
Abstract
In a review of EHR data, the authors found that although acute care occupational therapy utilization was driven partly by patient need, potential disparities in access to beneficial services may exist across sociodemographic characteristics and insurance type.
A primary indicator of quality acute care is a safe discharge to the community (Centers for Medicare & Medicaid Services [CMS], 2019a). Many hospitalized patients experience functional limitations that may undermine a safe community discharge, including diminished performance of activities of daily living (ADLs; Giral et al., 2018; Müller et al., 2011), defined as activities completed on a routine basis that enable care of oneself (e.g., bathing; American Occupational Therapy Association, 2020). Occupational therapists enable a safe discharge plan by analyzing barriers to and facilitators of community-based living for patients with ADL limitations (Jette et al., 2009, 2014a). Moreover, acute care rehabilitation services improve ADL performance, shorten lengths of stay, and limit hospital readmissions (Peiris et al., 2018; Rogers et al., 2017). As such, hospitalized patients who would benefit from occupational therapy should receive timely access to these essential services.
Health care access refers to the extent to which patients use health services they need; disparities in access occur when factors independent of their need influence service utilization (Anderson et al., 2014). Although some studies have indicated that patients with greater need are more likely to receive acute care rehabilitation (Freburger et al., 2012), evidence suggests disparities in access. For example, some studies have indicated that race/ethnicity (Freburger et al., 2012, 2018) and insurance type (Freburger et al., 2012; Kumar et al., 2019; Prohaska et al., 2019) predict receipt of acute care rehabilitation. Nonetheless, our knowledge of disparities in access to acute care rehabilitation remains insufficient.
The relatively few studies that have examined acute care occupational therapy utilization have frequently used proxy indicators of patient need that have a limited ability to reflect primary targets of occupational therapy intervention. For example, comorbidity burden is often used as an indicator of need for occupational therapy (Kinney et al., 2021); however, comorbidity burden is weakly associated with ADL performance in hospitalized patients (Kumar et al., 2016), undermining arguments in favor of its ability to reflect patient function, a primary target of occupational therapy services. To more accurately depict disparities in occupational therapy utilization, there is a need for studies that more directly measure patient need for occupational therapy (e.g., actual ADL performance). Moreover, many studies consider occupational therapy utilization as receipt of an evaluation for services (e.g., Kinney et al., 2021). Although such research is important to gain an understanding of potential disparities in access to evaluative occupational therapy services, there is a need for studies that examine predictors of subsequent treatment. Understanding disparities in access to occupational therapy treatment can inform the development and testing of strategies targeting the multilevel factors (e.g., sociopolitical, organizational) that underlie access inequities (Woodward et al., 2019).
The purpose of this study was to investigate whether the relationship between patient need and acute care occupational therapy treatment utilization is moderated by predisposing and enabling factors. We hypothesized that patients with lower ADL performance would be more likely to receive occupational therapy and that this relationship would differ depending on patients’ sociodemographic characteristics and insurance type.
Method
Data Source and Participants
A retrospective cross-sectional study of de-identified patient data was conducted to describe occupational therapy utilization across five acute care hospitals within a health system. Data came from electronic health records obtained from 212,767 patients discharged between June 2014 and June 2018. Data were included if the patient had received an evaluation for occupational therapy services, was an adult (age ≥18 yr), was admitted to inpatient acute care (excluding observation stays), was not hospitalized for giving birth, did not die during hospitalization, and had complete data for the variables of interest. When a patient had multiple admissions, their first admission was used as the index hospitalization. These data were validated, de-identified, organized, and provided to us by an enterprise data warehouse affiliated with the health system. Inclusion criteria were met by 56,022 adults (Figure 1). A signed data use agreement was in place, and the study was approved by the local institutional review board.
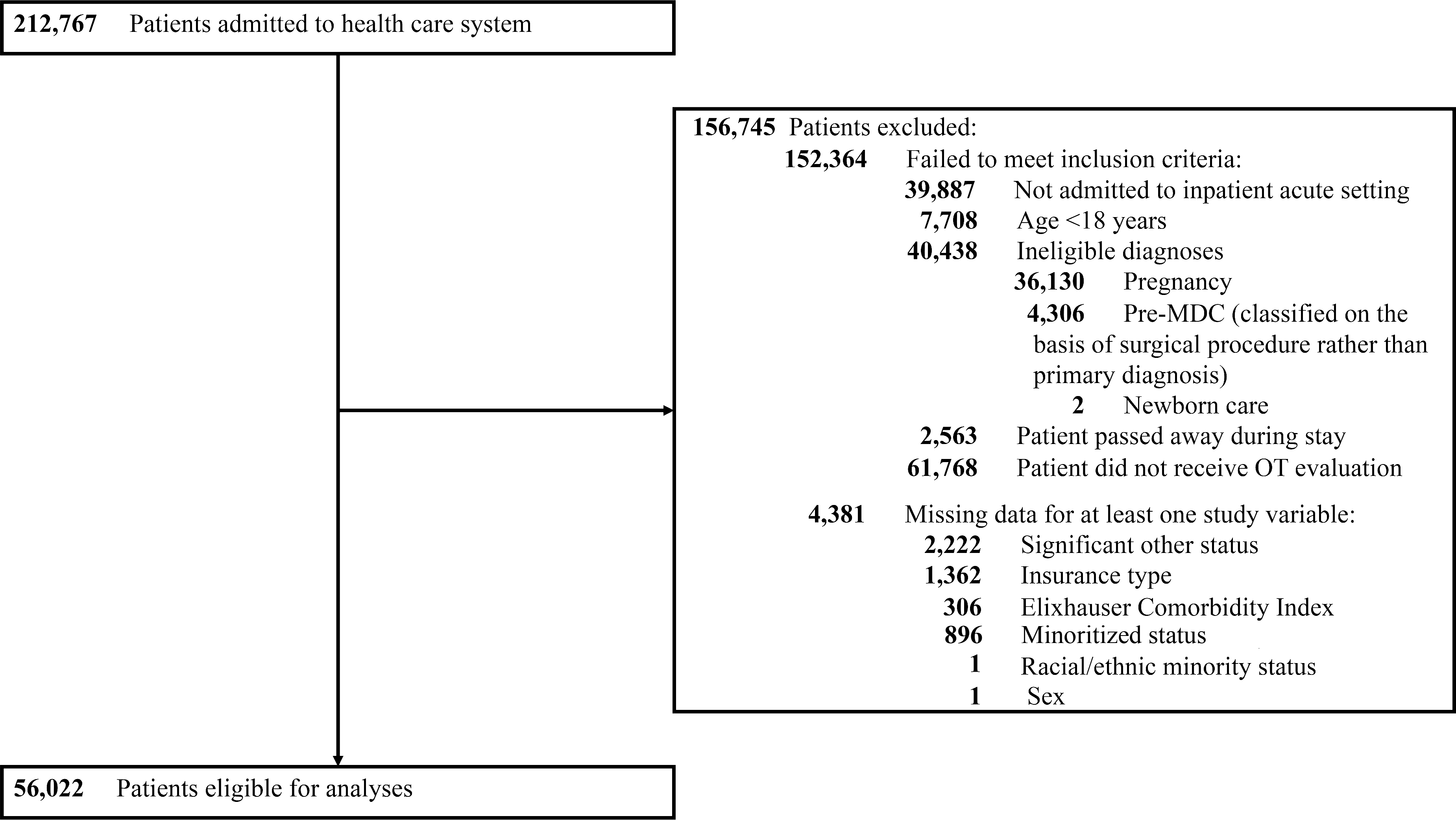
Diagram illustrating cohort selection.
Conceptual Framework
We used the Behavioral Model of Health Services Use as a conceptual framework (Anderson et al., 2014). According to this model, in an equitable health care environment patient need (e.g., ADL performance) drives health care utilization (e.g., acute care occupational therapy). Access disparities exist when predisposing factors, enabling factors, or both explain health care utilization. Predisposing factors are conditions that influence health care utilization yet are not directly related to service need (e.g., sociodemographic characteristics). Enabling factors are forces that facilitate or obstruct utilization of beneficial services (e.g., insurance type).
Measures
Sociodemographic Characteristics (Predisposing Factors)
The following sociodemographic characteristics were examined: age (yr), sex (female, male), significant other status (yes/no), and minoritized status (no [white, non-Hispanic]; yes [e.g., Black; Hispanic/Latino]). The term minoritized was intentionally used to underscore the systemic forces that shape racial/ethnic status (see Sotto-Santiago, 2019).
Insurance Type (Enabling Factor)
Insurance type was included as an enabling characteristic. Five insurance types were included: (1) private, (2) Medicare/Medicare Advantage, (3) Medicaid, (4) Department of Veterans Affairs (VA), and (5) workers’ compensation.
Performance of Activities of Daily Living (Need)
The Activity Measure for Post-Acute Care (AM-PAC) “6-Clicks” measure of daily activity was used to assess performance of ADLs (Haley et al., 2004). Occupational therapists rate patient performance on the basis of assistance needed on a scale ranging from 1 (Total) to 4 (None) for six ADLs: (1) upper body dressing, (2) lower body dressing, (3) bathing, (4) toileting, (5) grooming, and (6) eating (Jette et al., 2014b). Values are summed, and raw scores are standardized (Jette et al., 2014b), with higher scores indicating greater ADL performance (range = 17.07–57.54). The measure has been validated in the hospital setting (Jette et al., 2014b) and has good interrater reliability (Jette et al., 2015). We used the baseline AM-PAC score (i.e., score derived during evaluation) because it reflects functional status during the initial clinical encounter, which is critical for acute care occupational therapy decision making (Jette et al., 2003).
Covariates
Primary diagnosis, comorbidity burden, and length of stay were included as covariates. Primary diagnosis was categorized using procedures previously reported (Kinney et al., 2021). In brief, the International Classification of Diseases 9th revision and 10th revision (ICD–9 and ICD–10; World Health Organization, 1996, 2004) codes for admission diagnosis were first categorized into the 25 Major Diagnostic Categories (MDC; CMS, 2019b). Three investigators independently collapsed eligible MDC into a smaller number of categories and achieved a consensus (Table 1). The Elixhauser Comorbidity Index was used to measure comorbidity burden (Elixhauser et al.,1998). The package (Wasey et al., 2019) was used to identify relevant comorbidities, and the Elixhauser Comorbidity Index was constructed according to Moore et al.’s (2017) guidelines. Length of stay was assessed by calculating the number of days between admission and discharge.
Descriptive Statistics: Participant Characteristics and Occupational Therapy Utilization (N = 56,022)
Note. ADL = activities of daily living; OT = occupational therapy; VA = U.S. Department of Veterans Affairs.
Outcome
Occupational therapy utilization was defined by determining whether the patient had been billed for any occupational therapy treatment (after the evaluation) during the acute care stay (yes/no).
Data Analysis
All analyses were performed using R (Version 3.6.2). Descriptive statistics for study variables were calculated within the total sample and stratified by occupational therapy utilization. The presence of patient clustering within hospitals was first considered by calculating the intraclass correlation coefficient (ICC) using the ICC package in R (Wolak, 2015). Given the relatively low ICC (.04), in addition to the small number of clusters (k = 5), mixed effects modeling was deemed unnecessary (Nezlek, 2008). Accordingly, two logistic regression models were specified to explain the binary indicator of occupational therapy utilization. The following independent variables were included in the first model: sex, age, significant other status, minoritized status, insurance type, and ADL performance. Primary diagnosis, comorbidity burden, and length of stay were included as covariates in the model. The second model additionally included interaction terms between (1) ADL performance and (2) sex, age, significant other status, minoritized status, and insurance type. Significant interactions were visually examined using the interactions R package (Long, 2019). A significance level of α = .05 was used to evaluate significance for all parameter estimates.
Results
Slightly fewer than half of the patients who received an occupational therapy evaluation received subsequent occupational therapy treatment (43.6%). The sample was evenly distributed with respect to sex (women = 51.0%), and the average age was 65.5 (SD = 16.5). Among all patients, the most prevalent primary diagnoses were conditions related to the musculoskeletal system (31.3%; see Table 1).
Model Excluding Interactions
As hypothesized, patients with lower ADL performance were more likely to receive occupational therapy treatment. Greater odds of receiving occupational therapy treatment was also associated with younger age; the presence of a significant other; and being White, non-Hispanic. Paying for care with private insurance was associated with higher odds of receiving occupational therapy treatment relative to Medicare/Medicare Advantage, Medicaid, and VA (Table 2).
Logistic Regression Models Explaining Occupational Therapy Utilization (N = 56,022)
Note. Age, Elixhauser Comorbidity Index, and ADL performance are mean centered. — = not applicable; ADL = activities of daily living; BIC = Bayesian Information Criterion; CI = confidence interval; OR = odds ratio; OT = occupational therapy; Ref. = reference category.
Model Including Interactions
The relationship between ADL performance and occupational therapy utilization also differed across sociodemographic characteristics and insurance type. Among patients with low ADL performance, those who were younger; were White, non-Hispanic (vs. racial/ethnic minorities); had a significant other (vs. not having one); and had private insurance (vs. Medicaid, Medicare/Medicare Advantage, and VA) were more likely to receive occupational therapy treatment. These differences diminished among patients with greater ADL performance, who had similarly low probabilities of receiving occupational therapy treatment (Figure 2). Although statistically significant, a probing of the interaction between ADL performance and sex revealed a negligible effect (to visually examine this effect, see Supplemental Figure 1, available online with this article at https://research.aota.org/ajot).
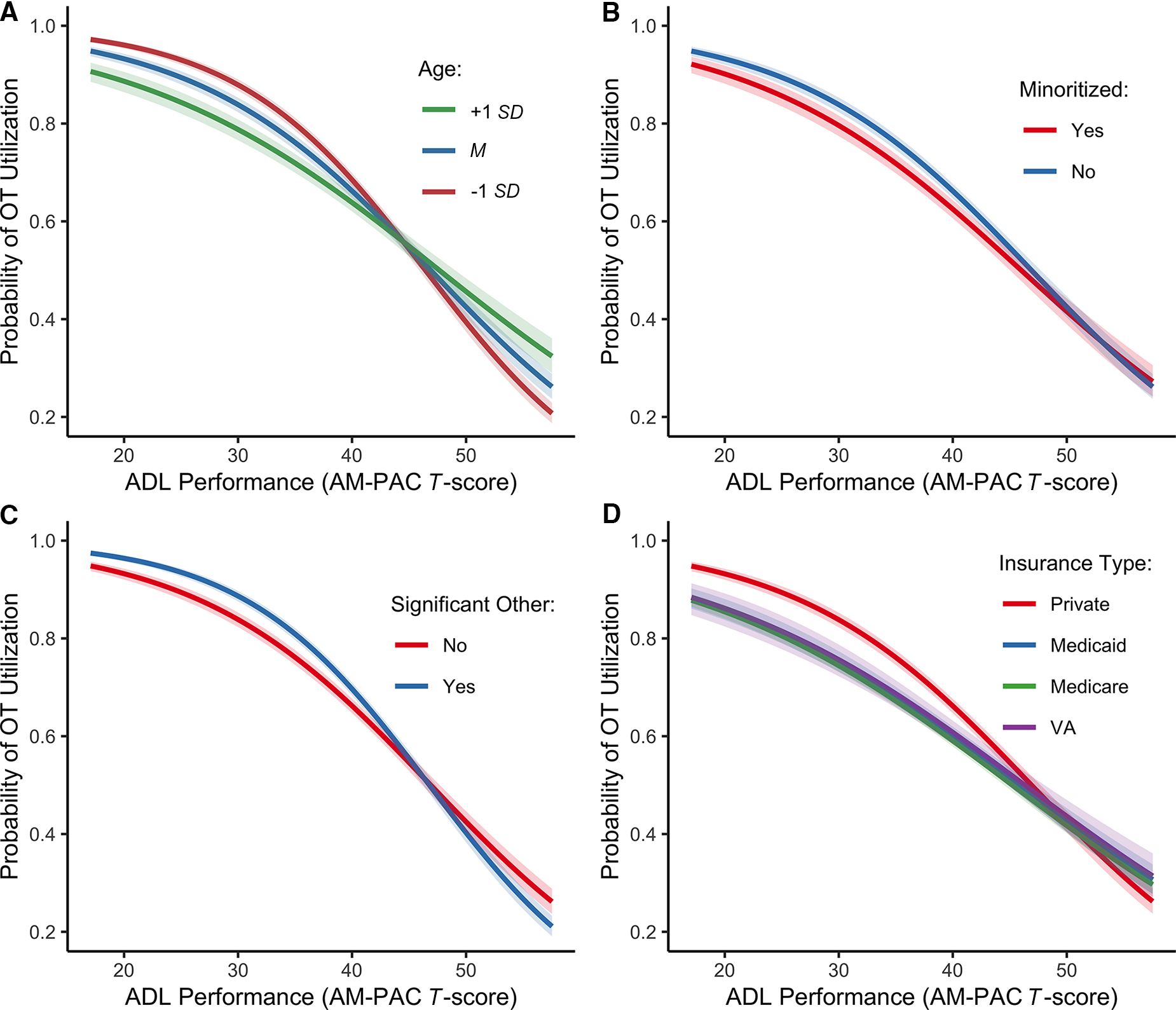
Illustration of the interactions between ADL performance and predisposing enabling factors.
Discussion
We examined whether the relationship between ADL performance and acute care occupational therapy utilization is moderated by sociodemographic characteristics and insurance type. Among patients who received an occupational therapy evaluation, those with lower ADL performance were more likely to receive subsequent treatment, but this relationship differed according to age, minoritized status, significant other status, and insurance type. To be clear, not every patient with poor ADL performance would necessarily benefit from occupational therapy treatment. Therapists’ evaluation of clinical factors unavailable for the current study (e.g., prior level of social support) informs decisions regarding appropriate receipt of services. Nonetheless, our findings offer direction for future explorations of the specific determinants of disparities in access to services.
Our results indicate that, among patients with low ADL performance, younger age was associated with greater odds of receiving occupational therapy treatment. This finding stands in contrast to prior research indicating that older patients are more likely to receive acute care rehabilitation (e.g., Freburger et al., 2012; Kinney et al., 2021). This conflicting finding may be explained by patients’ preadmission living situation. Older adults with low ADL performance in our sample may represent those already receiving needed support for safely completing their daily routine. As such, they may appear to have limited therapy potential (Jette et al., 2003), and younger patients with functional deficits for whom an independent return to the community is necessary may be prioritized for occupational therapy treatment. Moreover, implicit bias among health care providers associated with patient age has been shown to influence care processes (FitzGerald & Hurst, 2017). Thus, the role of therapist decisions as being based on perceptions of patient age, rather than a need for skilled services, cannot be ruled out. Future research should examine potential mechanisms underlying the observed age-related disparities in access to acute care occupational therapy.
The relationship between ADL performance and occupational therapy utilization was also moderated by minoritized status, such that minoritized patients with low ADL performance were less likely to receive occupational therapy relative to their White, non-Hispanic counterparts. This finding aligns with prior studies indicating that minoritized patients are less likely to receive acute (Freburger et al., 2018) and postacute (Asemota et al., 2013; Gregory et al., 2006; Holmes et al., 2012; Menendez & Ring, 2014) therapy. Moreover, it aligns with well-documented racial and ethnic disparities in access to quality care, the perpetuation of which is enabled by bias at the levels of the provider, institution, and health system as a whole (i.e., structural racism; Nelson, 2002). Should the disparities observed in this study be replicated in other health systems, future research should target the mechanisms by which these disparities occur. Such research can inform the development of strategies that target the multilevel sources of racial and ethnic disparities in access to occupational therapy services (Woodward et al., 2019).
Patients with significant others and low ADL performance were more likely than their counterparts without significant others to receive occupational therapy treatment. This finding conflicts with a prior study indicating that, among patients with a higher level of therapy need, those with significant others were less likely to receive acute care occupational therapy (Kinney et al., 2021). These discrepant findings may be explained by differences in how therapy need was measured. The prior study used a proxy indicator of need for therapy (i.e., fall risk), whereas the present study was able to more directly assess patient need using a measure of ADL performance, a construct central to clinical decision making in acute care occupational therapy (Jette et al., 2014a). Thus, the present study may more accurately describe the interactive effect of patient need and significant other status on acute care occupational therapy utilization. Families are active participants in decisions germane to acute care occupational therapy (Jette et al., 2003). Significant others may advocate on patients’ behalf or offer information that complements the patient perspective, thereby revealing novel intervention targets and maximizing the likelihood of receiving occupational therapy treatment. These findings should be replicated in other health systems to better understand whether patients with functional impairments, but no significant other, experience reduced access to beneficial acute care occupational therapy.
The relationship between ADL performance and acute care occupational therapy utilization also differed across insurance types. Among patients with low ADL performance, those with private insurance were more likely than those with public forms of insurance to receive occupational therapy treatment. This finding aligns with those of previous studies indicating that insurance type is associated with utilization of acute (Freburger et al., 2012; Kinney et al., 2021; Kumar et al., 2019; Prohaska et al., 2019) and postacute (Asemota et al., 2013; Freburger et al., 2018; Greene et al., 2015; Menendez & Ring, 2014) occupational therapy. Some have proposed that because insurance type is associated with certain health characteristics, it may function as a proxy indicator for unmeasured health-related factors that drive health service utilization (Freburger et al., 2012; Pollack et al., 2007; Shen & Washington, 2007). We used ADL performance, a direct indicator of occupational therapy need, thereby diminishing the likelihood that unmeasured clinical factors related to insurance type were responsible for observed differences in occupational therapy utilization. Therapists in acute care settings acknowledge that structural features of the health care system (e.g., patient insurance status) influence discharge recommendations (Jette et al., 2003). Future research is needed to understand whether therapist decisions regarding the appropriateness of treatment are also shaped by patient insurance status. Data regarding acute care occupational therapy utilization among noninsured patients were unavailable for this study. Future research should examine the effect of insurance status (i.e., insured vs. noninsured) on access to beneficial occupational therapy services.
Additional research within other health systems may provide evidence of disparities in acute care occupational therapy utilization across sociodemographic characteristics and insurance type. Assuming successful replication of findings, future research should apply an implementation science perspective to reveal specific drivers of potential disparities in acute care occupational therapy utilization. For example, the Health Equity Implementation Framework describes potential determinants of health care disparities at multiple levels (e.g., the health care system; Woodward et al., 2019). Understanding such determinants may inform the selection of implementation strategies that maximize access to acute care occupational therapy services among those who would benefit (Waltz et al., 2019). See Juckett et al. (2019) for a detailed discussion of selecting implementation strategies for occupational therapy services.
Study Limitations
This study has some limitations that should be noted. First, we were unable to capture all relevant predisposing and enabling factors. For example, the Behavioral Model of Health Services Use (Anderson et al., 2014) highlights contextual factors (e.g., home environment) that are worthy of investigation. Second, our study was limited to one health system, thus diminishing the generalizability of our findings to other care delivery systems. The results should be replicated in other health systems to determine whether they translate to geographically and socioeconomically diverse patient populations. Third, we used a dichotomous indicator of minoritized status to assess race and ethnicity, thereby precluding the assessment of potential variability within disparate racial and ethnic groups. Similarly, our operational definition of insurance type may have obscured potential variability (e.g., Medicare vs. Medicare Advantage). Understandings of potential disparities in access to occupational therapy would be bolstered by an evaluation of such heterogeneity in regard to race/ethnicity and insurance type. Fourth, we are unable to rule out the influence of variables that may confound observed relationships, including receipt of intensive care, health-related complications, patient income, patient perceptions, and premorbid social support. Last, as is the case when one is evaluating electronic health record data, coding and reporting errors may exist.
Implications for Occupational Therapy Practice
Our findings have the following implications for occupational therapy practice: Acute care occupational therapy utilization is driven by clinical need, but researchers, practitioners, and policymakers must be aware of potential disparities in patient access to beneficial services. Specific determinants of disparities in access require further study to inform practice and policy that maximize receipt of beneficial services.
Conclusion
We examined whether the relationship between patient need and utilization of acute care occupational therapy was moderated by predisposing and enabling factors. Although patients with lower ADL performance were more likely to receive occupational therapy treatment, this relationship varied according to age, minoritized status, significant other status, and insurance type. Further research is warranted to verify these relationships in health systems that serve geographically and socioeconomically diverse patient populations, thus informing practice and policy initiatives.
Supplemental Material
Supplementary material for Activities of Daily Living Performance and Acute Care Occupational Therapy Utilization: Moderating Factors
Supplementary material, sj-docx-1-aot-10.5014_ajot.2022.049060.docx for Activities of Daily Living Performance and Acute Care Occupational Therapy Utilization: Moderating Factors by Adam R. Kinney, James E. Graham, Rayyan Bukhari, Amanda Hoffman and Matt P. Malcolm in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This work was not supported by the Veterans Health Administration, and the views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the U.S. Department of Defense, U.S. Department of Veterans Affairs, or the U.S. government.