
Abstract
A systematic review of occupational therapy interventions for the prevention and reduction of falls found mixed strengths of evidence for common interventions.
The Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014 (Pub. L. 113-185) was passed into law as an amendment to Title XVIII of the Social Security Act. One of the primary aims of the IMPACT Act was to standardize postacute care (PAC) assessment data to improve the quality of services and facilitate payment and discharge planning. This aim was to be achieved by requiring PAC providers to report standardized patient assessment data on designated assessment instruments (e.g., the Minimum Data Set [MDS] for skilled nursing facilities; Centers for Medicare & Medicaid Services [CMS], 2018) and to report data on quality, resource use, and other measures. The five quality domains are Skin integrity, Functional status and cognitive function, Medication reconciliation, Major falls, and Transfer of health information and care preferences when an individual transitions.
The three resource use and other measures domains are Resource use measures, including total estimated Medicare spending per beneficiary; Discharge to the community; and All-condition risk-adjusted potentially preventable hospital readmission rates (American Occupational Therapy Association [AOTA], n.d.; CMS, 2018).
These data inform the U.S. Congress about new and future payment models, are used to protect patient choice and access to care, and allow quality comparisons across providers (AOTA, n.d.).
The IMPACT Act continued a growing movement toward quality and value-based care, which is care that cuts costs while providing safe and effective intervention. Efforts to reform payment for health care services had been strengthened with the passage of the Patient Protection and Affordable Care Act (Pub. L. 111-148) in 2010, and CMS began reimbursing on the basis of value (quality) rather than volume of services provided (AOTA, n.d.).
Although AOTA has called on practitioners to contribute to measures demonstrating occupational therapy’s value to patients, the health care team, and reimbursement sources (AOTA, n.d.), few research articles have discussed the IMPACT Act and its influence on occupational therapy practice. Kroll and Fisher (2018) suggested that practitioners should collect data on functional performance to justify rehabilitation intensity in the PAC arena. Sandhu et al. (2018) advocated for practitioners to participate in data collection and analysis for the functional measures introduced by the IMPACT Act. DeJong (2016) explained that practitioners, in accordance with the IMPACT Act, must provide interventions that are supported by evidence and that reflect patient goals and societal values.
This article is Part 1 of a two-part systematic review of the effectiveness of occupational therapy interventions related to the quality and resource use domains of the IMPACT Act (see Feldhacker et al., 2022, for Part 2 of the systematic review). In Part 1, we focus on fall prevention and reduction, community discharge and reintegration, and prevention of hospital readmission. This summary of the evidence in the literature can inform practitioners, leaders, and researchers about the effectiveness of occupational therapy interventions in order to promote best practice, advocacy, and ongoing research in areas that relate to current health care and reimbursement trends.
Because falls among older adults are associated with decreased independence and quality of life (AOTA, 2017) and with substantial medical spending (Burns et al., 2016), fall prevention and reduction are a focus of both occupational therapy and reimbursement sources. CMS (2019b) has defined discharge to community as successful discharge of a patient to a community setting with no unplanned readmission. Occupational therapy practitioners have expertise in transition planning, which includes community discharge planning for persons, groups, and populations (AOTA, 2020). Because the role of occupational therapy in promoting community discharge and preventing readmission includes providing community reintegration services, we wanted to capture evidence related to reintegration as well. Rogers et al. (2017) reported that occupational therapy was the only profession whose services significantly reduced hospital readmission rates for people with heart failure, pneumonia, and acute myocardial infarction. Although this study explored outcomes in acute care settings, Roberts and colleagues (2020) subsequently argued that the study findings can help guide payment reforms in PAC settings through holistic practice emphasizing community engagement.
The focus of this systematic review was to evaluate the literature specific to interventions provided by occupational therapy practitioners to determine outcomes related to three areas of the IMPACT Act. We did not limit our literature search to services provided in PAC settings because we wanted to capture all occupational therapy intervention outcomes related to areas of the IMPACT Act. We felt that broadening our search to include any setting providing services to adult individuals, groups, or populations would allow us to better determine effectiveness and draw conclusions from the available research. The research questions for this study were as follows: What is the effectiveness of occupational therapy interventions in preventing and reducing falls among adults? What is the effectiveness of occupational therapy interventions in facilitating community discharge and reintegration for adults? What is the effectiveness of occupational therapy interventions in preventing hospital readmission for adults?
Method
Systematic review authors use an organized approach to collect and critically analyze research findings through qualitative synthesis (Portney, 2020). We used this approach to answer each of the three review questions.
Search Strategy
We began by determining criteria for searching the literature. We established search terms aligned with terms in the IMPACT Act (Table 1). A health science research librarian skilled in database searching conducted a thorough search of available literature at an academic institution. Databases included CINAHL, Cochrane, MEDLINE, PsycINFO, OTseeker, and Scopus. Databases were searched within “all fields,” and all search terms were exploded, when applicable, to locate as many articles as possible; articles were then limited by publication year and language. We included peer-reviewed articles published between 2009 and 2019 in English that described studies that included adult clients or populations receiving occupational therapy services, involved an occupational therapy practitioner as the interventionist (or member of the intervention team), and addressed the review question.
Key Terms and Search Terms
We used the Oxford Centre for Evidence-Based Medicine (2009) classifications for level of evidence. Articles selected for inclusion described intervention studies providing Level 1b, 2b, and 3b evidence; only if higher levels of evidence were not available did we consider articles describing studies with descriptive or nonintervention designs. To be included, studies had to report findings of occupational therapy intervention. We excluded systematic reviews and meta-analyses but hand searched the included articles and screened them for inclusion. Studies included in this review provide evidence at the following levels: Level 1b: well-designed randomized controlled trial (RCT) Level 2b: prospective cohort study, lower quality RCT, or two-group nonrandomized study Level 3b: retrospective case–control study, one-group nonrandomized pretest–posttest study, or cohort study Level 4: case series or low-quality case–control or cohort study.
Screening and Selection
We established the following operational definitions of terms to assist in selecting articles for inclusion in the review: Fall: an event in which a person inadvertently comes to rest on the ground, floor, or other lower level (World Health Organization [WHO], 2018) Community discharge: discharge to a residence in the community such as a private home, apartment, board and care home, assisted living facility, group home, transitional living program, or other type of residential care (CMS, 2019a) Community reintegration: return to family, vocational, and community life (AOTA, 2016) Readmission: admission to a hospital within 30 days after discharge for a reason that is considered unplanned and potentially preventable (CMS, 2019c).
In groups of two study authors, we independently screened articles for inclusion by sorting them into three categories (yes, no, or maybe) on the basis of title and abstract. We then met as a group to compare screening results and discussed any discrepancies between reviewers. We obtained the full text of articles categorized as yes or maybe and sorted them by review question in a shared file. In groups of two review authors, we independently screened all full-text articles to ensure they met all inclusion criteria and made a final determination of which to include. If two reviewers were unable to reach consensus on inclusion, a third reviewer (Whitney Lucas Molitor or Diana R. Feldhacker) reviewed the article, and together they reached an agreement on whether to include it in the review. Throughout the screening process, we documented the number of articles and duplicates and the reasons for exclusion, which are presented in Figure 1 (Moher et al., 2009).
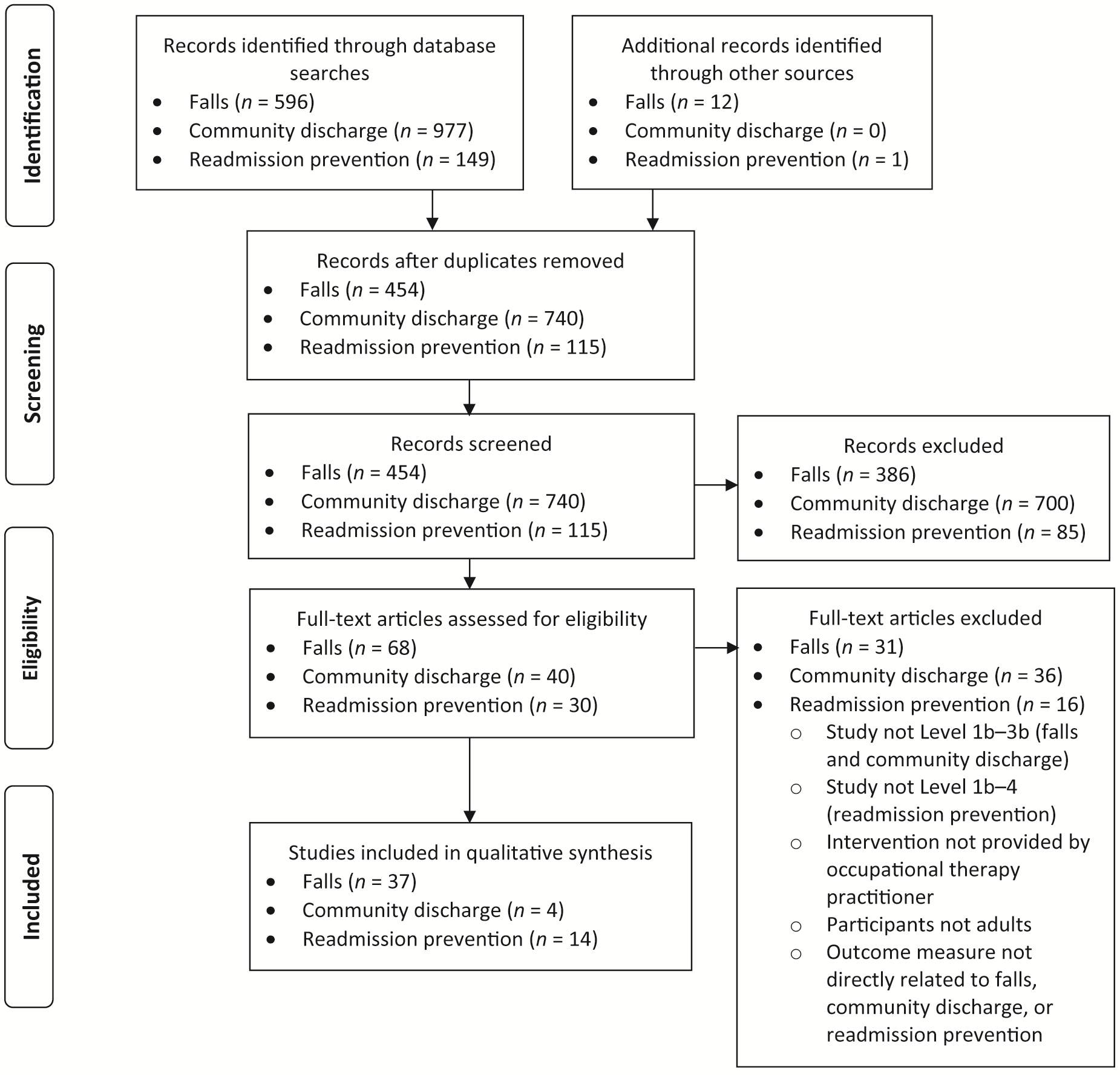
Flow diagram for inclusion and exclusion of studies in the systematic review.
Data Extraction and Quality Assessment
We divided the articles that met the inclusion criteria among all authors and individually extracted information into an evidence table (see Supplemental Appendix Table A.1, available online with this article at https://research.aota.org/ajot). We assessed articles for quality using the risk-of-bias format appropriate for the study design (Supplemental Appendix Tables A.2 and A.3; Higgins et al., 2016; National Heart, Lung, and Blood Institute, 2014). To ensure the quality of our results, a second author reviewed each assessment of risk of bias, and together the two authors reached an agreement on the ranking. For each domain of interest, we analyzed the populations, interventions, settings, and outcomes of the studies to establish themes agreed on by all authors. We assigned ratings for practice recommendations by theme on the basis of the study results for each theme.
Synthesis and Analysis
We used the U.S. Preventive Services Task Force (2018) recommendations as a guide in determining the level of certainty of our findings. We determined the strength of evidence in combination with the established risk of bias as follows: Strong: includes two or more well-designed and -conducted Level 1a or 1b studies that report consistent results. The findings are not likely to be questioned by the results of future studies. Moderate: includes at least one Level 1a or 1b high-quality study or multiple moderate-quality (Level 2a, 2b, 3a, or 3b) studies providing enough evidence to determine health outcomes. However, because these studies may have small sample sizes, lower quality, or inconsistency in findings across studies, the findings may be questioned in future research. Low: includes few low-level studies with flaws in design or high risk of bias, providing insufficient evidence to assess effects on health outcomes.
Results
We found 53 articles that met the inclusion criteria: 37 describe studies addressing the prevention and reduction of falls, 4 describe studies addressing community discharge and reintegration, and 14 describe studies addressing the prevention of hospital readmission. Two articles (Drummond et al., 2013; Lockwood et al., 2019) addressed both the falls and readmission prevention review questions. Details of the studies, sorted by question and theme, can be found in Supplemental Appendix Table A.1.
Fall Prevention and Reduction
For the review question on fall prevention and reduction, we found 20 Level 1b, 14 Level 2b, and 3 Level 3b studies. Outcomes generally included balance, falls, fall risk, and falls efficacy, but specific outcome and measurement tools varied.
Single Risk Factor
Thirteen studies (5 Level 1b, 7 Level 2b, 1 Level 3b) included interventions that targeted a single risk factor. Seven studies addressed physical risk for falling using exercise (including balance and vestibular training; Bell et al., 2011 , Level 2b; Cho et al., 2012, Level 2b), functional exercise (Burton et al., 2013, Level 1b; Clemson et al., 2010, Level 2b; Clemson et al., 2012, Level 1b), conditioning and balance training (Bhovad & Kale, 2015, Level 2b), and dual task training (Sahu et al., 2018, Level 2b). Results showed some improvements for participants in the intervention groups, but in general, between-group differences and sustained progress were inconsistent.
Five studies addressed environmental risk for falling using a home assessment (Chu et al., 2017, Level 1b; Johnston et al., 2010, Level 2b; Lockwood et al., 2019, Level 1b) or risk management and safety training (Finlayson et al., 2009, Level 3b; Waterman et al., 2016, Level 2b). These studies did not find significant differences between groups after intervention, despite reporting some short-term gains. One study included the single risk factor of nutrition (Beck et al., 2016, Level 1b). In a multidisciplinary intervention for older adults, an occupational therapist and a nutrition coordinator addressed dysphagia; however, no significant differences related to falls were reported.
In summary, low strength of evidence is available that interventions addressing a single fall risk factor can reduce falls.
Multiple Risk Factors
Twenty-four studies addressed multiple risks for falling. We divided the articles into two categories: (1) interventions that were customized to each participant and (2) those that followed a structured program (i.e., all participants received the same intervention).
Customized interventions
Nineteen studies (14 Level 1b, 5 Level 2b) examined interventions that were tailored to meet the individual needs of participants and addressed more than one risk for falls. Many of these studies were individualized by engaging the participant in a client-centered therapy process that included identification of meaningful goals. All but 6 of the studies involved a multidisciplinary team. Of studies that included an occupational therapist as the sole study interventionist, most found some improvements in fear of falling and home safety but no significant differences between groups (Ciaschini et al., 2009, Level 1b; Drummond et al., 2013, Level 2b; Fox et al., 2010, Level 1b; Hosseini et al., 2012, Level 2b; Sheffield et al., 2013, Level 1b; Whitehead et al., 2016, Level 2b).
Twelve studies incorporated an environmental component (home assessment, home modifications, or both) into interventions that addressed another risk factor such as cognitive training (Ciaschini et al., 2009, Level 1b), accessibility using assistive technology (Conroy et al., 2010, Level 1b), adaptive equipment training and client–family collaboration (Di Monaco et al., 2015, Level 1b; Neyens et al., 2009, Level 1b; Sheffield et al., 2013, Level 1b), safety education (de Vries et al., 2010, Level 1b; Drummond et al., 2013, Level 2b; Whitney et al., 2017, Level 1b), physical activity or exercise (Irvine et al., 2010, Level 1b; Mikolaizak et al., 2017, Level 1b; Wesson et al., 2013, Level 2b), or medication review (Fox et al., 2010, Level 1b). All studies found some within-group reduction in falls after intervention, yet many found no significant between-group differences.
In summary, studies of customized interventions addressing multiple risks for falls generally found similar outcomes between the intervention and control groups. Thus, low strength of evidence is available for customized interventions focused on fall risk prevention to reduce falls.
Structured interventions
Five studies (1 Level 1b, 2 Level 2b, 2 Level 3b) used a structured fall prevention program that incorporated multiple risks for falling. Structured fall prevention programs included Otago (Mackenzie & Clemson, 2014, Level 3b; Tan et al., 2018, Level 1b), Matter of Balance (Alexander et al., 2015, Level 3b), Community Aging in Place—Advancing Better Living for Elders (Szanton et al., 2011, Level 2b), and a modified Tai Chi program that incorporated balance, strength, and functional activities (Comans et al., 2010, Level 2b). Interventions took place over 6–8 wk and included a combination of environmental and physical (exercise and balance) risks for falls. Outcome measures were related to balance, self-reported falls, and falls efficacy (e.g., fear of falling). Falls efficacy generally was not improved as a result of the interventions; however, falls were reduced for participants who received the intervention in a community center.
In summary, low strength of evidence is available for the use of structured fall prevention programs to improve falls efficacy. Moderate strength of evidence supports community-based structured fall prevention programs to reduce falls.
Community Discharge and Reintegration
We included 1 Level 1b, 2 Level 2b, and 1 Level 3b studies that addressed community discharge and reintegration using two types of intervention: (1) education programming and (2) physical activity.
Educational Programming
Two studies (1 Level 2b and 1 Level 3b) examined multistep group interventions delivered in a community setting that involved a variety of educational components and aimed to improve community reintegration. Lee et al. (2017, Level 2b) found no significant differences in results after a six-session program compared with outpatient rehabilitation only. After a 10-session intervention, Lee et al. (2016, Level 3b) reported a significant improvement from pre- to postintervention for participants’ ability to find community resources and community support but found no significant improvements in self-efficacy and community living outcomes. These studies had small sample sizes and moderate risk for bias, and they reported differences in findings between studies.
In summary, low strength of evidence is available for interventions that incorporate educational programming to promote community discharge and community reintegration.
Physical Activity
Two studies incorporated physical activity into interventions. Although these studies also included other intervention strategies, they used a similar approach to group-based exercise. Mayo et al. (2015, Level 2b) reported improved engagement outside the home after the Getting on With the Rest of Your Life: Mission Possible program. Morrissey et al. (2012, Level 1b) reported similar differences between recuperative care and inpatient care groups at 3-mo and 12-mo follow-ups.
In summary, low strength of evidence is available for physical activity incorporated into interventions to promote community discharge and community reintegration.
Readmission Prevention
Fourteen studies (3 Level 1b, 1 Level 2b, 2 Level 3b, 8 Level 4) addressed readmission prevention and were categorized into four themes on the basis of participants’ condition: (1) stroke, (2) mental health conditions, (3) chronic conditions, and (4) hip fracture. In many, “typical” occupational therapy services, such as evaluation, ADL training, equipment provision, referral to community services, and discharge planning, were the intervention.
Stroke
Seven studies (1 Level 1b, 1 Level 2b, 5 Level 4) examined interventions aimed at preventing readmission of people with stroke. Two studies found lower readmissions for patients who received postdischarge outpatient therapy (Freburger et al., 2018, Level 4) and home health (Langstaff et al., 2014, Level 4). Drummond et al. (2013, Level 2b) and Clemson et al. (2016, Level 1b) reported no differences between intervention and control participants after a predischarge home visit. Three Level 4 studies (Andrews et al., 2015; Burke et al., 2014; Chang et al., 2018) found that patients who received typical occupational therapy were at lower risk for hospital readmission.
In summary, findings for interventions to prevent hospital readmission for people with stroke were inconsistent. Moderate strength of evidence supports occupational therapy provided in acute care and inpatient rehabilitation settings and predischarge home visits to reduce hospital readmission.
Mental Health Conditions
Two Level 3b studies examined the effects of occupational therapy interventions to reduce hospital readmission for people diagnosed with a mental health condition. Macritchie et al. (2019) and Shimada et al. (2016) used psychoeducation to address discharge planning and self-monitoring in addition to craft activities and motivational interviewing; at the conclusion of the studies, no participants had been readmitted.
In summary, insufficient evidence is available for interventions to prevent hospital readmissions among people with a mental health condition, so the strength of evidence is low.
Chronic Conditions
Four studies (1 Level 1b, 3 Level 4) examined interventions for people with a chronic condition other than stroke. Typical occupational therapy intervention (Nielsen et al., 2018, Level 1b; Rogers et al., 2017, Level 4; Wang et al., 2019, Level 4) and telehealth (Martin et al., 2017, Level 4) produced mixed results for readmission rates. In summary, low strength of evidence was found for occupational therapy to prevent hospital readmission for people with chronic conditions.
Hip Fracture
One well-designed Level 1b study (Lockwood et al., 2019) compared traditional occupational therapy combined with a predischarge home visit to traditional occupational therapy alone for people with hip fracture. The intervention group experienced fewer readmissions within the first 20 days postdischarge and at 30-day and 6-mo follow-ups. In summary, moderate strength of evidence supports occupational therapy to prevent readmission for people with hip fracture.
Discussion
We aimed to determine the effectiveness of occupational therapy interventions addressing three target areas of the IMPACT Act. Interventions that align with these areas can help keep adults safely in their homes and actively engaged in daily occupations. In turn, the cost of health care can be reduced, and the future focus of occupational therapy can shift more toward prevention rather than management of illness or disease.
The first target area we explored was prevention and reduction of falls. Occupational therapy practitioners work to prevent falls while facilitating older adults’ continued safe engagement in roles, occupations, and environments that are meaningful and important to them. Risks for falling include factors such as the environment, medications, and cognitive and mobility status (Panel on Prevention of Falls in Older Persons, 2011). The literature we reviewed focused on balance, fall risk, and falls efficacy. Interventions addressed a single or multiple risk for falling. Our findings align with those of a previous review (Elliott & Leland, 2018), which showed varied results but generally supported interventions addressing environmental safety and structured community fall risk prevention. Our study broadens Elliott and Leland’s (2018) findings by including all practice settings and adults age 18 yr and older.
The second target area we explored, facilitating discharge home and reintegration into the community, is often the goal of occupational therapy (Liu, 2018). Many older adults desire to remain at home to maintain their valued life roles, daily habits, and personal autonomy. A breakdown in the coordination of services between hospitals and community-based agencies has presented challenges with reintegration into the community (Guerin et al., 2013), and overcoming such challenges is critical for successful community discharge. Educational programming using a health promotion approach can help enable clients to take control of their health (Lee et al., 2016, 2017; Morrissey et al., 2012). In a systematic review of health promotion, management, and maintenance interventions, Berger and colleagues (2018) found that clients’ success in health self-management was supported by their ability to learn new skills and implement new habits. By including leisure, social participation, and physical exercise in group and individual interventions, occupational therapy practitioners can help older adults remain at home, aging in place as productive members of their communities (Liu, 2018).
The third target area we explored was preventing hospital readmissions after discharge. Hospital readmissions increase health care spending, often result in a decline in patients’ functional status, and can lead to poorer health outcomes (Greysen et al., 2015). The increasing age of the U.S. population brings a higher rate of chronic illness and greater complexity in managing health and keeping people out of the hospital. Our review supports previous literature indicating that readmissions are best prevented by providing health condition education, implementing community- and home-based services after discharge, and emphasizing transitional care (Kripalani et al., 2014; Rennke & Ranji, 2015). Many studies in this review examined the effectiveness of occupational therapy interventions that focus on functional retraining of daily activities evaluation, ADL training, equipment provision, and referral to community services along with discharge planning. Leppin and colleagues (2014) also studied hospital readmission, finding that functional status in self-care tasks was an important predictor in readmission rates.
Study Limitations and Strengths
The findings of this systematic review are limited by the variety of interventions examined in included studies, which limits the evidence available for each type of intervention. In addition, many of the studies we included to answer the fall prevention question used a control group that received typical occupational therapy intervention, limiting our ability to identify which intervention produced the results. Because of the limited number of studies, we used Level 4 evidence to answer the readmission prevention question. The review was strengthened by the inclusion criterion that an occupational therapy practitioner carried out or was a member of the team that provided therapeutic interventions, as well as by the participation of five authors, which supported thoroughness in data extraction and qualitative synthesis.
Implications for Occupational Therapy Practice
Our practice recommendations based on this review are supported by low strength of evidence, so occupational therapy practitioners should consider these recommendations in light of their clinical judgment and the client’s goals. Staying current on health care policy and legislation can help practitioners maintain the future viability of the profession and meet societal health care needs. Further research is needed that explores community-based models of service delivery that address the impact of clients’ context on the three outcomes of interest in this review—falls, community discharge and reintegration, and hospital readmission—while also offering new opportunities for occupational therapy practice. In addition, this review has the following implications for practice: To reduce or prevent falls, occupational therapy interventions should routinely incorporate functional exercise, participation of a multidisciplinary team, and structured community-based fall prevention approaches. To facilitate community discharge and reintegration, practitioners should combine educational programming and physical activity with additional interventions that are supported by moderate and strong strength of evidence. To prevent unplanned hospital readmissions, occupational therapy practitioners should assist in facilitating discharge to the community and provide interventions based on the client’s condition that are supported by strong strength of evidence.
Conclusion
The findings of this systematic review address three areas of the IMPACT Act. We reviewed the evidence on what occupational therapy practitioners are currently doing to address three areas of this act, highlighting strengths and ideas for future research. Occupational therapy interventions aiming to help clients reduce or prevent falls, navigate discharge and reintegrate into the community, and avoid hospital readmissions will support clients’ occupational participation and improve their health outcomes, ultimately securing the value and worth of the occupational therapy profession now and into the future. Continued work to highlight the value of occupational therapy is critical in the current health care landscape, in which payment is being reduced and competition among health professions is increasing. Future research should focus on examining not only the effectiveness of novel occupational therapy interventions that lead to value-based outcomes, but also the longstanding, foundational interventions of occupational engagement and client-centered care.
Supplemental Material
Supplementary material for Occupational Therapy and the IMPACT Act: Part 1. A Systematic Review of Evidence for Fall Prevention and Reduction, Community Discharge and Reintegration, and Readmission Prevention Interventions
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.049044.pdf for Occupational Therapy and the IMPACT Act: Part 1. A Systematic Review of Evidence for Fall Prevention and Reduction, Community Discharge and Reintegration, and Readmission Prevention Interventions by Whitney Lucas Molitor, Diana R. Feldhacker, Helene Lohman, Angela M. Lampe and Lou Jensen in The American Journal of Occupational Therapy
Footnotes
*
Indicates articles included in the systematic review.
Acknowledgments
All authors participated in the conceptual design of the study, engaged in data collection, and were involved in drafting and editing of this review. None of the authors declare competing financial interests. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.