
Abstract
This systematic review supports occupational therapy practitioners addressing PA and medication health management and maintenance IADLs through the use of coaching interventions when treating people with MS.
Multiple sclerosis (MS) is a progressive, immune-mediated condition that causes delays or stoppage of nerve signals in the central nervous system, resulting in widely varying symptoms and functional impact. It is estimated that almost 1 million Americans are living with MS, with 2.8 times higher prevalence among women (Wallin et al., 2019) and most people diagnosed between ages 20 and 50 yr (Walton et al., 2020). Common symptoms of MS can include fatigue, spasticity, weakness, changes in cognition, pelvic floor problems, and emotional changes. The resulting functional changes can vary greatly, including decreased physical activity (PA), forgetting medications, difficulty preparing meals, or problems driving.
Occupational therapy practitioners help people engage in the things that they need and want to do through the use of occupations, or meaningful daily activities (American Occupational Therapy Association [AOTA], 2020). Occupational therapy practitioners can provide a variety of physical rehabilitative, mental health, health promotion, and preventive interventions to promote functional engagement in everyday life. Examples of occupational therapy goals for a person with MS could include increasing driving skills, identifying supports for medication compliance, or establishing a PA routine to improve conditioning.
The last systematic review of the effectiveness of interventions within the scope of occupational therapy practice for people with MS was conducted by Yu and Mathiowetz (2014a, 2014b). They reported the need for better understanding of the length of benefit from occupational therapy–related interventions, unique contributions of occupational therapy practitioners to multidisciplinary teams, need for occupational therapy practitioners to play a role in developing health promotion interventions, and need for more research on the efficacy of occupational therapy interventions on level of impairment. Since then, no other systematic review has sought to update the evidence about occupational therapy–related interventions for people with MS, despite the rapidly changing landscape of MS research and prevalence estimates.
Because occupational therapy practitioners rely on high-quality evidence to inform their clinical practice and research, in this systematic review we sought to update and build on the previous literature by addressing the following question: “What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve and maintain performance and participation in instrumental activities of daily living (IADLs) among adults with MS?” This review was one of four systematic reviews conducted at the same time. The other three reviews asked the same question, with different focuses on activities of daily living (ADLs), rest, and sleep (Foidel et al., 2021; Yu et al., 2021); education, work, volunteering, leisure, and social participation (Nastasi & Harris, 2021); and caregivers (Preissner & Plow, 2021).
Method
This systematic review followed the Cochrane Collaboration methodology (Higgins et al., 2019) and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting a systematic review (Moher et al., 2010). This review provides a narrative synthesis of current evidence within the parameters of our project.
Search Strategy
The search terms were created on the basis of input from an advisory group of clinical and quality improvement content experts, input from a medical librarian, and a review of the current available literature. An example of the search strategy can be found in Table 1. The search was conducted by a medical librarian. Medical subject headings and text words were used and adapted as needed on the basis of each database. Databases searched were CINAHL, MEDLINE in PubMed, Cochrane, OTseeker, and PsycINFO.
Search Strategy
Eligibility Criteria
Types of Studies
Peer-reviewed journal articles published from January 2011 to December 2018 in English were included. The previous review of evidence by Yu and Mathiowetz (2014a, 2014b) covered articles from 2003 to May 2011, so this systematic review seeks to cover new evidence. Articles were excluded if they were published before January 2011 or after December 2018; were published in a non-English language; or were dissertations, theses, presentations, or conference proceedings. Levels of evidence were assigned according to the Oxford Centre for Evidence-Based Medicine (2009) in the following way: Level 1b: well-designed, appropriately powered, individual randomized controlled trial (RCT) Level 2b: individual prospective cohort study; small, lower quality RCT (e.g., <30 participants per group or pilot/feasibility studies); ecological studies; and two-group, nonrandomized studies.
In this systematic review, Level 1b and 2b studies were included because of the number of studies available. Level 3 studies were included only when no Level 1b or 2b studies were obtained for a particular theme. Systematic reviews that included our population of interest and some kind of IADL outcome were included in the search findings. These reviews were evaluated for our full review parameters, and none met them. Those reviews were then deconstructed, and the individual articles were hand searched and assessed for this systematic review’s specific inclusion criteria.
Participants
The population included adults age 18 yr and older with a diagnosis of MS. Articles were excluded if the average age of participants was <18 yr.
Interventions
Interventions were included if they were within the scope of occupational therapy services (did not require additional licensure or educational degree) and defined by the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; OTPF–3; AOTA, 2014), which was the current practice framework when the searches were conducted. Types of occupational therapy interventions included occupations and activities, preparatory methods and tasks, education and training, advocacy, and group interventions. Interventions outside the scope of occupational therapy practice were excluded.
Outcomes
Any outcomes that directly measured participation in and performance of IADLs, as outlined by the OTPF–3 (AOTA, 2014), were included. Outcomes were excluded if they measured client factors, performance skills, symptoms, or other measures that may affect participation and performance but did not measure participation and performance directly. If a study used an assessment that measured IADL participation or performance via subscales or specific items but did not include these subscales or items as part of the results, then that outcome was excluded.
Additional Inclusion Criteria Decision: Health Management and Maintenance IADLs
During the full article review stage, the authors found the literature supporting exercise and PA for people with MS to be vast. However, much of the literature focused on components of PA but not on PA occupations. The authors determined that additional inclusion criteria were necessary to ensure accuracy of the systematic review in assessing occupation, not rote components of PA, and reassessed all previously assessed articles with these new criteria.
The OTPF–3 (AOTA, 2014) defines health management and maintenance IADLs as “developing, managing, and maintaining routines for health and wellness promotion, such as physical fitness, nutrition, decreased health risk behaviors, and medication routines” (p. S19). It further defines routines as “patterns of behavior that are observable, regular, and repetitive and that provide structure for daily life” (p. S27). On the basis of these definitions, the authors determined outcomes needed to promote PA routines in some way, including carryover from clinic to home, measuring outside of structured time with an interventionist, or problem solving with an interventionist to embed exercise or PA into daily life.
Study Selection
Literature search results were collected, exact duplicates were removed, and the results were exported into EndNote format (Clarivate Analytics, Philadelphia, PA) by the medical librarian working on the project. The methodologist for the project reviewed all study titles, eliminating articles that were clearly outside of the review parameters (e.g., did not study MS, not research, not in the date range), and then forwarded the remaining results to the review authors.
The authors exported all citations from EndNote into a citation tracking table that tracked whether each study did or did not meet the inclusion criteria for the abstract/title review and full-text review. The authors used this table to make notes and to easily categorize the citations. The authors independently screened abstracts and titles yielded by the search, then compared their decisions to include or exclude. Differences were resolved by discussion with both authors. For 4 studies, the authors requested feedback from a third party until consensus was reached. The full texts of the remaining articles were assessed for inclusion following the same procedure, with 2 studies requiring third-party consultation and consensus.
Study Quality
Final articles that met the inclusion criteria were evaluated for risk of bias and strength of evidence, then abstracted into an evidence table (Table A.1 in the Appendix). Each author independently evaluated and extracted data for each study, then the evaluations and data were compared, and edits were completed after discussion. A master citation table was created for the final studies and was reviewed, along with the evidence table and the risk-of-bias table (Table A.2), for quality control by AOTA staff and the research methodologist.
Strength of Evidence (Level of Certainty)
Note. OT = occupational therapy. The strength of evidence is based on the U.S. Preventive Services (2018) guidelines.
Levels of Evidence
Level 1b and 2b studies were included (Oxford Centre for Evidence-Based Medicine, 2009). Level 3 studies were included only when no Level 1b or 2b studies were obtained for a particular theme.
Risk of Bias
Risk of bias was evaluated depending on the study design. Because all of the articles in this systematic review had a control group, the Cochrane tool was used to assess risk of bias (Higgins et al., 2016).
Overall Strength of Evidence
Results were narratively synthesized into thematic groups on the basis of which IADLs were measured. To determine the level of certainty about the net benefit of these interventions, the authors analyzed themes for strength of evidence according to the U.S. Preventive Services Task Force (2018) ratings using a formula based on the number of studies, level of evidence, risk of bias, and significance of the findings for each theme or subtheme. Table 2 describes each strength of evidence level.
Results
Final Studies
After the initial review by the librarian and research methodologist, the authors reviewed 610 articles. These articles were screened for inclusion, which resulted in 519 records excluded. Full-text review was completed for 91 articles, resulting in 20 studies included in the final review. The PRISMA flow diagram is presented in Figure 1. The final articles were grouped into themes and subthemes on the basis of IADL outcomes and related interventions (see Table A.1).
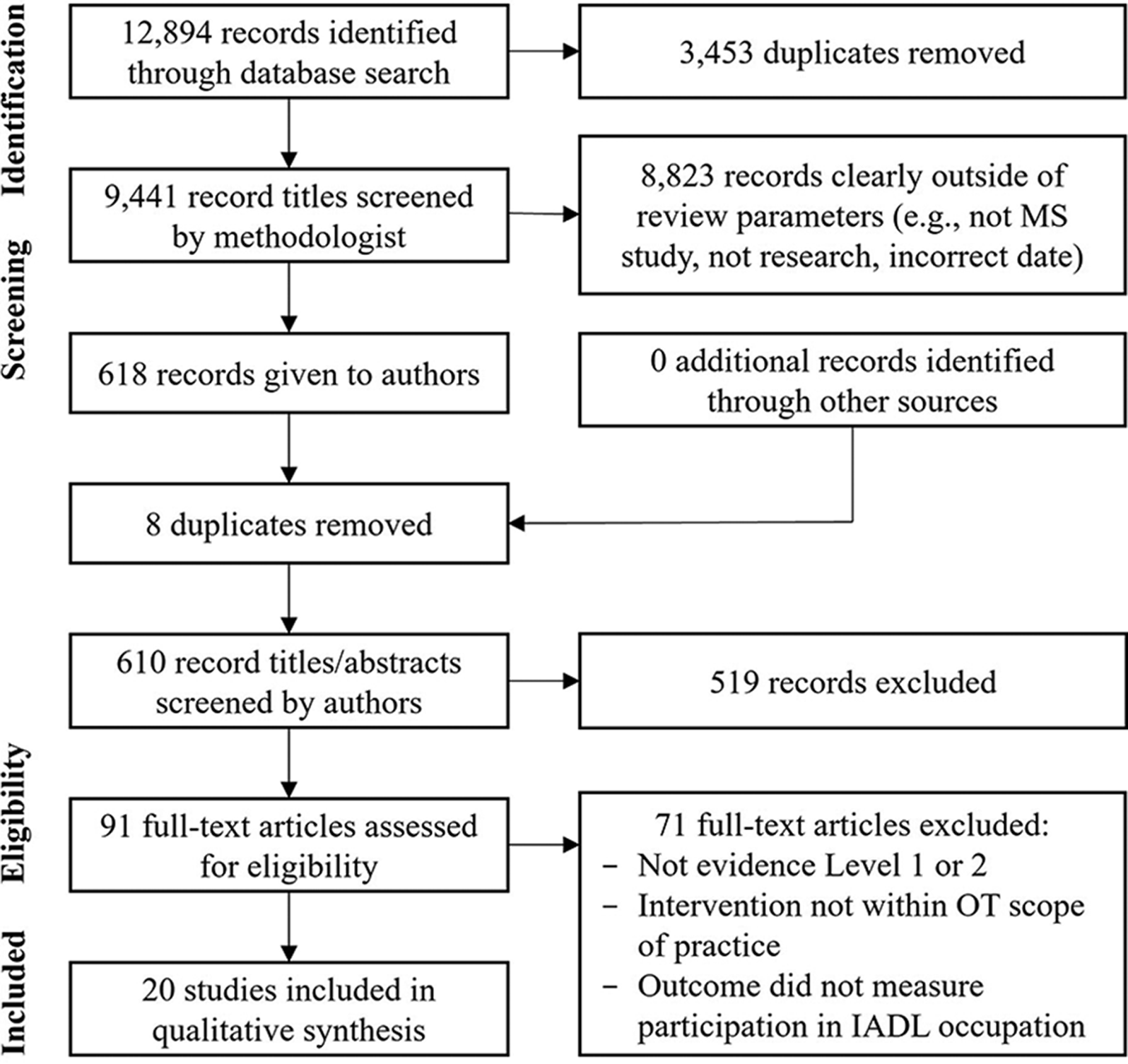
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
Study Characteristics
Settings
The final included studies covered a variety of contexts, including home (Carter et al., 2013, 2014; Heine et al., 2017; Kamm et al., 2015; Learmonth et al., 2017; Plow et al., 2014; Thomas et al., 2017, Turner et al., 2014), community-based spaces (Hayes et al., 2017), virtual spaces (Bruce et al., 2016; Dlugonski et al., 2012; Hayes et al., 2017; Learmonth et al., 2017; Motl et al., 2017; Pilutti et al., 2014; Sandroff et al., 2014; Suh et al., 2015; Thomas et al., 2017; Turner et al., 2016), outpatient clinics (Blikman et al., 2017; Bruce et al., 2016; Carter et al., 2013; Eyssen et al., 2013; Heine et al., 2017; Rietberg et al., 2014), and university labs (Akinwuntan et al., 2014; Carter et al., 2014). Multiple studies used a combination of settings for delivery because of the multicomponent nature of the intervention (Bruce et al., 2016; Carter et al., 2013, 2014; Hayes et al., 2017; Heine et al., 2017; Learmonth et al., 2017; Thomas et al., 2017).
Interventions
Coaching interventions were included in 11 studies addressing PA routines (Carter et al., 2013, 2014; Dlugonski et al., 2012; Hayes et al., 2017; Learmonth et al., 2017; Motl et al., 2017; Pilutti et al., 2014; Sandroff et al., 2014; Suh et al., 2015; Thomas et al., 2017; Turner et al., 2016). Both studies addressing medication routines involved coaching interventions (Bruce et al., 2016; Turner et al., 2014). The remaining studies consisted of a variety of interventions, including driving simulation (Akinwuntan et al., 2014), fatigue-management programs (Blikman et al., 2017), dexterity training (Kamm et al., 2015), prescribed PA programs (Heine et al., 2017; Plow et al., 2014), and rehabilitation services (Eyssen et al., 2013; Rietberg et al., 2014).
Outcomes
The outcome measures that were yielded from the systematic review were measures of PA in 11 studies (Carter et al., 2013, 2014; Dlugonski et al., 2012; Hayes et al., 2017; Learmonth et al., 2017; Motl et al., 2017; Pilutti et al., 2014; Sandroff et al., 2014; Suh et al., 2015; Thomas et al., 2017; Turner et al., 2016), medication management in 2 studies (Bruce et al., 2016; Turner et al., 2014), driving ability in 1 study (Akinwuntan et al., 2014), meal preparation in 1 study (Kamm et al., 2015), and home and financial management in 4 studies (Blikman et al., 2017; Eyssen et al., 2013; Heine et al., 2017; Rietberg et al., 2014). Although the majority of outcomes used were self-report, objective measurements of PA were used in some studies as an additional outcome, including pedometer (Dlugonski et al., 2012), accelerometer (Carter et al., 2014; Thomas et al., 2017), and moderate to vigorous PA (Learmonth et al., 2017; Motl et al., 2017; Pilutti et al., 2014).
Risk of Bias
The overall risk-of-bias analyses resulted in 7 low, 12 moderate, and 1 high risk-of-bias study. Overall risk of bias assessments are included in the evidence table (see Table A.1), and the full risk-of-bias evaluation is available in Table A.2.
Synthesis of Results by Theme
Physical Activity Health Management and Maintenance IADLs
Twelve studies measured participation or performance in PA health management and maintenance IADLs. Three subthemes were determined on the basis of interventions used in the set of articles.
Subtheme 1: Interventions emphasizing coaching
Six studies, 3 Level 1b (Pilutti et al., 2014; Sandroff et al., 2014; Turner et al., 2016) and 3 Level 2b (Dlugonski et al., 2012; Motl et al., 2017; Suh et al., 2015), measured the impact of multicomponent interventions with a coaching emphasis on PA. Four studies measured the effects of interventions consisting of educational content delivered through an Internet platform and video-based coaching sessions (Dlugonski et al., 2012; Motl et al., 2017; Pilutti et al., 2014; Sandroff et al., 2014). All 4 studies showed statistically significant improvements in self-reported PA participation or performance in favor of the intervention group. Another study measured the effects of telephone-delivered coaching sessions plus telehealth monitoring, resulting in statistically significant improvement in self-reported PA in the intervention group (Turner et al., 2016). The final study measured the effect of an intervention consisting of newsletter education about PA with telephone coaching sessions to reinforce information, ensure comprehension, and apply information to daily routines (Suh et al., 2015). The intervention group showed statistically significant improvement in self-reported PA. Five studies (Dlugonski et al., 2012; Motl et al., 2017; Pilutti et al., 2014; Suh et al., 2015; Turner et al., 2016) used the Godin Leisure-Time Exercise Questionnaire (GLTEQ), and the remaining study (Sandroff et al., 2014) used the International Physical Activity Questionnaire. On the basis of 3 Level 1b studies, RCT design, and consistent findings across articles, strong strength of evidence exists for interventions with a coaching emphasis.
Subtheme 2: Interventions involving prescribed physical activity with coaching
Five studies, all Level 2b (Carter et al., 2013, 2014; Hayes et al., 2017; Learmonth et al., 2017; Thomas et al., 2017), measured the impact of interventions that involved prescribed PA and coaching on participation in or performance of PA. Carter et al. (2013) measured the impact of PA plus cognitive–behavioral techniques. No statistically significant differences were found in PA. The follow-up RCT to this study measured the same protocol on PA participation with larger sample sizes (Carter et al., 2014). In contrast to the feasibility study, the intervention group significantly increased self-reported PA. The remaining 3 studies measured the effects of PA and coaching (Hayes et al., 2017; Learmonth et al., 2017 ; Thomas et al., 2017). In Hayes et al.’s (2017) study, results showed statistically significant within-group differences for self-reported PA but no between-group differences. Learmonth et al. (2017) found no significant improvements in PA. Thomas et al. (2017) reported only descriptive statistics but identified effect sizes of PA at 6 mo in favor of the intervention group. All 5 studies (Carter et al., 2013, 2014; Hayes et al., 2017; Learmonth et al., 2017; Thomas et al., 2017) used the GLTEQ as the primary outcome measure for PA participation. For interventions involving prescribed PA and coaching, moderate strength of evidence exists on the basis of mixed findings, 5 Level 2b studies, and pilot or feasibility design in 4 of 5 studies.
Subtheme 3: Intervention involving prescribed physical activity only
One Level 2b study (Plow et al., 2014) measured the impact of an intervention involving prescribed PA on participation or performance in PA. Plow et al. (2014) measured the impact of a prescribed home exercise program followed by educational pamphlets. The results showed a statistically significant increase in self-reported PA in the intervention group. The study used the GLTEQ and the revised version of the Physical Activity and Disability Survey. On the basis of the presence of only 1 Level 2b study with a small sample size, low strength of evidence exists for interventions involving prescribed PA.
Medication Health Management and Maintenance IADLs
Two studies, both Level 2b (Bruce et al., 2016; Turner et al., 2014), measured participation in or performance of medication routines. Bruce et al. (2016) measured the impact of motivational interviewing–informed, cognitive–behavioral therapy on medication reinitiation. The intervention group was significantly more likely to indicate reinitiating MS medication. Turner et al. (2014) measured the effects of telephone counseling plus telehealth monitoring. The intervention group showed statistically significant improvement in MS medication compliance at the 6-mo time point. On the basis of significant findings in both studies, 2 Level 2b studies, and smaller sample sizes, moderate strength of evidence exists.
Meal Preparation IADLs
One Level 2b study (Kamm et al., 2015) measured the effect of a dexterity training program on meal preparation participation. The intervention group showed statistically significant improvements in the meals and kitchen domain of the dexterity ADL questionnaire. Although the findings of the study are promising and the risk of bias is low, the strength of evidence is low because of the presence of only 1 Level 2b study with a small sample size.
Driving and Community Mobility IADLs
One Level 2b study (Akinwuntan et al., 2014) measured driving performance. The intervention consisted of driving training through the use of a high-fidelity simulator. No significant differences were observed between groups. On the basis of nonsignificant findings and 1 Level 2b study, low strength of evidence exists.
Home and Financial Management IADLs
Four studies, 1 Level 1b (Eyssen et al., 2013) and 3 Level 2b (Blikman et al., 2017; Heine et al., 2017; Rietberg et al., 2014), measured home and financial management participation or performance. Blikman et al. (2017) measured the effects of individual energy conservation management. Eyssen et al. (2013) compared client-centered occupational therapy with care-as-usual occupational therapy. Heine et al. (2017) measured the impact of aerobic training. Rietberg et al. (2014) measured the effects of multidisciplinary outpatient rehabilitation. None of the studies demonstrated statistically significant improvements for IADL participation or performance. On the basis of the lack of significant findings across studies and significant variability in delivered interventions, low strength of evidence exists.
Discussion
In this systematic review, we aimed to examine the effectiveness of interventions within the scope of occupational therapy to improve and maintain performance of and participation in IADLs among adults with MS. Although a previously completed systematic review by Yu and Mathiowetz (2014a, 2014b) focused on interventions, in this systematic review, we intended to expand on the findings by focusing on IADL occupational performance to increase specificity of clinical recommendations. Through analysis of themes cultivated from the final included articles, one subtheme demonstrated strong strength of evidence, one theme and one subtheme demonstrated moderate strength of evidence, and three themes and one subtheme demonstrated low strength of evidence (Table 3).
Overview of Results
Note. PA = physical activity.
The majority of included articles measured participation or performance in PA health management and maintenance IADLs. Research has shown that engagement in PA benefits aerobic capacity and muscular strength and may have benefits for mobility, fatigue, and health-related quality of life for those living with MS (Latimer-Cheung et al., 2013). Despite these documented benefits, people with MS are less physically active than the general population (Kinnett-Hopkins et al., 2017). This finding suggests that interventions promoting PA in the population with MS are needed. Systematic reviews examining the impact of behavior change interventions on PA among people with MS have shown that relatively short-term protocols lead to improvements in subjective outcomes of PA (Casey et al., 2018). This result aligns with the findings of this systematic review because interventions emphasizing coaching demonstrated strong evidence for increasing self-reported PA participation or performance among people with MS.
Despite the benefits of coaching and behavior change interventions described earlier, as well as promising preliminary evidence for prescribed PA interventions (Plow et al., 2014) for improving PA among people with MS, this systematic review found mixed results when coaching was combined with prescribed PA. In Hayes et al.’s (2017) study, one group received exercise plus coaching, and the other arm received exercise alone. The results showed significant within-group differences for self-reported PA but showed no between-group differences, which suggests that the coaching component did not affect PA participation. Thus, it seems that coaching alone or prescribed PA alone is more effective than a combined approach. However, Carter et al. (2014) reported significant improvement in self-reported PA participation after their intervention consisting of exercise plus coaching. Because of conflicting evidence, additional research is warranted to determine the conclusive impact of a combined intervention on PA participation or performance. On the basis of the current available evidence from this systematic review, the strongest evidence for increasing PA participation or performance in those living with MS is through interventions that emphasize coaching without prescribed PA.
MS disease-modifying therapies (DMTs) work to prevent relapse and disease progression, which is important for protecting functional abilities and reducing disease severity. One population-based study (Evans et al., 2016) reported a 75% adherence rate with MS DMT, which, although higher than that among other chronic disease populations, still leaves 25% of people missing doses. Therefore, interventions to support medication compliance could benefit people with MS in managing their DMT regimen. Studies included in this systematic review (Bruce et al., 2016; Turner et al., 2014) show moderate evidence for the utilization of coaching interventions to support participation in medication health management and maintenance IADLs. However, because of varied points of measurement related to medication routines in the included studies, additional research is needed to increase the strength of evidence and related clinical recommendations.
Analysis of articles that measured meal preparation, home and financial management, and driving IADL participation or performance demonstrated low strength of evidence. No significant findings were found across the studies addressing driving, home management, and financial management. However, the effect of a dexterity training program on meal preparation participation showed significant improvements (Kamm et al., 2015). Although the findings of that study are promising and the risk of bias is low, additional research is necessary to strengthen the evidence and clinical recommendations.
Limitations
Articles that were not published in English were excluded from the study if an English translation was unavailable, which may have resulted in the exclusion of articles that would have added to the strength of evidence of themes and conclusions. The heterogeneity of interventions in the home and financial management routines theme made it difficult to make comparisons. The majority of the included studies had moderate risk of bias, which was most often because of limitations regarding blinding in behavioral intervention protocols. The majority of studies used self-report outcome measures, which increases bias. Finally, as with any review, the possibility of publication bias exists; in addition, pertinent articles for inclusion may have been missed.
Future Considerations
Overall, the majority of final included studies were not developed and delivered by occupational therapy practitioners. Additionally, half of the final included articles involved coaching interventions, the majority of which were delivered by physical therapy or counseling professionals. Because of the focus of coaching interventions on behavior change, as well as habit and routine modifications, these interventions fall within the occupational therapy scope of practice. Thus, occupational therapy practitioners and researchers should consider increasing involvement in research that focuses on IADL participation and performance, as well as coaching-based research studies, in the MS population.
Because of the focus of this systematic review on IADL participation and performance, the use of an outcome measure that assessed IADLs was required for article inclusion. Thus, many studies that involved interventions related to PA, self-regulation behaviors, and fatigue management were excluded because of the lack of IADL outcome measure use. Therefore, to better understand the impact of occupational therapy interventions on MS performance or participation in IADLs, it is important to increase the inclusion of IADL outcome measures in MS-related research and clinical practice. Moreover, increasing use of objective assessments of IADL participation, such as moderate to vigorous PA, will reduce bias and strengthen findings and application to clinical care.
Occupations can be the end goal or the means by which a goal is achieved. For instance, a client may have a goal of improved participation in work-related tasks, but because of severe anxiety, they may not be functionally capable of completing the tasks. An occupational therapy practitioner may work with the client on establishing a regular routine of meditation or PA that promotes anxiety management so that the client can improve their functional work abilities. This systematic review addresses occupations as the end goal. Thus, it would be beneficial in future systematic reviews to consider language that addresses occupation as a means to capture the totality of the occupational therapy scope of practice in meeting the IADL needs of the population with MS.
Implications for Occupational Therapy Practice
Occupational therapy practitioners should address health management and maintenance IADLs, including PA and medication routines, as part of a plan of care when treating people with MS. Occupational therapy practitioners’ distinct skills in supporting the development of health-promoting habits and routines paired with utilization of evidence-supported interventions emphasizing coaching can support increased independence with health management and reduce the negative impact of MS on daily activity participation. Thus, occupational therapy practitioners should consider utilization of coaching interventions in their plans of care to address PA and medication routine participation when treating people with MS; consider additional training in social–cognitive theory, motivational interviewing, and similar coaching models to support integration of related interventions into practice; and increase inclusion of assessments that measure the impact of occupational therapy interventions on IADL performance when treating the population with MS.
Conclusion
The final articles included in this systematic review demonstrate strong support for coaching interventions in addressing PA participation and moderate support for coaching interventions in addressing medication routines. Preliminary evidence exists for dexterity training programs for improving meal preparation and the use of prescribed PA programs for increasing PA participation. Overall, limited representation of IADLs unrelated to health management was found because the majority of assessments that were used focused on health management routines. Thus, increased occupational therapy–delivered research studies on performance are needed for a variety of IADLs among the populations with MS. Through these recommendations, occupational therapy practitioners can better meet the needs of the population with MS and improve IADL occupational engagement.
Footnotes
*
Indicates studies included in the systematic review.
Acknowledgments
The authors have no conflicts of interest, funding, or sponsorship to disclose. This project was supported in part by the American Occupational Therapy Association. Thanks to Deborah Lieberman, Elizabeth Hunter, Susan Cahill, and Hillary Richardson for their guidance and support throughout the process of this review.
Appendix. Evidence and Risk-of-Bias Tables for the Systematic Review
Risk-of-Bias Table for the Studies Included in the Systematic Review
| Citation | Selection Bias | Performance Bias | Detection Bias | Attrition Bias: Incomplete Outcome Data | Reporting Bias: Selective Reporting | Overall Risk of Bias Assessment | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Random Sequence Generation | Allocation Concealment | Baseline Differences Between Intervention Groups | Blinding of Participants During the Trial | Blinding of Study Personnel During the Trial | Blinding of Outcome Assessment: Self-Reported Outcomes | Blinding of Outcome Assessment: Objective Outcomes | ||||
| Akinwuntan et al. (2014) | − | − | − | − | − | + | + | − | + | M |
| Blikman et al. (2017) | + | + | + | − | + | − | − | + | + | L |
| Bruce et al. (2016) | + | + | + | − | − | − | − | + | + | M |
| Carter et al. (2014) | − | − | + | − | − | + | − | + | + | M |
| Carter et al. (2013) | − | − | + | − | + | + | + | + | + | L |
| Dlugonski et al. (2012) | + | − | + | − | − | + | − | + | + | M |
| Eyssen et al. (2013) | + | − | − | + | + | + | − | + | − | M |
| Hayes et al. (2017) | − | − | − | + | + | + | + | − | + | M |
| Heine et al. (2017) | + | − | + | − | + | + | + | − | + | L |
| Kamm et al. (2015) | + | − | + | − | + | + | + | + | + | L |
| Learmonth et al. (2017) | + | + | + | − | − | − | + | − | + | M |
| Motl et al. (2017) | + | + | + | − | − | + | + | + | + | L |
| Pilutti et al. (2014) | + | + | − | − | − | + | − | + | + | M |
| Plow et al. (2014) | + | + | + | − | − | − | − | − | − | M |
| Rietberg et al. (2014) | + | + | + | − | − | − | + | + | + | L |
| Sandroff et al. (2014) | + | − | + | − | − | + | − | + | + | M |
| Suh et al. (2015) | + | − | + | − | + | − | − | + | + | M |
| Thomas et al. (2017) | + | + | − | − | − | − | − | − | − | H |
| Turner et al. (2016) | + | + | + | − | − | − | − | + | + | M |
| Turner et al. (2014) | + | + | + | − | − | − | + | + | + | L |
Note. Categories for risk of bias are as follows: low risk of bias (+), high risk of bias (–). Scoring for overall risk of bias assessment is as follows: L = low overall risk of bias (0–3 minuses); M = moderate overall risk of bias (4–6 minuses); H = high risk of bias (7–9 minuses). Table format adapted from “A Revised Tool for Assessing Risk of Bias in Randomized Trials,” by J. P. T. Higgins, J. A. C. Sterne, J. Savović, M. J. Page, A. Hróbjartsson, I. Boutron, . . . S. Eldridge, 2016, Cochrane Database of Systematic Reviews 2016, Issue 10 (Suppl. 1), 29–31. https://doi.org//10.1002/14651858.CD201601.
This table is a product of AOTA's Evidence-Based Practice Program and AOTA and is copyright ©2022 by the American Occupational Therapy Association. It may be freely reproduced for personal use in clinical or educational settings as long as the source is cited. All other uses require written permission from the American Occupational Therapy Association. To apply, visit http://www.copyright.com.
Citation: Cunningham, R., & Uyeshiro Simon, A. (2022). Interventions for instrumental activities of daily living among adults with multiple sclerosis: A systematic review (Table A.2). American Journal of Occupational Therapy, 76, 7602205130. https://doi.org/10.5014/ajot.2022.049092