
Abstract
A retrospective study found no associations between acute self-care status, social support, or housing situation and 30-day readmission when all HRRP diagnoses were examined together; higher levels of independence with self-care were significantly associated with reduced odds of readmission for patients with pneumonia.
Hospital readmissions are associated with poor patient health outcomes and high costs, and they are used as an important metric to evaluate the quality of care provided (Boozary et al., 2015; Jencks et al., 2009). The Centers for Medicare and Medicaid Services (CMS) initiated the Hospital Readmissions Reduction Program (HRRP) to reduce unplanned 30-day readmissions for Medicare patients (CMS, 2021). HRRP penalizes hospitals up to 3% of reimbursement if they have excessive 30-day readmissions compared with national averages for Medicare patients with one of the following diagnoses: acute myocardial infarction (AMI), heart failure (HF), pneumonia (PN), coronary artery bypass graft (CABG), chronic obstructive pulmonary disease (COPD), and total hip arthroplasty (THA) or total knee arthroplasty (TKA). To avoid HRRP penalties and improve patient health outcomes, hospital administrators and health care professionals are focusing enormous efforts on reducing readmissions. Occupational therapy has the potential to substantially reduce unplanned readmissions; however, the profession’s role has yet to be clearly defined.
Two areas in which occupational therapy could reduce readmission risk are optimization of independence with self-care during hospitalization and identification and integration of social factors into discharge planning. Occupational therapy is one of only a few professions that simultaneously consider both clinical and social factors when creating a plan of care and discharge recommendations (American Occupational Therapy Association [AOTA], 2020). Both lower levels of independence with self-care in postacute settings and social factors have been linked with readmission risk (Calvillo-King et al., 2013; Greysen et al., 2015; Middleton, Downer, et al., 2018; Middleton, Graham, & Ottenbacher, 2018). To the best of our knowledge, researchers have not examined acute self-care status and readmission using documentation from the acute care setting. This lack of research has resulted in limited guidelines on how occupational therapy could contribute to reducing readmissions. Patients at higher risk for hospital readmission need to be identified in the acute care setting, and interventions need to be implemented accordingly to prevent readmission.
In recent years, there has been debate about whether social factors should be included in risk-adjustment methodology for HRRP (Bernheim et al., 2016; Joynt Maddox et al., 2019). Social factors such as poverty, disability, housing instability, lack of social support, and residence in a disadvantaged neighborhood have been linked to poor patient health outcomes and warrant consideration when evaluating methods for reducing readmissions (Calvillo-King et al., 2013; Joynt Maddox et al., 2019; National Academies of Sciences, Engineering, and Medicine, 2016). The link between social factors and patient health outcomes is complex. Further exploration of how social factors can be proactively addressed to reduce readmissions within the context of occupational therapy care delivery is needed.
The objective of this study was to examine whether acute self-care status and social factors are associated with 30-day, all-cause readmission for Medicare patients included in HRRP. It was hypothesized that patients who required no physical assistance with self-care tasks and who did not live alone would have lower odds of hospital readmission.
Method
Design and Data
This study used a retrospective, cross-sectional design with secondary data from a large acute care hospital in southeastern Wisconsin. All data were collected from the hospital’s electronic medical records (EMRs). The sampling time frame was January 2014 to February 2020. The study was approved by the institutional review board at the Medical College of Wisconsin and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental Appendix Table A.1, available online with this article at https://research.aota.org/ajot).
Participant Characteristics by Readmission Status
Note. ICU = intensive care unit.
Of the 17,618 patients included in the analytical sample, 17,518 patients (2,312 readmitted and 15,206 not readmitted) had race and ethnicity documented in their electronic medical records.
Participants
The study sample included Medicare patients admitted to the study site between 2014 and 2020 with an HRRP-qualifying diagnosis: AMI, HF, PN, CABG, COPD, or THA or TKA. Participants were identified in the EMR by International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD–10; World Health Organization, 2019) codes. All patients admitted to the study site during the sampling time frame with Medicare as the primary payor for their hospital stay were included in the study regardless of age. Patients were excluded from the sample on the basis of the following criteria: left the hospital against medical advice, transferred to another acute care hospital, died during the index hospitalization, discharged to hospice, or died within 30 days after discharge from the hospital. Excluding these patients from the sample helped to ensure that only the standard of care was provided during hospitalization and that readmissions were indicators of the quality of care provided and not the result of unavoidable circumstances (Kumar et al., 2019; Figure 1).
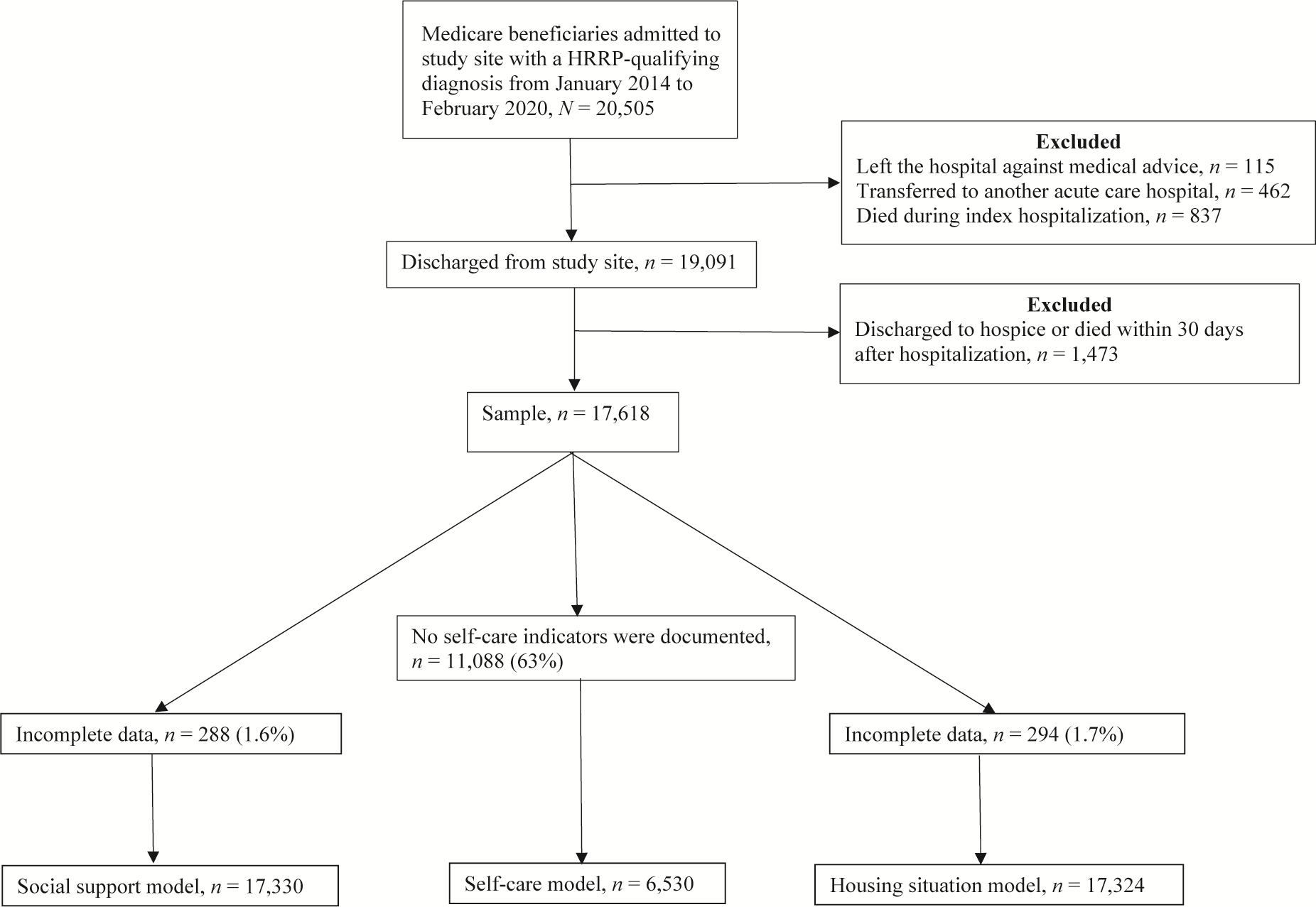
Cohort selection.
Key Variables
The key variables were acute self-care status and two social factors: social support and housing situation. Self-care is a domain composed of multiple indicators and can vary depending on the setting. The self-care indicators used at the study site, an acute care hospital, were eating, grooming, shower or bathe self, upper body dressing, lower body dressing, and toileting hygiene. Unlike postacute settings, no universal patient assessment instrument in the acute care setting defines relevant self-care indicators. Moreover, no national regulating organizations mandate acute care occupational therapy practitioners to provide documentation on any specific self-care indicators, which results in large amounts of missing data and practice discrepancies.
In anticipation of a considerable amount of missing data, a composite variable was created for the self-care variable. Patients were included if self-care indicators were documented at any point during their hospital stay. If a patient required physical assistance for any of the self-care indicators, the variable was scored as 1; if none of the self-care indicators reflected that the patient required physical assistance, the variable was scored as 0. Physical assistance and no physical assistance were defined by the levels of independence available in the documentation. Physical assistance included the following levels of independence: dependent, maximum assistance, moderate assistance, minimal assistance, and contact guard assistance. No physical assistance included the following levels of independence: supervision, conditional independence (i.e., modified independence), and independent. Using this composite scoring method, we could include a patient’s record in the analysis even if they had documentation of only one self-care indicator.
Quantification of social factors is also challenging in the acute care setting secondary to minimal documentation requirements. Two social factors within the scope of occupational therapy practice were collected for this study: (1) social support and (2) prehospitalization housing situation (hereinafter, housing situation). Collection of the data for social support and housing situation at the study site was done as soon after admission as clinically appropriate. The social support variable captured who was reported to live with the patient. Documentation options for social support were alone, child(ren)–adult, child(ren)–dependent, facility resident, friends, grandchildren, grandparents, other relatives, parents, siblings, significant other, and spouse. The options were consolidated into two categories to create a dichotomous variable: alone or not alone.
The housing situation variable captured where the patient was reported to be living before hospitalization. The following housing situation documentation options were included: home, apartment, or condo; correctional facility; extended care facility; foster care; group home; homeless; hotel or motel; independent or assisted living facility; residential facility; and shelter. The housing situation options were consolidated into categories to create a categorical variable. Transitional housing included foster care; correctional facility; homeless; and hotel, motel, or shelter. Supportive housing included extended care facility and group home. Independent housing included home, apartment, or condo. Finally, other included residential facility and independent or assisted living facility. Because of sample size limitations in the subgroup analyses, the housing situation variable was collapsed into a dichotomous variable: independent housing or other.
Covariates
The following covariates were included in the statistical analyses: age, sex, race, postacute discharge location, comorbidities, and intensive care unit (ICU) stay (Horney et al., 2017; McIntyre et al., 2016; Pedersen et al., 2017; Silverstein et al., 2008). Age was entered as a continuous variable, whereas sex was a dichotomous variable including male or female. White or Caucasian, Black or African-American, or other were the categories used to classify race and ethnicity. Postacute discharge location was entered as a categorical variable with the following options: home health care and self-care, nursing facility, or other. We calculated the number of comorbidities with the Elixhauser comorbidity measure using ICD–10 codes (Quan et al., 2005). The measure has demonstrated good predictive validity after translation from the International Classification of Diseases, Ninth Revision, Clinical Modification (Centers for Disease Control and Prevention, 2001) codes to ICD–10 codes for in-hospital and 30-days posthospitalization mortality (Menendez et al., 2014; Sharabiani et al., 2012). The comorbidity variable was a continuous variable. The ICU stay variable was dichotomized into yes or no.
Outcome
The primary outcome measure used in this study was 30-day, unplanned hospital readmissions. This measure included any unplanned readmission that occurred within 30 days of discharge from the hospital. Verification that all the readmissions included in the study met CMS criteria was done by an external company, Vizient (Irving, TX).
Statistical Analyses
Descriptive analyses were performed for the total sample, then stratified by readmitted and not readmitted. Three models were estimated to examine the association among (1) self-care status and 30-day readmission (self-care model), (2) social support and 30-day readmission (social support model), and (3) housing situation and 30-day readmission (housing situation model) using the sample with all the HRRP diagnoses. Unadjusted and adjusted results were calculated for the three models. The adjusted models controlled for age, sex, race, postacute discharge location, comorbidities, and ICU stay. Estimations of the three models were done for the following subgroups: AMI, HF, PN, COPD, CABG, and THA or TKA (i.e., the individual HRRP diagnoses). If the unadjusted models for the subgroups were significant, then adjusted models were estimated controlling for age, sex, race, postacute discharge location, comorbidities, and ICU stay. Last, the interaction between (1) social support and self-care and (2) housing situation and self-care for each diagnosis was evaluated. We performed statistical analyses using R (Version 4.0.0; R Project for Statistical Computing, Vienna, Austria).
Results
After the application of the inclusion and exclusion criteria, the sample included 17,618 older adults hospitalized for an HRRP-qualifying diagnosis over the study period. Incomplete data for the social support model (1.6%) and housing situation model (1.7%) were minimal (see Figure 1). However, only 37% of the sample had self-care indicators documented (see Figure 1). The overall readmission rate was 13%. Most of the patients discharged to home (74.1%). When comparing patients who were readmitted with patients who were not readmitted, patients who were readmitted were younger, were more likely to be Black or African-American, were more likely to have discharged to a nursing facility, had higher comorbidity counts, and were more likely to have had a stay in the ICU while hospitalized (Table 1). No difference was found in readmission rates by sex (see Table 1).
For the self-care model, social support model, and housing situation model that included all the HRRP diagnoses, only the category of supportive housing in the unadjusted housing situation model was found to significantly increase the odds of readmission for Medicare patients (odds ratio [OR] = 1.22, 95% confidence interval [CI] [1.05, 1.41]). In the adjusted self-care model, social support model, and housing situation model, no associations were found between self-care status and readmissions, social support and readmissions, and housing situation and readmissions (Table 2). Therefore, the odds that patients with HRRP-qualifying diagnoses were readmitted within 30 days were not increased or decreased on the basis of their level of independence with self-care tasks while hospitalized; whether they lived alone (i.e., social support); or whether their housing situation was transitional, supportive, independent, or other. Moreover, no significant interactions were found between social support and self-care or between housing situation and self-care for any of the HRRP diagnoses. As a result, we did not stratify the analyses.
Models (Unadjusted and Adjusted) Estimating the Association Between Self-Care Status and Readmission, Social Support and Readmission, and Housing Situation and Readmission
Note. CI = confidence interval; ICU = intensive care unit; OR = odds ratio; ref. = reference category.
p < .05.
p < .01.
In the subgroup analyses, the association between self-care status and readmission was significant when limited to the PN subgroup. Patients with PN were found to have lower odds of readmission when they had higher levels of independence with self-care in both the unadjusted (OR = 0.64, 95% CI [0.48, 0.85]) and adjusted (OR = 0.59, 95% CI [0.43, 0.80]; Table 3) models. None of the other subgroup models that estimated the association between self-care status and readmission were significant. Last, the subgroup models that estimated the association between social support and readmission and housing situation and readmission for the individual HRRP diagnoses were not significant.
Subgroup Analyses for Each HRRP Diagnosis (Adjusted for PN Group Only)
Note. AMI = acute myocardial infarction; CABG = coronary artery bypass graft; CI = confidence interval; COPD = chronic obstructive pulmonary disease; HF = heart failure; HRRP = Hospital Readmissions Reduction Program; ICU = intensive care unit; OR = odds ratio; PN = pneumonia; ref. = reference category; THA = total hip arthroplasty; TKA = total knee arthroplasty.
Unadjusted.
Adjusted.
p < .05.
p < .01.
The following patient characteristics were all significantly associated with readmission risk in all three models (i.e., self-care, social support, and housing situation) that included all the HRRP diagnoses: age, comorbidity count, and ICU stay while hospitalized (see Table 2). For the PN subgroup, age, discharge to a location other than home (excluding nursing facility), and comorbidity count were significantly associated with readmission (see Table 3).
Discussion
In accordance with the stated goals and policies of CMS, reduction of hospital readmissions has been identified as a quality improvement priority. The holistic practice approach of occupational therapy uniquely situates the profession to reduce readmission rates by incorporating both clinical and social factors in patient care and discharge planning. To leverage this opportunity, a nuanced understanding of how these clinical and social factors affect risk of readmission is needed. In this study of more than 17,000 Medicare inpatients with an HRRP-qualifying diagnosis, no associations were found between self-care status and readmissions, social support and readmissions, and housing situation and readmissions in analyses that included all HRRP-qualifying diagnoses. In subgroup analyses, we found that higher levels of independence with self-care were associated with reduced odds of readmission for patients with PN.
Impaired functional status, specifically related to self-care tasks, has consistently been found to be associated with higher likelihood of readmission in postacute settings (Greysen et al., 2015; Middleton, Downer, et al., 2018; Middleton, Graham, & Ottenbacher, 2018). In the acute care setting, Freburger et al. (2020) evaluated the relationship between acute occupational therapy and physical therapy utilization and risk of 30-day readmission or death for patients with PN. More utilization of acute occupational therapy and physical therapy services reduced the risk of readmission and death for patients with PN. Freburger et al. proposed that because occupational therapy and physical therapy minimize functional decline while hospitalized, patients who receive these services are less likely to be readmitted.
Our findings support the relationship between self-care and readmission risk for patients with PN in the acute care setting; however, we were unable to find an association between self-care and readmission for the other HRRP diagnoses (AMI, HF, COPD, CABG, and TKA or THA). Our study was limited by missing data for self-care status, owing to the absence of documentation requirements for this variable. Moreover, the lack of a standardized measure to evaluate independence with self-care in the acute care setting introduces variability related to differences in clinical judgment among occupational therapy practitioners. The most complete understanding of the relationship between acute self-care status and readmission would be provided by a widely used comprehensive and standardized measure of self-care status in the acute setting.
We found no association between social support and readmission. These results are specific to the definition of social support used in this study: whether the patient lived alone. The variable definition did not include data on the willingness or ability of any people who lived with the patient to assist the patient in postdischarge care or on the patient’s perceived level of support. Chan et al. (2019) determined that minorities who report a high level of perceived social support have reduced risk of readmission. Quality of social support, as opposed to the mere presence or absence of support, may have the greatest impact on patient outcomes. Future work should incorporate data on the quality of support.
Housing situation was also not found to be significantly associated with readmission. To the best of our knowledge, our study is the first to explore housing situation as a social factor related to readmission risk. This variable is similar to housing instability, which is defined as the number of address changes in the past year. Housing situation was used because it is a common topic discussed between occupational therapy practitioners and patients while hospitalized. Housing instability has been found to be a significant predictor of readmission in previous studies; however, housing situation was not associated with risk for readmission in our sample (Calvillo-King et al., 2013).
The primary intent of this study was to examine the impact of self-care status and social factors within the scope of occupational therapy practice on readmission. For years, it has been proposed that occupational therapy is a profession with the training needed to reduce hospital readmissions (Roberts & Robinson, 2014; Roberts et al., 2020; Rogers et al., 2017). However, in the acute care setting, direct evidence that supports the role of occupational therapy in improving patient outcomes such as readmission is limited. In our study, higher levels of independence reduced the odds of readmission only for patients with PN. However, our findings may have been affected by the lack of a standardized self-care measure in the acute setting, the complexity associated with defining and collecting information on social support and housing situation, and missing data.
Although it is important for occupational therapy practitioners to use their clinical judgment during sessions with patients, it is debatable whether the same lack of standardization should be applied to documentation (AOTA, 2020; Zanca & Dijkers, 2014). Without clear and consistent documentation among acute care occupational therapy practitioners, not only within the same facility but across all facilities nationally, researchers are limited in accurately evaluating occupational therapy’s impact on quality outcomes in the acute care setting. This limitation may threaten the inclusion of occupational therapy as a needed profession when considering how best to improve patient outcomes. Acute care occupational therapy departments should consider national implementation of a set of standardized measures to determine independence level with self-care tasks.
Study Limitations
The sample we used for our study was from a single hospital, which may have reduced the generalizability of our findings. Moreover, only within-system readmissions were captured for this study. Several limitations resulted from using EMRs as the data source for this study, including potential data-entry issues, missing data, and a lack of a standardized format for collecting the information. Missing data were a significant issue for the self-care variable, with missing data present in 9.4% to 66.1% of cases (Supplemental Appendix Table A.2). As a result, our results may not be generalizable to the entire HRRP population.
Additionally, data were not available on patients’ baseline function before hospitalization, which may have affected the self-care status outcome. More thorough documentation of baseline function and self-care status is needed for future research. The occupational therapy practitioners at the study site received no formal training on how to document levels of independence for self-care tasks related to this study, which may have confounded results. Last, the data source for this study did not include a measure of cognition. Impaired cognitive status is known to be a factor associated with readmissions (Middleton, Downer, et al., 2018; Middleton, Graham, & Ottenbacher, 2018). In future studies, researchers should consider alternative methods that would allow inclusion of cognitive status in the analyses.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice: Acute care occupational therapy practitioners should consider adopting a standardized measure of self-care status that can be implemented in hospitals nationwide. Inclusion of quality of social support should be included in the acute care occupational profile.
Conclusion
Self-care status was significantly associated with lower odds of readmission only for patients with PN. Self-care status, social support, and housing situation were not significantly associated with readmission for any of the other HRRP diagnoses. The findings may reflect the inadequacies of acute occupational therapy documentation. Acute rehabilitation departments may want to consider creating guidelines on documentation of self-care tasks to ensure consistent and complete documentation. In future studies, researchers should consider using a standardized measure for self-care status that provides a comprehensive report on all self-care tasks.
Supplemental Material
Supplementary material for Impact of Acute Self-Care Indicators and Social Factors on Medicare Inpatient Readmission Risk
Supplementary material, sj-docx-1-aot-10.5014_ajot.2022.049084.docx for Impact of Acute Self-Care Indicators and Social Factors on Medicare Inpatient Readmission Risk by Jessica Edelstein, Addie Middleton, Rebekah Walker, Timothy Reistetter and Stacey Reynolds in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This article was written as part of the requirements for Jessica Edelstein to obtain her doctoral degree at Virginia Commonwealth University. We thank Sneha Nagavally (Medical College of Wisconsin) for her assistance with creating the analytical data set and statistical support for this project as part of her regular employment. We also thank Erin DeJarlais for her expertise in navigating the Froedtert Hospital system while conducting this research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.