
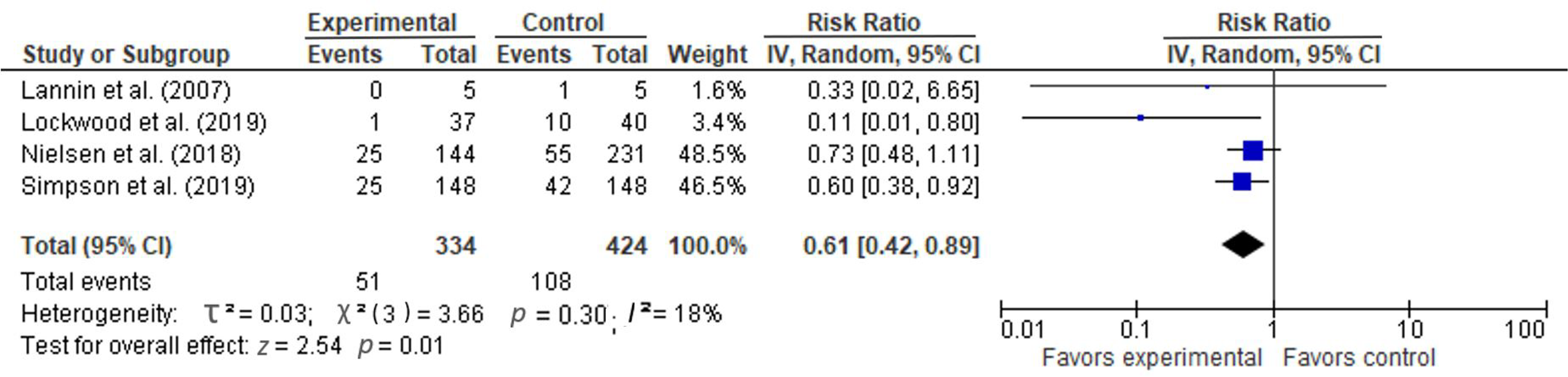
Forest plot of comparison: Hospital-based occupational therapy interventions provided across hospital and community settings versus standard care, outcome: 1-mo readmission rates.
Data from five studies were not included in the meta-analysis because of differences in patient populations or time points for monitoring readmissions to the hospital. Two studies found no difference in long-term readmissions to the hospital between the intervention and comparison groups within 6 mo (Mudge et al., 2006) and 12 mo (Pardessus et al., 2002). Drummond et al. (2013) reported more readmissions among patients with stroke who participated in a predischarge home visit compared with those who received standard care. Of the 15 participants included in the pilot study of Eyres and Unsworth (2005), 1 control group participant was readmitted twice within 12 wk after discharge. Shimada et al. (2019) reported significantly longer time to readmission among patients with schizophrenia who received individualized treatment compared with those who received usual group intervention.
Causes of Readmission to the Hospital
Only 2 studies reported on causes for readmission to the hospital. Pardessus et al. (2002) reported the number of participants readmitted for falls compared with other reasons within 12 mo of discharge, whereas Lockwood et al. (2019) reported on all reasons for readmission within 30 days (intervention group, n = 1 medical reason; control group, n = 5 falls, n = 3 functional decline, n = 3 medical reason).
Discussion
In this systematic review, meta-analysis provided evidence that occupational therapy interventions for hospitalized adults admitted for surgery or for the management of acute medical conditions were effective in reducing 1-mo readmissions to hospital. However, because of the high degree of heterogeneity, the quality of evidence is low, indicating that future research may affect the estimates of effect. Subgroup analysis provided moderate-quality evidence with acceptable levels of heterogeneity that occupational therapy transitional care interventions were effective in reducing 1-mo readmissions among adult hospitalized patients receiving general medical and surgical care.
These findings are important to inform current and future decisions regarding resource allocation in health care. An important finding of this systematic review was that adult hospitalized patients receiving medical and surgical care who participated in additional occupational therapy interventions had less risk of being readmitted to the hospital in the first month after discharge compared with those receiving standard care. Although no prior reviews about the effect of occupational therapy interventions for hospitalized adults on rates of readmission have been identified, another systematic review (Lockwood et al., 2015) explored the role of predischarge home assessment visits completed by occupational therapy practitioners and found evidence that they reduced the risk of readmission to the hospital. In this review, the features that were similar across the interventions were (1) comprehensive assessment of the patient; (2) a focus on patients’ contextual factors, including their functional and social needs; and (3) provision of individually tailored strategies and programs that support patient self-management and empowerment. Stronger evidence was also found to support interventions that focused on the transition from the hospital to the community.
Similar findings have been identified in reviews of discharge interventions (Braet et al., 2016; Gonçalves-Bradley et al., 2016; Scott, 2010) and interventions to reduce hospital readmissions (Leppin et al., 2014). In these reviews, considering the hospital–community interface and focusing on patient empowerment (which enabled patients to make informed choices) were both seen as key elements of interventions that were effective in reducing hospital admissions.
When interpreting the results of studies in this systematic review, it is important to consider that all studies compared standard care occupational therapy interventions with receiving additional services. All studies used standard occupational therapy service provision (along with other multidisciplinary care) as the comparator. Therefore, the results in this review may present a conservative estimate of the effect of occupational therapy interventions for hospitalized adults on readmission rates. One study (Rogers et al., 2017) of more than 1 million patients in acute care settings in the United States reported that the vast majority of patients with pneumonia, heart failure, and acute myocardial infarction were not seen by an occupational therapy practitioner (72%–79%), suggesting that opportunities exist to complete research in which standard care includes no care delivered by occupational therapy practitioners.
In this systematic review, another factor influencing the data was heterogeneity. Heterogeneity in the included studies was present in the patient populations, interventions provided, and the study context, including health care and funding models provided across multiple countries. The context in which an intervention is delivered may play a role, not only in the way that the intervention is delivered but in the way that services are configured for the control group. Six of the 12 studies included in this review were based in Australia, with the remaining 6 studies being performed in the United States, Hong Kong, France, Denmark, England, and Japan. In each country, funding arrangements and the orientation of primary care services differed, which has implications for the interpretation of the results.
The patient populations also varied; however, the majority of participants were admitted for management of acute medical conditions or for surgery, and the studies were conducted predominantly in postacute settings. In addition, because some interventions were occupational therapy alone, whereas others were multidisciplinary interventions, the interpretation of study variability is further complicated. Moreover, not all interventions were described clearly, and available information was often limited on how the occupational therapy intervention was delivered. Variation in the quality of a delivered intervention can have an impact on outcomes in systematic reviews and can be a major source of clinical heterogeneity (Herbert & Bø, 2005).
A further important dimension of the fidelity of the intervention relates to dose, which includes the focus of the intervention sessions, the number and frequency of the sessions, and the length of the contact (Bellg et al., 2004). The dose of the intervention varied considerably across studies and could not be determined with any accuracy in the majority of studies. Further high-quality trials are needed to explore the effects of providing occupational therapy interventions in hospital settings and to define the patients most likely to benefit as well as the content and intensity of the interventions that make a difference.
Limitations
A limitation of this systematic review is the small number of studies investigating the effect of occupational therapy interventions for hospitalized adults on readmission rates. One reason for this limited literature may be that the broader concept of rehabilitation may have been described as the intervention rather than interventions delivered explicitly by occupational therapy practitioners. Readmission to the hospital was not typically a primary outcome in these studies, and so they may have been underpowered to detect an intervention effect in a secondary outcome. From the studies included in this review, no consistent definition or time frame for readmission was found; moreover, given the lack of information reported in studies about the reasons for readmission, it was often not possible to determine whether the readmissions were planned or unplanned. Heterogeneity was present in the study context, the interventions, and the amount of occupational therapy provided. Consideration was given to the clinical homogeneity in the meta-analyses, and the more conservative random effects model was used for analysis. The GRADE approach was also applied, which determines the level of confidence in the results.
Implications for Occupational Therapy Research and Practice
Unplanned hospital readmissions impose a burden on health care facilities and affect the health and well-being of patients. Occupational therapy practitioners working in hospital settings need to understand their value and their contribution to addressing readmissions. The results of this systematic review have the following implications for occupational therapy research and practice: Occupational therapy interventions can be effective in reducing readmissions in some adult hospitalized patient populations, including those admitted for surgery or management of acute medical conditions. Stronger evidence was found to support interventions that focus on transition from the hospital back into the community. Features that were similar across interventions that were effective in reducing readmissions included comprehensive assessment of the patient; a focus on contextual factors, including functional and social needs; and provision of individually tailored strategies and programs that support patient self-management and empowerment. A need exists for further well-designed studies to evaluate the relationship between readmissions and occupational therapy interventions with different patient populations and in different hospital settings. Occupational therapy practitioners and researchers need to consider how the unique value of their contribution is measured when they are working both alone and collaboratively as part of the broader rehabilitation team.
Conclusion
Occupational therapy interventions delivered by occupational therapy practitioners alone or as part of a team can be effective in reducing readmissions in some adult hospitalized patient populations, including those admitted for surgery or management of acute medical conditions. Stronger evidence was found to support interventions that focused on the transition from inpatient hospital care back into the community. Further rigorous research in studies with strong intervention fidelity is required across other patient populations and hospital settings to determine the patients most likely to benefit as well as the content and intensity of the interventions that make a difference.
Supplemental Material
Supplementary material for Effectiveness of Hospital-Based Interventions by Occupational Therapy Practitioners on Reducing Readmissions: A Systematic Review With Meta-Analyses
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.048959.pdf for Effectiveness of Hospital-Based Interventions by Occupational Therapy Practitioners on Reducing Readmissions: A Systematic Review With Meta-Analyses by Kylee J. Lockwood and Judi Porter in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
The authors declare no potential conflicts of interest with respect to the research, authorship, and publication of this systematic review. Both authors made substantial contributions to the conceptualization and design of the study, analysis, and interpretation of data; drafted and revised the article critically for important intellectual content; and gave final approval of the version submitted. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The authors acknowledge Victoria Richardson, who contributed to study conceptualization and the first round of study selection.
*
Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.