
Abstract
In the current policy context, the occupational therapy profession must act to promote and sustain high-value care. Stakeholders have delineated efforts, such as defining and measuring high-quality care processes or promoting the adoption of evidence into practice, that can enhance the value of occupational therapy services. There is a growing recognition, however, that low-value care is the product of deficiencies within health care systems and is therefore most amenable to system-level solutions. To date, the specific nature of system-level changes capable of identifying and rectifying low-value occupational therapy has yet to be elucidated. In this “The Issue Is. . .” column, we introduce occupational therapy to the Learning Health System concept and its essential functions. Moreover, we discuss action steps for occupational therapy stakeholders to lay the foundation for Learning Health Systems in their own professional contexts.
The authors introduce the Learning Health System (LHS) concept and provide action steps for occupational therapy stakeholders to lay the foundation for LHSs in their own professional contexts.
High-value occupational therapy services can be defined as the optimization of four outcomes (i.e., the Quadruple Aim): (1) enhanced patient experience, (2) enhanced practitioner experience, (3) improved population health, and (4) reduced cost (Bodenheimer & Sinsky, 2014). Compared with health care systems globally, the U.S. health care system delivers low-value care, expending more resources yet achieving worse patient outcomes (Davis et al., 2014). The Patient Protection and Affordable Care Act (Pub. L. 111-148) sought to reverse this trend by altering the incentive structure of the U.S. health care system to reward greater value, requiring that occupational therapy researchers and practitioners promote the value of occupational therapy services (Leland et al., 2015). Related to this, the American Occupational Therapy Association’s (AOTA’s) Vision 2025 includes the goal of achieving high-value services, or the delivery of evidence-based, patient-centered, and cost-effective care (AOTA, 2019). Thus, occupational therapy researchers, practitioners, and educators must organize their collective efforts toward optimizing the value of occupational therapy services across settings and patient populations.
Many in the occupational therapy profession have embraced the challenge of this contemporary context, offering proposals for how practitioners, researchers, and educators can bolster the value of occupational therapy services. For example, some researchers have proposed that the value of occupational therapy can be promoted by improving the adoption of evidence into routine care through an implementation research agenda (Juckett et al., 2019; Marr, 2017). Others have highlighted the importance of defining and measuring high-value occupational therapy care processes to inform efforts aimed at achieving the Quadruple Aim (Leland et al., 2015). These efforts are necessary, yet insufficient, for promoting and sustaining value-based occupational therapy. Recognition that low-value care is the product of deficiencies within health care systems is growing; therefore, the focus on optimizing system-level processes has increased (Friedman et al., 2015). However, the specific nature of system-level processes capable of identifying and rectifying low-value occupational therapy has yet to be elucidated. The Learning Health System (LHS) concept—the focus of this column—holds promise for ensuring the delivery of high-value occupational therapy.
Learning Health Systems
The National Academy of Medicine has asserted that LHSs represent the primary means of achieving high-value care, and it defined an LHS as a system within which “science, informatics, incentives, and culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the delivery process and new knowledge captured as an integral by-product of the delivery experience” (Institute of Medicine [IOM], 2013, p. ix). In this way, LHSs can enact the multifaceted system-level changes necessary for achieving high-value care, including innovative care delivery and performance evaluation (Menear et al., 2019).
LHSs emerge from systemic infrastructure (e.g., culture, strategic planning) that incentivizes perpetual quality improvement, in contrast to systems that implement solutions in response to crises or other external incentives (e.g., accreditation standards; Friedman et al., 2017; Kraft et al., 2017). For example, a shared culture of perpetual quality improvement became entrenched within an academic medical center after routinely providing incentives for high-quality care (Kraft et al., 2017). Incentives provided by the health care system included transparent reporting of patient satisfaction surveys, systemwide celebrations of high-quality care, and financial incentives for outstanding performance.
Perpetual Quality Improvement
Perpetual quality improvement is achieved through learning cycles, an essential function of LHSs characterized by three phases: (1) Data to Knowledge (D2K), (2) Knowledge to Performance (K2P), and (3) Performance to Data (P2D; Friedman et al., 2017; Figure 1).
Data to Knowledge
The D2K phase of the learning cycle involves transforming data generated by both internal (e.g., routine care) and external (e.g., published research) sources into a form that guides clinical decision making and quality improvement efforts (Guise et al., 2018; Menear et al., 2019). Critical to this phase of the learning cycle—and to the function of LHSs generally—is the formation of a learning community, a network of stakeholders (e.g., patients, caregivers, practitioners, system leaders) devoted to addressing a problem of interest (Friedman et al., 2017; Menear et al., 2019). Among the learning community’s most critical tasks is to establish consensus regarding a definition of value that is accepted by all stakeholders (Menear et al., 2019). This consensus definition can inform the selection and development of indicators that use available information to characterize high-value occupational therapy, thereby enabling efforts aimed at understanding whether the system is producing high-value services.
In turn, identifying low-value care enables the learning community to generate data-driven practice recommendations (Friedman et al., 2017). For example, a health care system may use electronic health record (EHR) data to describe contemporary care and assess whether certain patterns of utilization are linked to higher value occupational therapy, perhaps operationalized using patient-reported outcomes, experience measures, cost data, or some combination of these. Such an approach is illustrated by a mounting body of work that leverages occupational therapy clinical encounter data to identify beneficial outcomes and areas that need improvement (e.g., Mroz, 2018). The results of this phase, synthesized with published evidence or practice guidelines, may generate occupational therapy practice recommendations that reflect high-value care (Friedman et al., 2017; Guise et al., 2018).
Knowledge to Performance
The K2P phase involves implementing the knowledge generated through the D2K phase (i.e., practice recommendations) to improve service delivery and achieve high-value care (Friedman et al., 2017; Menear et al., 2019). Again, the learning community plays an integral role in designing initiatives that align the delivery of occupational therapy services with the practice recommendations identified in the D2K phase. Efforts at this stage of the learning cycle may be informed by implementation science, the study of methods designed to maximize the uptake of evidence-based practices into routine care (Eccles & Mittman, 2006). For example, stakeholders can offer crucial information regarding potential determinants (e.g., inefficient communication) of adopting practice recommendations into routine care within the LHS (Juckett et al., 2020). An understanding of these determinants can inform the selection of implementation strategies aimed at promoting the adoption of practice recommendations that the learning community considers to reflect high-value occupational therapy (Waltz et al., 2019). (See Juckett et al., 2019, for a detailed discussion of selecting implementation strategies and measuring implementation outcomes.)
Performance to Data
In the P2D phase, practice-based data are collected to document the outcome of the efforts designed and implemented in the K2P phase of the learning cycle (Friedman et al., 2017). This phase includes the development and maintenance of a data infrastructure (e.g., EHRs) capable of capturing changes in indicators of high-value care, including patient and practitioner experience, patient outcomes, and cost (Menear et al., 2019). Thus, data infrastructures must be designed to allow an accurate and comprehensive depiction of documented occupational therapy services (Leland et al., 2015). For example, the learning community can work with information technology (IT) experts and data scientists to design an EHR platform that embeds indicators of occupational performance and other relevant clinical factors (e.g., environmental determinants). Multidisciplinary collaboration can help ensure that the documentation platform captures information useful for developing quality measures that reflect the process of high-quality occupational therapy, as previously defined by stakeholders of the learning community (see Leland et al., 2015). Consistent with the continuous and iterative nature of LHSs, quality improvement efforts do not cease at the conclusion of the P2D phase. Rather, the D2K phase is reinitiated, and quality improvement efforts continue into perpetuity (Figure 1; Friedman et al., 2017).
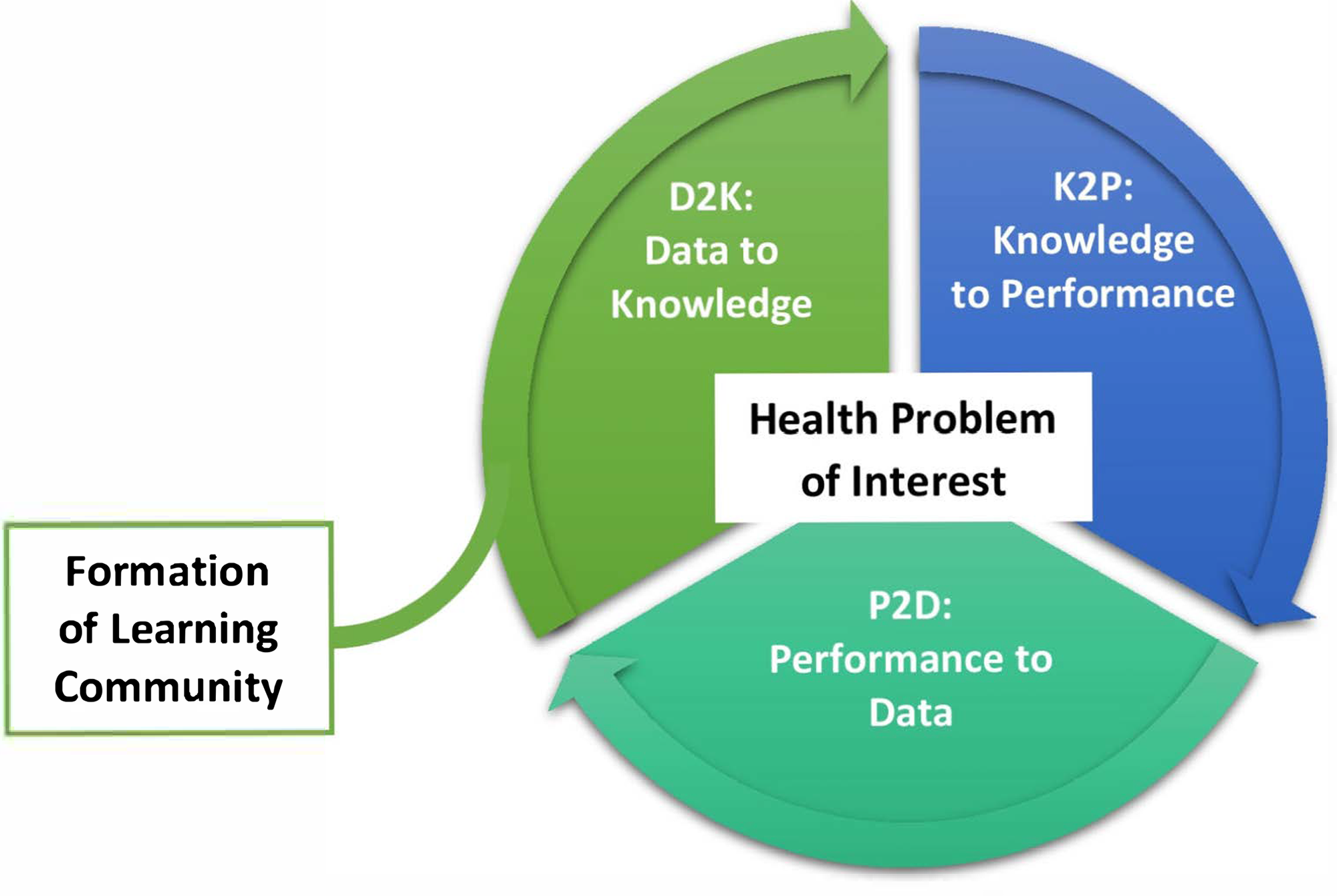
The learning cycle.
Note. From “Toward an Information Infrastructure for Global Health Improvement,” by C. P Friedman, J. C. Rubin, and K. J. Sullivan, 2017, Yearbook of Medical Informatics, 26, p. 18 (https://doi.org/10.15265/IY-2017-004). Copyright © 2017 by the authors. Adapted with permission under a CC-BY license.
Core Pillars: Laying the Foundation for Occupational Therapy Involvement in Learning Health Systems
The core pillars of LHSs form the infrastructure enabling learning cycles that promote and sustain high-value care. Using a rigorous process of literature review and expert stakeholder engagement, Menear et al. (2019) identified six core pillars that provide the foundation upon which value-creating LHSs are built: (1) scientific, (2) social, (3) technological, (4) policy, (5) legal, and (6) ethical. In the sections that follow, we define each pillar and describe its importance for supporting the essential functions of LHSs. In Table 1, we describe specific action steps the occupational therapy profession can take to bolster each respective pillar.
Learning Health System Pillars and Corresponding Action Steps for OT Stakeholders
Note. LeaRRn = Learning Health Systems Rehabilitation Research Network; LHS = Learning Health System; OT = occupational therapy. From “A Framework for Value-Creating Learning Health Systems,” by M. Menear, M.-A. Blanchette, O. Demers-Payette, and D. Roy, 2019, Health Research Policy and Systems, 17, p. 79 (https://doi.org/10.1186/s12961-019-0477-3). Copyright © 2019 by Springer Nature. Adapted with permission.
Scientific
This pillar refers to the “scientific infrastructure, programs, and resources that support knowledge generation, sharing and application” within the LHS (Menear et al., 2019, p. 4). We echo prior calls to build a critical group of health services researchers who are equipped with the skill set needed to improve the quality of occupational therapy (Leland et al., 2015) and rehabilitation services (Graham et al., 2018). To fully leverage the benefits of LHSs, the profession must develop scientific expertise and infrastructure unique to LHS research. Most important, efforts should enable occupational therapy researchers to embed themselves within health care systems, facilitating collaboration with stakeholders to create knowledge that is rapidly implemented to improve services while not disrupting clinical processes (Forrest et al., 2018). For example, efforts to bolster LHS research capacity in the profession (e.g., curricula development) could be informed by the LHS researcher competencies developed by Forrest et al. (2018).
Social
The social pillar represents the collaboration, or engagement, among stakeholders within the LHS and other related networks (Menear et al., 2019). As previously mentioned, an engaged learning community is essential for the successful function of an LHS, and the diversity of perspectives offered by different stakeholder groups (e.g., occupational therapy practitioners, patients, health care administrators) plays an integral role throughout the learning cycle (Friedman et al., 2017; Menear et al., 2019). However, potentially divergent perspectives across stakeholder groups, the complexity of health care systems, and the need to rapidly adopt quality improvement solutions pose significant challenges to stakeholder engagement within LHSs.
To overcome these challenges, occupational therapy and other stakeholders can develop a unique set of skills, such as communication and conflict resolution capabilities (Forrest et al., 2018). Moreover, system-level efforts that foster trusting relationships among diverse stakeholders can promote a culture of perpetual learning and improvement within occupational therapy settings (Kraft et al., 2017; Menear et al., 2019). For example, occupational therapy clinical leaders could form steering committees consisting of diverse stakeholders who help shape decisions regarding service delivery.
Technological
This pillar represents health technologies, devices, and IT infrastructure (Menear et al., 2019) that enable the LHS to “learn from every patient” by capturing information generated during daily clinical encounters (Friedman et al., 2015). A wide array of technological tools can enable occupational therapy delivery systems to engage in perpetual cycles of quality improvement, including clinical decision support systems, EHR platforms, and machine learning algorithms (see IOM, 2011, for a review). Input from occupational therapists and other stakeholders (e.g., patients) can help ensure such tools are feasible to implement and that they promote patient- and family-centered, evidence-based, and cost-effective care (Leland et al., 2015). For example, stakeholders could collaboratively develop tools embedded within the EHR (e.g., decision aids) that enable practitioners, patients, and their families to arrive at shared decisions regarding occupational therapy goals, treatments, and reevaluations (Agoritsas et al., 2015; Kuo et al., 2018).
Policy
The policy pillar refers to the rules, financing structures, and accountability measures within the LHS that incentivize routinized quality improvement efforts (Menear et al., 2019). To enable the successful operation of LHSs, occupational therapy leadership (e.g., rehabilitation supervisors) must enact policies that create conditions under which the various components of highly complex health care systems are mobilized toward strategic objectives (i.e., producing high-value occupational therapy; Forrest et al., 2018; Menear et al., 2019). Put more specifically, such conditions must incentivize a state of perpetual quality improvement within the system, thereby promoting and sustaining high-value occupational therapy. For example, a health care system may create a quality-improvement department to coordinate, promote, and sustain efforts that financially incentivize high-value occupational therapy service delivery (Kraft et al., 2017).
Legal
The legal pillar represents the laws and regulations that enable or restrict the operations of LHSs (Menear et al., 2019). For example, the Health Insurance Portability and Accountability Act of 1996 (Pub. L. 104-191) protects patient health data and shapes how information is exchanged among LHS stakeholders (U.S. Department of Health and Human Services, 2018), thus determining what can be used for quality-improvement efforts (Menear et al., 2019). Legislation and regulations that govern occupational therapy service delivery (e.g., reimbursement) also influence the LHS by encouraging particular patterns of care (Menear et al., 2019). Occupational therapy stakeholders must advocate for laws and regulations that enable, rather than constrain, the essential functions of LHSs within their practice communities. For example, occupational therapists have played an important role in efforts made by the Centers for Medicare & Medicaid Services aimed at developing quality metrics that assess the process of home- and community-based service delivery (Mallinson et al., 2018).
Ethical
Finally, the ethical pillar reflects the ethical structures and guidelines governing the processes of the LHS (Menear et al., 2019). Within LHSs, the distinctions among clinical practice, research, and quality-improvement efforts can be unclear, and the effective governance of such efforts requires a full understanding of unique and shared ethical issues (Finkelstein et al., 2015; Forrest et al., 2018). Clear ethical guidelines could ensure that access to data, generated by occupational therapy encounters, satisfies research and quality improvement efforts while also maintaining patient privacy (Menear et al., 2019). Other ethical considerations unique to LHSs include assigning patients who are receiving occupational therapy in real-world settings to treatment conditions in research protocols (Forrest et al., 2018). Occupational therapy clinical leaders, for example, could bolster this pillar by adopting an ethics framework designed to govern LHS processes (Faden et al., 2013).
Conclusion
The occupational therapy profession must act to promote and sustain high-value care, the achievement of which is most amenable to system-level solutions. Aligning health care systems with the essential functions of LHSs holds promise for optimizing high-value occupational therapy. By incorporating the provided action steps we have outlined, the profession can foster LHSs across practice contexts, thereby achieving the Quadruple Aim and the profession’s Vision 2025.
Footnotes
Acknowledgments
This work was not supported by the Veterans Health Administration, and the views expressed in this column are those of the authors and do not necessarily reflect the official policy or position of the Department of Defense, Department of Veterans Affairs, or the U.S. government. We thank Menear et al. (2019) for providing permission to adapt their table, originally published by Springer Nature and distributed under the terms of the Creative Commons Attribution 4.0 International License (![]() ).
).