
Abstract
A qualitative exploration of occupational therapists’ experiences in primary care found that participants perceived contributing to positive outcomes through working with patients on self-management, functional problem solving, and behavior change.
The Patient Protection and Affordable Care Act (ACA; Pub. L. 111-148), passed in 2010, catalyzed efforts to provide comprehensive primary health care as a means to improve health in the U.S. population (Jacobson & Jazowski, 2011). One key component of comprehensive primary health care involves transitioning from a dyadic physician–patient relationship to an interprofessional team approach, which can include occupational therapy practitioners (Halle et al., 2018). Indeed, primary care providers have articulated the value occupational therapy practitioners bring to the team through improved patient outcomes and organizational change (Dahl-Popolizio et al., 2017; Eichler & Royeen, 2016; Merryman & Synovec, 2020). Moreover, researchers have identified a broad range of unmet patient needs that can be addressed in primary care and fall within occupational therapy’s scope of practice (Winship et al., 2019).
Although strong evidence supports the opportunities for occupational therapy in the domain of primary care, no study has yet examined the experiences of occupational therapists from different contexts and U.S. regions to understand contemporary practice. Investigating these experiences can help clarify the processes for becoming part of the care team as well as facilitators of and barriers to service provision. Thus, the aim of this qualitative study was to explore contemporary occupational therapy in primary care by answering the following research question: What are occupational therapists’ experiences of and recommendations for the role of occupational therapy in primary care? The results can guide future efforts toward integrating occupational therapy into primary care.
Method
Study Design
We used a descriptive qualitative study design with deductive thematic analysis to explore experiences (e.g., barriers to and facilitators of providing care) and recommendations for the role of occupational therapy practice in primary care, which was approved by the University of Pittsburgh’s institutional review board. All participants provided verbal consent to take part in the study procedures. Descriptive qualitative designs aim to identify key patterns while staying close to the data (Moser & Korstjens, 2018). Questions for semistructured interviews were guided by Donabedian’s (1966) health services framework.
Researcher Description
The principal investigator (PI; Stephanie A. Rouch) is a trained occupational therapist with experience providing occupational therapy services in a primary care community-based setting. Past experience contributed to her belief in the benefit occupational therapy can offer the primary care team, which led to the pursuit of this research. During the time of data collection and analysis, the PI was not providing occupational therapy services in a primary care setting.
Participants
Participants were included if they were licensed occupational therapists in any state in the United States. They had to have at least 6 mo of experience in the past 5 yr in a primary care setting in the United States in order to capture practice experiences specific to the national health care context. Participants were initially recruited in June 2019 by means of purposive sampling so we could capture rich experiences (Moser & Korstjens, 2018). We transitioned to snowball sampling from August 2019 to December 2019 to capitalize on the existing network of occupational therapists in primary care. All participant interviews took place from July 2019 to December 2019. Three people expressed interest but were not eligible because they had less than 6 mo experience providing services in a primary care setting.
Data Collection Procedures
Participants completed a brief demographic survey via Qualtrics describing their practice experience overall and in primary care (available on request). They then engaged in 1:1 semistructured standardized telephone interviews (available on request) with the PI, which were then transcribed. To further immerse herself in the data, the PI listened to and read through all transcripts at least twice before the analysis.
Data Analysis
After each interview, the PI engaged in first-round coding using the Donabedian framework, which focuses on the structure, process, and outcome of health care. Examples of possible codes for barriers or facilitators reflecting this framework included space or equipment (i.e., structure), team communication (i.e., process), and patient satisfaction (i.e., outcome). Possible recommendation codes that reflect next steps in primary care included policy and educational opportunities. With each subsequent interview, codes were added as new ideas emerged. Once data saturation occurred (i.e., no new codes were created for the final two interviews), a codebook was created from all first-round codes. This codebook reflected descriptive codes for barriers and facilitators from the Donabedian framework as well as recommendations for future integration of occupational therapy into primary care. All transcripts were then recoded with the codebook using NVivo software (Version 12; QSR International). Each code was then analyzed to develop themes and subthemes, which were presented to the participants in July 2020 by means of a member-checking presentation and Word document.
Participants were given 4 wk to review the data and provide feedback through a 10-question, open-ended survey. This member-checking process added trustworthiness to study findings by providing participants the opportunity to add context and ensure the accuracy of initial themes (Korstjens & Moser, 2018). Five of 7 participants provided feedback by August 2020; this feedback was then integrated into the subthemes for additional context.
Results
Participants consisted of 7 occupational therapists (all women) with 1 to 8 yr of experience providing occupational therapy services in primary care (Table 1). Four themes emerged regarding the experiences of and recommendations for occupational therapy’s role in primary care: (1) gaining entry onto the primary care team, (2) navigating team-based care, (3) providing patient-centered care, and (4) expanding reach nationally (Figure 1).
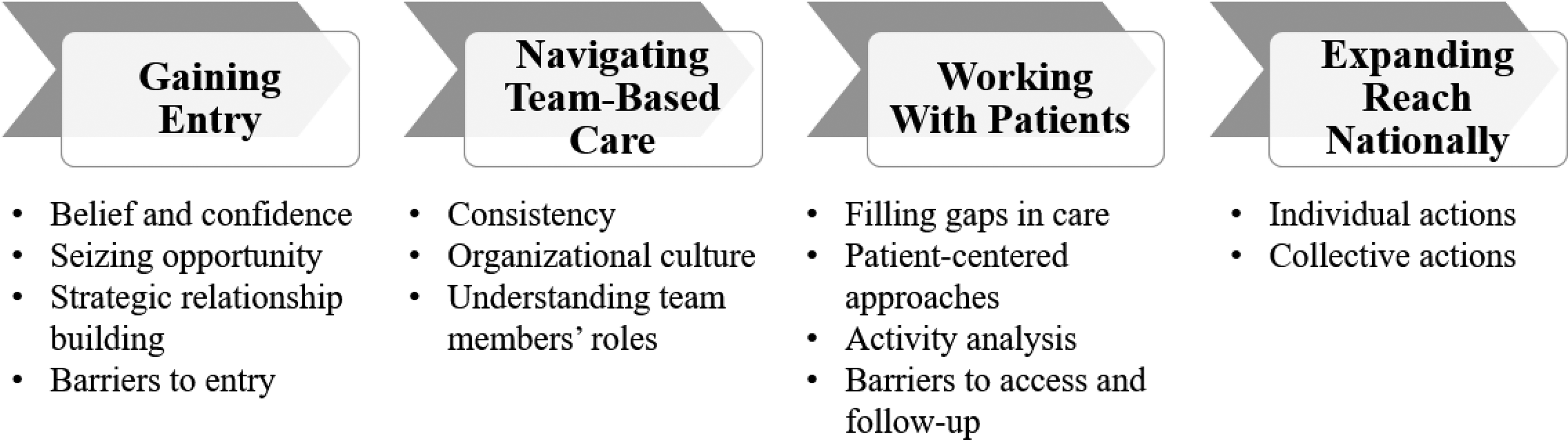
Themes and subthemes.
Participants’ Experience Providing Occupational Therapy Services
Note. N = 7. OT = occupational therapy.
OT experience in traditional settings categories are not mutually exclusive. Many participants reported past experience in more than one setting. bBased on data from the U.S. Census Bureau (2010).
Theme 1: Gaining Entry Onto the Primary Care Team
Seeking and gaining entry was fueled by participants’ belief in the value of occupational therapy services in primary care in combination with their confidence in providing skills-based care. Participants reported that “OT naturally fits in a primary care environment” (Participant 2) given that occupational therapy practitioners are “naturally good at behavioral health and addressing the person holistically” (Participant 1). For patients “dealing with depression, pain, fall risk, age, and safety . . . I feel that I’m uniquely qualified to help them” (Participant 6).
Belief and confidence cemented into action, resulting in the participants having seized opportunities in various ways. Four participants were sought out to fulfill an existing occupational therapy position in primary care. Three participants intentionally created their positions in primary care: “I literally just made an appointment [with my primary care doctor] and said, ‘I think you should hire me and this is what I think I can do,’ and he was like really interested . . . ‘Let’s try this out’” (Participant 2). Participants also leveraged their networks by gaining financial and organizational support from institutions, granting them access to opportunities that may not otherwise be possible. “One of the professors said to me, ‘Hey, what if we went for a . . . grant for patients in primary care?’” (Participant 6).
All participants mentioned that strategic relationship building with stakeholders was a key facilitator to gaining entry: “You have to address all areas of getting into clinic culture—front desk staff, MAs [medical assistants], clinic staff, physicians. . . . If any one of those pieces is out of alignment, there is a risk of disintegrating” (Participant 3). Participants emphasized that relationship building is not a one-step milestone: “It did take a lot of groundwork and selling OT to the general physicians who were providing the services. . . . So just making sure to maintain that constant presence is huge” (Participant 1).
Even with relationship building, consistent communication, and advocacy for occupational therapy’s role, participants faced barriers to actualizing their potential in primary care settings, including lack of space, resources, control, and understanding of their role: “I feel no control over this situation, and I’m working in a conference room with . . . no room for supplies, working with my mind and my piece of paper, no computer” (Participant 6). Finally, some participants found themselves in a position of needing to figure out what their role would be: I can’t say that I had much of an idea of what type of work would be involved. . . . In acute care, and also rehab, you’re always expected to be able to fill the role of OT, wherever it is . . . it wasn’t until I really got into the clinic that I realized that this was going to take more work than sort of just going to a different floor and kind of winging it. (Participant 4)
Theme 2: Navigating Team-Based Care
Participants all agreed on the value of team-based care and saw occupational therapy as a complement to the team. They reflected on the importance of consistency for building relationships and understanding roles. One participant acknowledged how regular time in the office contributed to more referrals: “If I wasn’t in the office . . . I probably wouldn’t get as many [referrals]. . . . Being the regular face is helpful” (Participant 1). Provider consistency also was important. When the participant could build a relationship with the same providers over time, those providers would become advocates for occupational therapy services. For some participants, however, the providers with whom they worked varied from week to week. Inconsistency made forming a relationship difficult: “There are multiple providers, they are late for their own appointment, so it is hard to fit in a time to kind of pop in and introduce yourself” (Participant 5).
Understanding team members’ roles enhanced patient care by ensuring that patients accessed the providers they needed: “I think that we can also help bridge gaps . . . we can make sure [patients] talk with the social worker” (Participant 1). On the other hand, other providers’ lack of understanding of occupational therapy’s role contributed to inappropriate referrals: “People don’t know who to refer to OT…. Sometimes they’d rather have me see all their patients than try to figure out who to send” (Participant 6). Another participant reported that a lack of understanding resulted in too few referrals: “We were [only] receiving referrals for a couple of musculoskeletal problems. You know, a lot more of the traditional occupational therapy services . . . changing people’s minds about what occupational therapy can do was a challenge” (Participant 4).
The organizational culture either acted as a facilitator of or barrier to team-based care. When the culture was more collaborative and patient centered, participants expressed having had greater success with providing care as part of a team: “There have been some providers [who] have been really good about collaboration . . . the providers will ask patients to schedule when I’m in the office so I can see them” (Participant 2). In contrast, the organizational culture did not always align with occupational therapy approaches: “The other thing about this setting, it operates more from the medical model, so it’s more about trying to control hypertension; it’s about just medicating them” (Participant 7).
Theme 3: Providing Patient-Centered Care
Within this theme, participants emphasized the importance of understanding the individual patient and their care needs. Thus, the subthemes captured patient populations cared for, approaches used to guide interactions, the importance of in-depth interviewing and activity analysis, and barriers to providing care. Participants reported how a growing population of patients with unmet chronic care needs provided an opportunity for occupational therapy services to fill gaps in care: “We get like a mix of just those patients who just are falling through the cracks” (Participant 2). They also described treating patients with chronic pain, arthritis, concussions, repetitive use injuries, multiple chronic conditions, anxiety and depression, and patients with a high fall risk. Older adults with mild cognitive impairment and preclinical disability in particular benefited from occupational therapy, because “they don’t qualify for home health or a visiting nurse, because they’re too independent. But they’re starting to have initial signs of decreased independence” (Participant 1). Patients who benefited most were functioning independently enough to be ineligible for traditional services but needed occupational therapy “to control their pain, fatigue, reduce the risk of falling, [and] increase the safety” (Participant 6).
To promote participation and health promotion, all participants reported engaging in patient-centered approaches to maximize patient engagement. Three participants reported being primarily driven by a self-management approach, with an emphasis on managing chronic conditions and engaging patients through self-selected goals. Two participants focused on sustainable behavior change to promote healthy habits and routines into patients’ day-to-day functioning. Two participants most strongly emphasized focusing on function: “I am all about functional problem solving with patients through their day to day, and that’s my approach . . . doing some education and then setting an action plan or coming up with different strategies that are personalized” (Participant 2).
All participants reported using activity analysis and in-depth interviewing to comprehensively understand the root causes of a patient’s symptoms. For example, one participant determined that a patient’s nonergonomic behaviors were caused by lingering fear as a result of a decades-old automobile accident: “A patient had a lot of sciatic pain. . . . We found out that she was sitting too far away from her steering wheel” (Participant 4). Another participant reported a similar process when working with a patient with chronic back pain and migraines, which prevented him from working and surfing on consecutive days, despite a year of physical therapy: “I started asking him, ‘How do you surf?’ And we went through this whole activity analysis [and] energy conversation strategy. . . . [The patient] said, ‘Any time I do what we talked about, I can surf the next day’” (Participant 2).
Although all participants had success stories regarding patient care, they also identified operational barriers that contributed to lack of patient access to occupational therapy services. For example, one participant reported how patients “cannot receive Medicare A (home care services) and Medicare B (outpatient OT) at the same time” (Participant 6), which makes registering and scheduling patients difficult. One participant highlighted challenges with Medicare and local insurers denying reimbursement. Chronic condition management and coaching interventions resulted in “denials stating that you’re billing for [self-care] and it’s not an [activity of daily living], you’re not doing dressing, bathing, [or] grooming” (Participant 2). Some patients had insurance but could not afford the accompanying copays: “We have . . . underserved folks who have really good insurance but can’t really pay the copay” (Participant 7). Finally, lack of transportation and scheduling challenges made it difficult for patients to attend follow-up appointments: “[The patients] had good intentions of coming back, but it was difficult for them to come back” (Participant 5). High copays, limited reimbursement, scheduling difficulties, and transportation all negatively affected patient care access and follow-up.
Theme 4: Expanding Reach Nationally
On the basis of their experience gaining entry to the primary care milieu and providing team-based, patient-centered care, participants ultimately saw benefit in expanding their reach nationally. They described actions occupational therapy practitioners could take to create a position for themselves as well as collective actions needed to help secure occupational therapy’s position in primary care.
Multiple participants mentioned that occupational therapy practitioners can use existing evidence to support the field’s role in the self-management of chronic conditions and health behavior change: “I see a lot of what we do in primary care as things that OTs have done for generations. Chronic condition management isn’t new; we have been doing that since the 1960s” (Participant 3). Participants also recommended taking advantage of continuing education opportunities to gain skills in promoting self-management, health behavior change, and pain management: “I think that training on behavior change, making sure people are aware of how to assess readiness for change and how to approach those different stages of change [are important]” (Participant 5). Finally, seeking mentorship within the profession and networking outside the profession with primary care providers were mentioned by participants as key recommendations for practitioners hoping to gain entry onto the team. One participant mentioned that a place to start would be networking with state primary care physician organizations: “I do think OTs have a huge value linking up with a physician organization . . . every state has those” (Participant 2). For those already practicing in primary care, participants expressed that individual practitioners should communicate the profession’s role: “OTs [who] are in primary care . . . need to continue to tell others how they did what they did, with education through OT Practice magazine, conferences, and partnering interprofessionally in research with their peers” (Participant 3).
Participants recommended the following collective actions for occupational therapy as a profession: embedding primary care practice into entry-level education (including fieldwork placements), generating health services research evidence, capitalizing on policy efforts, and achieving a consensus on occupational therapy’s role in primary care. To promote confidence among the next generation of practitioners, they supported the idea of fieldwork opportunities in primary care: “It definitely starts with students. I think we need to start not only educating our students in the classroom, I think we need to embed students in primary care clinics where there are OTs” (Participant 3). Generating health services research that evaluates occupational therapy practitioner contributions to system-level outcomes (e.g., health care utilization, patient self-rated health) is a necessary next step toward influencing policy. Participants highlighted the need to capitalize on policy efforts aligned with prevention, wellness, and health promotion: “The ACA . . . has OT written all over it” (Participant 3). Participants, aware of broad policy support for prevention-oriented activities, noted the need to advocate for billing codes that are reflective of health management activities: Self-care is not just brushing your teeth, or combing your hair, or going to the bathroom—self-care is being able to manage your disease . . . so having a broader self-care and home management [billing code] would be helpful to really encompass a broader scope. (Participant 2)
Above all, participants reported the need for a clear consensus on occupational therapy’s role in primary care to reach the wider audience of occupational therapists, primary care team members, and policymakers. A collective consensus on occupational therapy’s role is a first step to clearly communicating the role through action: “So, if [our role] is in medication management, home evaluations, [or] fall prevention . . . it emerges more strongly in what we do—rather than people still being confused about our area of expertise” (Participant 7).
Discussion
This study captured 7 occupational therapists’ experiences of and recommendations for the presence of occupational therapy in primary care. We learned that participants’ commitment to pursuing an emerging practice area was critical to their success. To become part of the team, participants fostered interprofessional relationships, garnered organizational resources, and built their knowledge base and skills. Once on the team, continued and consistent integration is needed to deliver occupational therapy services. To achieve the goal of integrating occupational therapy into this practice setting, both grassroots efforts from primary care clinicians and top-down efforts from health systems, state associations, and AOTA are needed.
Comprehensive primary care delivered by an interprofessional team has the potential to achieve the population health goals set forth by the ACA (Jacobson & Jazowski, 2011). Although team-based care shows promise in contributing to positive patient outcomes, integrating new team members and expanding the roles of existing team members is challenging (Karimi-Shahanjarini et al., 2019; Pape & Muir, 2019). Consistent with past studies, we found that the barriers to primary care entry included poor understanding of occupational therapy’s role and limited reimbursement (Halle et al., 2018), and facilitators included networking, consistency, and constant communication of occupational therapy’s scope of practice (Eichler & Royeen, 2016; Koverman et al., 2017). Our study adds to this evidence by integrating the multiple individual, interpersonal, and institutional factors that contribute to the successful integration of occupational therapy practitioners into a primary care team.
Professional grassroots approaches to health care improvement can help ensure sustainable change because change agents’ efforts are fueled by belief, meaning, and purpose in their work (Harnett, 2018). Indeed, all of our participants demonstrated their grassroots initiative to address an unmet need in their community by championing an emerging practice area. They adopted behaviors of influential change agents, including developing the skills and knowledge needed to meet population health needs, communicating their role to the team, and modeling their role through delivery of best practice (McCormack et al., 2013). Continued grassroots efforts will be critical to achieving widespread integration of occupational therapy into primary care (Koverman et al., 2017; Pape & Muir, 2019).
Change agents cannot achieve success alone (McCormack et al., 2013). When clinicians adapt care delivery to meet patient needs without accompanying organizational support, there is a risk of both staff burnout and poor outcomes (Tucker & Edmondson, 2003). To support grassroots efforts, organizations (e.g., health systems) can provide the structure (e.g., clear professional roles and expectations) and resources needed for sustainable change (Harnett, 2018). Within a professional organization, a formal pipeline for clinical mentorship is one strategy to support practitioners who seek to enter primary care (Ramsey, 2011).
Combining top-down and grassroots approaches to health care implementation can provide both the resources and motivation needed for change (Harnett, 2018; Stewart et al., 2015). Achieving a consensus on the key contributions of occupational therapy to primary care is one key action that would benefit from top-down and grassroots input. The next step, building on existing efforts by the American Occupational Therapy Association (AOTA; 2020) to disseminate occupational therapy’s role in primary care, would be to involve multiple stakeholders to prioritize occupational therapy’s key contributions and identity on primary care teams. This approach has been achieved in other disciplines by executing a Delphi process that establishes an evidence-based consensus among key primary care stakeholders (e.g., clinical experts, researchers; Sumsion, 1998). Collectively identifying occupational therapy’s key contributions to and identity on primary care teams would facilitate a greater ability to communicate and demonstrate unique areas of expertise that contribute to the health needs of the U.S. population.
Limitations
This study has several limitations. The PI conducted all the interviews, coding, and theme development. Although steps were taken to decrease bias (e.g., member checking), having a single person code all interviews and develop the themes increased the risk of bias. Second, as with any research, it is possible that occupational therapy practitioners who had unfavorable experiences practicing in a primary care setting opted not to participate in this study, resulting in their experiences not being reflected in the data. Third, although we reached data saturation in our interviews, our sample size was small, which increases the likelihood that we did not capture all perspectives.
Implications for Occupational Therapy Practice
Our findings provide a road map and considerations for occupational therapy in this emerging practice area. As members of an interprofessional primary care team, occupational therapy practitioners can fill critical gaps in service by using their unique skill set to promote improved patient outcomes. Recommendations for occupational therapy practitioners aiming to practice in primary care include consuming existing evidence that supports occupational therapy’s role, including evidence on chronic condition management (AOTA, 2021); pursuing relevant continuing education, including health behavior change, behavioral health, and functional cognition; seeking mentorship within the profession; and networking with primary care providers outside the profession.
Conclusion
This qualitative study explored occupational therapy practitioners’ experiences of and recommendations for the profession’s role in primary care. Participants engaged their skills, resources, and networks to gain entry onto a team. Constant communication about occupational therapy’s role was necessary to gain buy-in from interprofessional, primary care teams. Participants used activity analysis and patient-centered approaches to promote positive patient outcomes for some patients who would otherwise not be eligible for services. To expand national reach, occupational therapy practitioners and AOTA should work toward reaching a consensus on occupational therapy’s key contributions to and identity in primary care.
Footnotes
Acknowledgments
The authors have no funding or conflicts of interest to disclose.