
Abstract
Limited, moderate-quality evidence, primarily for interventions using cognitive and behavioral strategies, exists within the occupational therapy scope of practice for addressing depressive and anxiety symptoms within the physical disability IPR setting.
The disability adjustment process often begins in the inpatient rehabilitation (IPR) setting after discharge from acute care services in the hospital (Jesus & Silva, 2016). In the IPR therapy setting, skilled rehabilitation-focused medical care is provided to support independence with activities of daily living (ADLs; Forrest et al., 2019). The IPR setting consists of a multidisciplinary health care team—including physical, speech, occupational, and recreational therapies; social work; rehabilitation psychology; case management; physiatry; and nursing—working together to promote physical and mental health recovery (Forrest et al., 2019). The Centers for Medicare & Medicaid Services (CMS) require that patients in IPR receive 180 min of therapy per day, 5 days per week (Forrest et al., 2019). This minute requirement often makes IPR the most time- and cost-intensive therapy setting (Forrest et al., 2019). Because the average length of stay (LOS) in an IPR facility is 16 days, the goal of IPR is to maximize recovery and prepare the patient for a safe discharge from the IPR facility as quickly as possible (Forrest et al., 2019; Graham et al., 2013).
Because time is of the essence in the costly and intensive IPR setting, maximizing productive time spent in therapy is vital to promoting functional recovery and participation in meaningful occupations. However, adjustment to disability can be emotional and challenging. Depressive and anxiety symptoms are common among IPR patient populations, affecting between one in three and one in four of all individuals living with physical disability (Crichton et al., 2016; Livneh et al., 2019; Peterson et al., 2019). Further, it is well documented that experiencing depressive and anxiety symptoms during IPR adversely affects recovery, including functional outcomes of occupational participation and engagement (Graham et al., 2013 ; Singh et al., 2009; White et al., 2010).
Those who experience depressive and anxiety symptoms are at increased risk for poor adjustment to disability and have increased mortality (Cree et al., 2020; Dossa et al., 2011; Graham et al., 2013 ; White et al., 2010). The behavioral manifestations of depressive and anxiety symptoms, such as irritability, apathy, and difficulty concentrating, can negatively affect a patient’s ability to actively engage with and participate in the rehabilitation process, thereby negatively affecting the ability to participate in meaningful occupations. These symptoms may potentially fuel disparities in recovery documented in the literature between patients who do and do not have depressive and anxiety symptoms (Dobrez et al., 2010).
Current recommended treatments for depressive and anxiety symptoms (medication typically managed by the attending physiatrist and talk-based psychotherapy, often delivered by either social work or rehabilitation psychology) have minimal effects on enhancing functional independence, particularly among neurologically affected populations (Clarke & Currie, 2009; Cree et al., 2020; Gillespie et al., 2011; Hees et al., 2013; Hofmann et al., 2012 ; Villa et al., 2018 ; Waldron et al., 2013). Many aspects of IPR may not be conducive to positive mental health because patients have reported experiencing loneliness and boredom during downtime, prioritization of physical health needs over mental health needs, and frequent sleep disturbances (Luker et al., 2015; Simpson et al., 2018). Moreover, patients have reported disappointment over a lack of coordination among health care team members regarding their mental health care (Peoples et al., 2011; Simpson et al., 2018).
Treating depressive and anxiety symptoms, even within the IPR setting, where a team-based multidisciplinary treatment perspective is maintained, has proven to be a difficult task. Therefore, it is important to consider the unique treatment outlook of all qualified professions, including the perspectives that occupational therapy practitioners can provide to enhance functional outcomes among patients affected by physical injury or disability (Simpson et al., 2018).
Rationale
Although rehabilitation psychology, physical medicine rehabilitation, and social work may also be used to address mental health in IPR, occupational therapy practitioners offer a unique and holistic view of medical care by minimizing adverse physical and mental health effects on function and participation in ADLs (American Occupational Therapy Association [AOTA], 2020). Occupational therapy practitioners may address depressive and anxiety symptoms by embedding the treatment of adverse mental illness symptoms within the context of a meaningful and goal-oriented activity, such as using problem-solving therapy while completing simple meal preparation (Hildebrand, 2015). The central perspective of occupational therapy practitioners in addressing depressive and anxiety symptoms is to facilitate patient engagement in meaningful and enjoyable occupations to support mental health and minimize the interference of adverse symptoms on participation (AOTA, 2020).
Occupational therapy is vital to the management of depressive and anxiety symptoms by being uniquely qualified to address both physical and mental health. Occupational therapy practitioners approach treatment through activity analysis and a focus on comprehensively treating physical, cognitive, and mental health to support meaningful participation (AOTA, 2020). Through such perspectives, the occupational therapy profession can augment the team-based approach to mental health care provided in IPR to support comprehensive health and functional recovery (AOTA, 2020).
Research, however, suggests that occupational therapy practitioners report several barriers that may negatively affect their delivery of mental health care, such as institutional barriers (e.g., limited time, increased productivity standards, expectations to facilitate physical recovery over mental recovery, concerns about insurance reimbursement for mental health services) and educational barriers (e.g., lack of training to address mental health issues in a non–mental health setting; Simpson et al., 2018). Limited research has examined interventions within the occupational therapy scope of practice for addressing depressive and anxiety symptoms among physically affected patient populations (Gutman & Raphael-Greenfield, 2014). Even less literature has examined setting-specific strategies across diagnostic groups (Gutman & Raphael-Greenfield, 2014). Exploration of interventions within the occupational therapy scope of practice is warranted given reported patient and provider dissatisfaction over current standards of care (Simpson et al., 2018).
Objective
Systematic exploration of the literature is needed to (1) understand the role of occupational therapy in addressing depressive and anxiety symptoms in IPR, (2) inform future interventions in the setting, (3) support the effectiveness of occupational therapy practitioners in implementing high-quality mental health care among physically affected populations, and (4) inform best practice specific to the intensive physical disability IPR setting. Exploration of IPR was chosen to identify strategies most effective for supporting mental health, functioning, and adjustment to disability, relative to stage of recovery (Brenner et al., 2019). Therefore, the objective of this systematic review was to identify interventions within the occupational therapy scope of practice for addressing depressive and anxiety symptoms in the IPR therapy setting and to determine the efficacy of these interventions for mental health, quality of life, and functional outcomes. The following elements composed the PICO research question for this study: The population (P) was IPR patients with physical impairments, the interventions (I/C) were treatments within the occupational therapy scope of practice, and outcomes of interest (O) were depressive and anxiety symptoms.
Method
Search Methods
After formation of the PICO research question, a health science librarian was consulted for development of the search strategy. Literature searches were conducted for nine databases: PubMed, Embase, Web of Science, Scopus, PsycINFO, AgeLine, CINAHL, Cochrane Library, and OTseeker. Medical Subject Headings (MeSH) terms were developed for each respective database by the health sciences librarian (Table 1). Full search strategies are available on request. Alerts were established for each respective database in the event of new, relevant publications. The hand literature search was completed through Google Scholar review, bibliographic review of included article references, and journals relevant to the topic (Archives of Physical Medicine and Rehabilitation, Occupational Therapy Journal of Research, Rehabilitation Psychology, and American Journal of Occupational Therapy). A second search of the literature was conducted in December 2020 to ensure the thoroughness of the review and to identify any additional articles published during the review process. OTseeker was not searched again because the database was no longer being updated.
Overview of MeSH Terms and Key Words Used in the Literature Search
Note. IPR = inpatient rehabilitation; IRF = inpatient rehabilitation facility; MeSH = Medical Subject Headings; OT = occupational therapy.
Study Selection
The article review process was conducted and managed with Covidence (Melbourne, Victoria, Australia) literature management software (Polanin et al., 2019). The authors served as reviewers for article screening and data extraction. They independently completed title and abstract screens, with discrepancy resolved through consensus. The same process was repeated for full-text screening. The reviewers held regular biweekly meetings throughout the review process to resolve discrepancies and to address any ongoing concerns. Articles were included on the basis of the following eligibility criteria: Publication type (written in English, full text, U.S.-based peer-reviewed articles, all years) Study design (randomized or clinical controlled trials) Setting (physical disability IPR) Intervention type (within the occupational therapy scope of practice per the Occupational Therapy Practice Framework: Domain and Process [4th ed.; OTPF–4;
AOTA, 2020]) Population (age ≥16 yr, any race–ethnicity and gender) Outcomes (measures of depressive or anxiety symptoms, excluding psychotic features, with a primary physical disability diagnosis that would qualify for IPR admission per CMS guidelines).
Articles including interventions delivered by all service providers in IPR were considered for inclusion if the intervention was within the occupational therapy scope of practice and could be provided by an occupational therapy practitioner, as defined in the OTPF–4. Moreover, articles were included if interventions were completed in tandem with medication therapies, but articles were excluded if they were exclusively medication interventions. Let Evidence Guide Every New Decision (LEGEND) critical appraisals were completed on each of the included texts to determine evidence level and quality, in addition to Cochrane risk-of-bias assessment (Clark et al., 2009; Higgins et al., 2020; James M. Anderson Center for Health Systems Excellence, n.d.).
Results
Figure 1 includes the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. Both the original and updated searches yielded 8,082 total articles for title and abstract screening, after removal of 4,429 duplicates across all databases. Title and abstract screening resulted in 237 relevant articles for consideration for full-text screening, with 92.1% rater agreement (excellent agreement; Polanin et al., 2019). Exclusion criteria for full-text review were pilot tested on 10% of the eligible full-text review articles, with consensus reached on exclusion criteria with 91.2% rater agreement (excellent agreement; Polanin et al., 2019).
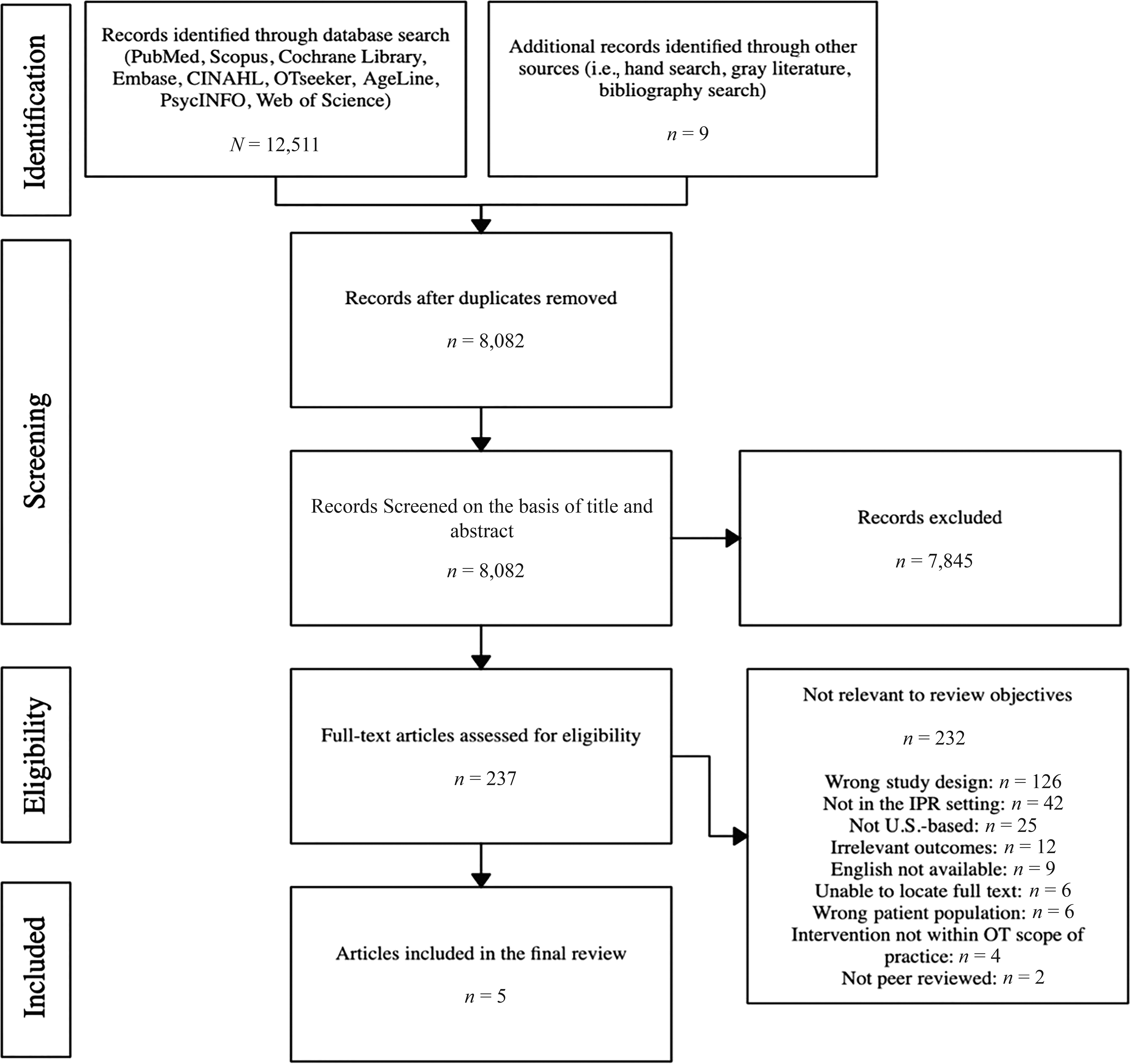
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
After full-text review, 5 articles were identified for inclusion. The article publication years for the included studies ranged from 1984 to 2009. Diagnostic populations included traumatic brain injury (n = 1), stroke (n = 1), rheumatoid arthritis (n = 1), general rehabilitation (gait disturbances, deconditioning, hip fracture repair; n = 1), and spinal cord injury and dysfunction (n = 1). Average reported LOS for nonmilitary participants was 18 days, and participants of the 5 studies were primarily middle-aged, non-Hispanic White men (approximately 80% of participants).
Study Design and Outcome Variables
Three of the studies used randomization, and only 1 study used a no-treatment control group. Four of the studies addressed depressive symptoms only (Davis, 2004; Duchnick et al., 2009; Lichtenberg et al., 1996; Parker et al., 1984). All of the studies had mental health outcomes as the primary outcome. One study assessed both depressive and anxiety symptoms (Vanderploeg et al., 2008). Regarding secondary outcomes of interest, all of the studies included measures of general health-related quality of life as an outcome measure in addition to impact of disability and functional independence. The evidence level of three of the studies was rated as Level 2b (lesser–quality randomized controlled trials) according to LEGEND critical appraisal. Occupational therapy practitioners were involved in the interventions for 3 of the studies (Lichtenberg et al., 1996; Parker et al., 1984; Vanderploeg et al., 2008). Nursing and psychology were involved in the remaining 2 studies (Davis, 2004; Duchnick et al., 2009).
Intervention Type
Treatment strategies used included life review therapy versus standard care control (Davis, 2004); coping effectiveness training versus supportive group therapy (Duchnick et al., 2009); cognitive–didactic therapy versus functional–experiential rehabilitation therapy (Vanderploeg et al., 2008); a three-arm behavioral treatment (positive events and relaxation training) delivered through rehabilitation psychology, versus behavioral treatment delivered through occupational therapy, versus no-treatment control (Lichtenberg et al., 1996); and a patient educational intervention versus standard care control (Parker et al., 1984). Table 2 summarizes the interventions used and supporting evidence for efficacy (specific to occupational therapy) for the included studies. Table A.1 in the Supplemental Appendix (available online with this article at https://research.aota.org/ajot) summarizes included articles and efficacy of the interventions, and Supplemental Appendix Table A.2 summarizes the risk of bias.
Overview of Interventions and Supporting Evidence
Note. AJOT = American Journal of Occupational Therapy; RCT = randomized controlled trial.
Intervention Intensity
The included articles demonstrated decreased depressive and anxiety symptoms with low-intensity interventions. Most interventions (n = 3) were administered for 60 min once per week. The total number of weeks of the interventions were not reported, due to fluctuations in participant LOS. Duchnick et al. (2009) demonstrated reduced depressive and state anxiety symptoms with weekly coping effectiveness training among patients with spinal cord injury and dysfunction. Life review therapy for stroke survivors was effective for reducing depressive symptoms and enhancing life satisfaction with three 60-min sessions weekly (Davis, 2004). In addition, Lichtenberg et al. (1996) demonstrated reduced depressive symptoms and increased functional recovery among geriatric patients receiving general musculoskeletal rehabilitation using two 30-min weekly treatment sessions. Vanderploeg et al. (2008) used the most time-intensive intervention, delivering 1.5 to 2.5 hr per day, 5 days per wk, of cognitive–didactic therapy or functional–experiential therapy. The educational intervention in the Parker et al. (1984) study involved a total of 7 hr of educational programs delivered over the course of the participants’ LOS.
Intervention Efficacy
The cognitive and behavioral strategies used in the studies were primarily efficacious for alleviating primary outcomes of adverse mental health symptoms (n = 4 had statistically significant reductions in depressive or anxiety symptoms). All but 1 of the included articles had statistically significant results for additional secondary outcomes, including life satisfaction (Davis, 2004), dexterity (Parker et al., 1984), independence in ADLs and return to work at follow-up (Lichtenberg et al., 1996; Vanderploeg et al., 2008), and cognitive recovery (Vanderploeg et al., 2008).
Discussion
In this systematic review, we sought to determine what interventions within the occupational therapy scope of practice address depressive and anxiety symptoms within IPR and the efficacy of these interventions. The results indicate that the majority of studies conducted in the IPR setting addressing depressive and anxiety symptoms were cognitive and behavioral interventions. Both cognitive and behavioral interventions are a common therapeutic framework for depressive and anxiety symptoms and have been used by occupational therapy practitioners largely for patients with primary mental health diagnoses (Berking et al., 2013; Gutman & Raphael-Greenfield, 2014). The interventions used in this review were primarily efficacious for both reducing depressive symptoms and enhancing quality of life and functional status. Adverse mental health symptoms were reduced with relatively low-intensity sessions. This finding may signal that efficacious interventions could be effectively incorporated into occupational therapy practice by requiring minimal disruption to routine care and service delivery (Lehane et al., 2019).
Only 1 study was rated as low risk for bias (Vanderploeg et al., 2008). This finding highlights the need for additional research investigating occupational therapy cognitive, behavioral, and cognitive–behavioral treatment strategies for depressive and anxiety symptoms in the IPR setting to conclusively determine efficacy. Factors indicating a high risk of bias were lack of blinding, reported fidelity measures, and intent-to-treat analyses. The high risk of bias among the studies does affect conclusions regarding the efficacy of the evidence and supports the need for further research to determine the efficacy of cognitive and behavioral interventions within the occupational therapy scope of practice among patient populations with physical disabilities. Moreover, the quality of the study designs in the included articles supporting occupational therapy was relatively low. Only 1 of the included studies used a no-treatment control group, and the findings were mostly concentrated in middle-aged, non-Hispanic White, male participants. Specifically, research that uses high-quality and rigorous methodologies among demographically and clinically diverse patient groups is warranted to determine the efficacy of cognitive and behavioral interventions within IPR. In addition, research is needed to examine strategies for supporting functional participation and quality of life through occupational engagement in this setting.
The results of this review indicate that the role of occupational therapy in supporting mental health within physically affected populations in the IPR setting has been minimally investigated. The most recent study included in this review was published in 2009, further warranting additional research investigating occupational therapy’s role in addressing depressive and anxiety symptoms in the IPR setting. This trend is consistent with a literature review by Gutman and Raphael-Greenfield (2014), which stated that mental health–related articles published in the American Journal of Occupational Therapy had been steadily declining. The findings of this review in light of the growing emphasis on the medical model and the prioritization of physical functional recovery among occupational therapy practitioners highlight the importance of maintaining mental health treatment perspectives in settings where such perspectives are often not traditionally adopted (Pizzi & Richards, 2017).
This lack of information may also reflect the impact of reported multilevel barriers to addressing depressive and anxiety symptoms in IPR patient populations among occupational therapy practitioners. Simpson et al. (2018) found that occupational therapy practitioners report both health care system and provider-level barriers to mental health care delivery among stroke survivors. Such barriers include increased productivity standards and pressure to emphasize physical recovery over mental recovery as well as a lack of professional development opportunities specific to the occupational therapy discipline (Graham et al., 2013). These previously identified barriers to addressing mental health among physically affected patients, including in the IPR setting, may correspond to the lack of available and current evidence from this systematic review. This lack of available evidence found in this review also validates the reported perceptions of occupational therapy providers because there is little literature to inform practice for addressing depressive and anxiety symptoms among physically affected populations in the IPR setting (Simpson et al., 2018).
The lack of consistent information and terminology for identifying and describing the IPR setting observed is troubling. The acuity of injury may affect the efficacy of commonly used cognitive-based interventions, particularly among patients with neurological injuries that may affect self-awareness and meta-analytic skills often required for cognitive-based treatments (Hofmann et al., 2012). In addition, as mentioned previously, the resources and structure of IPR settings differ from other settings and may also affect the feasibility of efficacious treatment delivery. The heterogeneity of terminology used to describe the IPR setting—including “acute rehabilitation,” “acute rehabilitation units,” “inpatients,” “inpatient rehabilitation,” “subacute rehabilitation,” and “postacute rehabilitation”—presents multiple problems not only for occupational therapy practitioners but also for other health care providers because it was noted that these terms are often used interchangeably between acute care and IPR levels of care.
The heterogeneity of terminology may also explain why so few articles ultimately met eligibility criteria (0.06%). Most articles were excluded on the basis of the criterion of not being conducted in the IPR setting. Often, the term “inpatient” was used interchangeably for “mental health institutionalization” and “acute care services.” This occurrence may have then resulted in a high number of these articles with this terminology being pulled into the initial search but ultimately not meeting the review criteria. The use of the term “inpatient rehabilitation” or “IPR” may be beneficial because it matches CMS language designating and accrediting IPR facilities in U.S. health systems.
The search surfaced non–U.S. based articles that otherwise met inclusion criteria (n = 25). However, many of these studies described the IPR experience as having a much longer duration than the U.S.-based studies (i.e., non–U.S. based studies described 6- or 8-wk courses of IPR). The differences in medical models and health services delivery may explain the greater availability of research in non–U.S. based studies because the longer LOS may facilitate greater time to comprehensively assess physical and mental health during IPR.
Moreover, because of the time- and cost-intensive nature of IPR facilities, shorter lengths of stay for patients are often pushed by administrative and health insurance officials (Dobrez et al., 2010; Forrest et al., 2019). Pressure to reduce LOS may limit the amount of time occupational therapy practitioners have to comprehensively assess and treat both physical and mental health, which may also contribute to limited research regarding depressive and anxiety interventions in IPR. However, pressure to reduce LOS should not mean compromising care through deprioritization of mental health care because the experience of depressive and anxiety symptoms during the IPR stay has negative long-term effects on quality of life and functional recovery and increases mortality (Cree et al., 2020; Graham et al., 2013).
Early assessment and rehabilitation are effective nonpharmacological strategies to prevent depressive and anxiety symptoms, and the occupational therapy profession in the IPR setting is uniquely qualified to facilitate physical and mental recovery to support participation in occupations. These strategies can positively influence health not only in the short term but also throughout the continuum of care by facilitating increased functional recovery and, thus, decreased future health care system utilization (Chandrasekar et al., 2019). Maintaining mental health treatment perspectives within physical disability settings could translate to increased research among inpatients with physical disability experiencing depressive or anxiety symptoms; in addition, it could highlight opportunities to explore the potentially mediating role that mental illness plays in affecting physical recovery after an illness or disability (Pizzi & Richards, 2017).
Limitations
This systematic review is not without its limitations. Articles may have been missed in the hand or gray literature search; however, the use of email alerts and completion of a second search of the literature to capture any articles published in that time frame mitigated these risks. The inconsistent terminology used in the literature may have affected the accuracy of the health care setting identification during determination of eligibility criteria. Moreover, the search terms may not have comprehensively identified relevant studies; however, a health sciences librarian was consulted to promote thoroughness of the search strategy. Because of the heterogeneity of the studies identified in the evidence, a meta-analysis could not be performed.
Future Directions
On the basis of the findings of this systematic review, future research should include the following directions: (1) expand research conducted on occupational therapy’s role in supporting mental health among populations with physical disabilities across the continuum of care, (2) increase research conducted specific to the IPR setting, and (3) use consistent and explicit terminology to describe settings to aid clinicians in the identification of relevant research.
Implications for Occupational Therapy Practice
The results of this systematic review have the following implications for occupational therapy practice: Limited, moderate-quality evidence exists to support occupational therapy practitioners in addressing mental health within the physical disability IPR setting. The 5 included studies support the use of cognitive and behavioral treatment strategies within the occupational therapy scope of practice among patients with depressive and anxiety symptoms in the physical disability IPR setting. The heterogeneity of terminology makes identification of evidence difficult, which may affect clinicians’ decisions to incorporate addressing mental health into practice. Given the pivotal time frame in the adjustment to disability and recovery stage that the IPR setting represents, additional research specific to this setting is warranted to support patient-centered mental health care in IPR.
Conclusion
Limited, moderate-quality evidence exists documenting occupational therapy practitioners’ role in addressing depressive and anxiety symptoms within the physical disability IPR setting. Further research in which high-quality, rigorous methodologies are used among demographically and clinically diverse patient groups is warranted. The IPR setting is an ideal care setting where occupational therapy can be used to address mental health in tandem with physical functional recovery while patients have access to a multidisciplinary team. Further research to investigate effective occupational therapy interventions for addressing depressive and anxiety symptoms and their impact on recovery is imperative to occupational therapy practitioners comprehensively supporting patient health and participation in meaningful occupations.
Supplemental Material
Supplementary material for Occupational Therapy Interventions to Address Depressive and Anxiety Symptoms in the Physical Disability Inpatient Rehabilitation Setting: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.049068.pdf for Occupational Therapy Interventions to Address Depressive and Anxiety Symptoms in the Physical Disability Inpatient Rehabilitation Setting: A Systematic Review by Janell Pisegna, Sarah Anderson and Jessica L. Krok-Schoen in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies included in the systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.