
Abstract
Precis (for TOC): This article reviews existing research on coaching models used by occupational therapists in early intervention and concludes that they are a viable intervention. Future research should seek to demonstrate the efficacy of caregiver coaching in achieving child and family outcomes and the training needed to implement coaching practices.
Early intervention (EI) services aim to have a positive affect on the development of infants and toddlers ages birth to 36 mo with diagnosed or potential developmental delays and to support families in meeting their children’s special needs (Individuals With Disabilities Education Improvement Act of 2004 [IDEA], Pub. L. 108-446). Defined as a primary service of EI under Part C of IDEA, occupational therapy aims to improve a child’s functional skills and ability to participate in everyday routines and activities. The 1997 Individuals With Disabilities Education Act Amendments (Pub. L. 105-117) required that EI services be provided, to the maximum extent possible, in a child’s natural learning environment, which includes home and community settings (Dunst et al., 2001). In alignment with Part C of IDEA, family-centered care has become the foundation of EI (Kuo et al., 2012). In family-centered care, the family is seen as a whole, and families collaborate with health care providers to set goals and make decisions about the care process (Kuo et al., 2012; Rush et al., 2003; Shields, 2015). Family-centered care is evident, for example, in the process of creating the required Individualized Family Service Plan (IFSP), in which caregivers collaborate with multidisciplinary providers to prioritize family goals and make decisions concerning their child’s services and supports (Katsiyannis et al., 2001). Thus, for more than 2 decades, EI practitioners have been tasked with developing effective methods for supporting young children and their families to meet their defined goals through intervention approaches that apply the concepts of family-centered care in natural learning environments (American Occupational Therapy Association [AOTA], 2019).
The term coaching emerged in the literature toward the end of the 1990s, as EI professionals and researchers sought to reconceptualize common intervention approaches, such as parent education and parent teaching, to create a distinct model for practice that would reflect the reciprocal and collaborative practitioner–caregiver relationship inherent to family-centered care (Kemp & Turnbull, 2014; Rush et al., 2003). Closely aligned with the goal of IDEA Part C to strengthen parents’ ability to support their children’s development and drawing on adult learning strategies, coaching promotes caregiver reflection and problem solving in the process of gaining and refining knowledge and skills to better support children during life routines in typical family environments (Graham et al., 2010; Rush et al., 2003). Between 2000 and 2010, parent coaching became an accepted and often expected practice among multidisciplinary providers in EI (Kemp & Turnbull, 2014), even though a clear pragmatic definition of coaching and what it looks like in practice has been lacking (Friedman et al., 2012; Graham et al., 2018; Kemp & Turnbull, 2014), and evidence to guide the designation of coaching as a model of best practice is limited (Campbell & Coletti, 2013; Kessler & Graham, 2015).
The core concepts of coaching are strongly aligned with the professional paradigm of occupational therapy, in which practitioners across practice areas are trained to analyze a client’s existing habits, routines, and roles, in their particular contexts and physical and social environments, to create interventions to maximize participation in valued life activities (AOTA, 2020). The Occupational Therapy Practice Framework: Domain and Process (4th ed.; AOTA, 2020) further highlights co-occupations as highly interactive occupations that inherently involve two or more people who may share, as in the case of caregiving activities involving infants and young children, a high level of physical and emotional connection. Although EI is a multi- and transdisciplinary service (AOTA, 2019), occupational therapy’s defined scope of practice appears to distinctly position occupational therapy practitioners to deliver family-centered interventions within a family’s existing routines and environments, as caregiver coaching aims to do.
Indeed, occupational therapy–specific coaching interventions have been developed for working with parents and caregivers (Graham et al., 2009; Kessler & Graham, 2015). These interventions include occupational performance coaching, which uses a collaborative problem-solving framework to guide parents to solve occupational performance challenges (Graham et al., 2009), and contextual intervention, which is designed for children with autism spectrum disorder and incorporates the family’s natural environment and everyday routines and the child’s sensory processing patterns (Dunn et al., 2012). Currently, AOTA does not endorse a particular model or approach for EI service delivery; it states that further research is needed (AOTA, 2019); however, multiple states recommend or require a coaching model in EI service delivery, with varying requirements for practitioner training in its use (Massachusetts Department of Public Health, 2013).
Although evidence exists for the use of caregiver coaching across multidisciplinary pediatric practice areas (Dunn et al., 2012; Graham et al., 2013; Miller-Kuhaneck & Watling, 2018; Novak & Honan, 2019), our intention with this scoping review was to examine the evidence currently available on the use of caregiver coaching specifically within occupational therapy services delivered through EI in the United States, given the requirements of IDEA Part C, the apparent suitability of coaching to support co-occupations central to family life with young children, and the distinct scope of practice underlying occupational therapy practitioners’ delivery of this support. Thus, the objective of this scoping review was to examine (1) the current working definition of coaching as it has evolved over 2 decades of EI practice and (2) the ways in which occupational therapy practitioners in the United States are using caregiver coaching in EI.
Method
Following Arksey and O’Malley’s (2005) framework as well as updated methodological guidance from Peters et al. (2020), we conducted this scoping review to explore the topic of parent coaching in EI to help further direct family-centered care in occupational therapy. Choosing a scoping review as the method of study more readily aligned with the goals of a scoping review, which are to explore, describe, and understand the current scholarship rather than to inform clinical practice or determine the efficacy of an approach, as with systematic reviews (Peters et al. 2020). This methodology was chosen with the aim of clarifying the term parent coaching, which lacks consistent definition in the EI literature and in practice (Kemp & Turnbull, 2014), and how occupational therapists incorporate this service delivery model in their practice. The five steps of the scoping review methodology were followed: (1) identifying the research questions, (2) identifying relevant research articles, (3) selecting relevant studies, (4) charting the data, and (5) collecting and summarizing the data.
Two questions guided this scoping review: (1) “What is the current working definition(s) of coaching as it has evolved over 2 decades of EI practice?” and (2) “How are occupational therapy practitioners in the United States utilizing parent coaching as an intervention approach in EI practice?”
To ensure a comprehensive search, a team of four graduate students (Emily Feit, Alexys Tirado, Diana Ottomanelli, and Melissa Celio) under the supervision of the lead researcher (Francine M. Seruya) searched the following online databases for eligible peer-reviewed articles: CINAHL Complete, CINAHL with full text, Education Research Complete, ERIC, PsycARTICLES, PsycINFO, Teacher Reference Center, Academic Search Premier, Academic Search Complete, Socindex with full text, and Social Work Abstracts. We intentionally selected these databases because they most readily aligned with the topic. Parent coaching is a service delivery model designated as part of education law (IDEA, Part C), not traditional medical or rehabilitation service delivery models. Biomedical databases, such as MEDLINE or Embase, would include the latter interventions and were thus excluded. Databases providing grey literature, including theses, dissertations, or only abstracts, were also excluded because the evidence suggests that unpublished research is not a frequent component of scoping or systematic reviews. In addition, the inclusion of grey literature in meta-analyses yields minimal differences in statistical significance or effect size (Hartling et al., 2017). We therefore deemed it not appropriate for this scoping review.
The key terms used in the searches were as follows: “parent coaching” OR “parent training” OR “parent education,” AND “early intervention,” AND “occupational therapy” OR “occupational therapist” OR “OT.” All literature searches were limited to English-only articles published from 2000 through 2020. These publication dates were chosen because of the increase in use of the term coaching and the emphasis on this approach in EI service provision beginning in 2000, relative to the earlier terms or approaches parent training and parent education, which were predominant features of family-centered practice during the 1990s (Kemp & Turnbull, 2014). Still, as the term coaching was being introduced, there were variations in the terminology, including training and education. Accordingly, in an attempt to capture all relevant research, we included these terms to avoid limiting the scope of the review as a result of semantic differences.
Studies included were intervention based and conducted with parents or caregivers of infants or toddlers with disabilities or developmental delay or at high risk for developmental delay. Studies that included children outside of the age range of birth to 36 mo were excluded. Included articles used the term coaching or training or described an intervention or referred to some aspect of an intervention involving parent coaching, parent training, or parent education. Therefore, articles that did not define or describe how these approaches were used in intervention sessions or that were purely descriptive articles and not intervention studies were excluded.
In addition, given differences in governmental funding and frameworks for the provision of EI and other services internationally, and given the unique guidelines set forth in IDEA Part C as they relate to EI service provision solely in the United States, studies conducted outside of the United States were excluded. Finally, to be included in the scoping review, the interventions described had to be delivered at least partially in the context of home visits, as per IDEA, Part C, guidelines requiring service provision in natural settings. Therefore, studies of services provided exclusively in hospital, neonatal intensive care unit, preschool, or other settings were excluded. Studies were also excluded if occupational therapy was not mentioned as one of the services being delivered. We did not consider or report on level of evidence or risk-of-bias assessment when determining whether to include or exclude articles because the intention of a scoping review is to describe and assess the available evidence rather than present a systematic analysis of the evidence to inform clinical decision making or practice (Peters et al., 2020).
Collectively, we reviewed article titles and abstracts for relevance on the basis of the inclusion and exclusion criteria. Disagreements about inclusion were discussed in depth to reach consensus. The articles were divided evenly among the authors, and each author then reviewed their articles in full to determine eligibility. The group discussed any article about which the primary reviewer was undecided. To complete study selection, a background search of the reference lists of several systematic and other literature reviews obtained through the database search, as well as the reference lists of all included articles, was then conducted. The study selection process is shown in Figure 1.
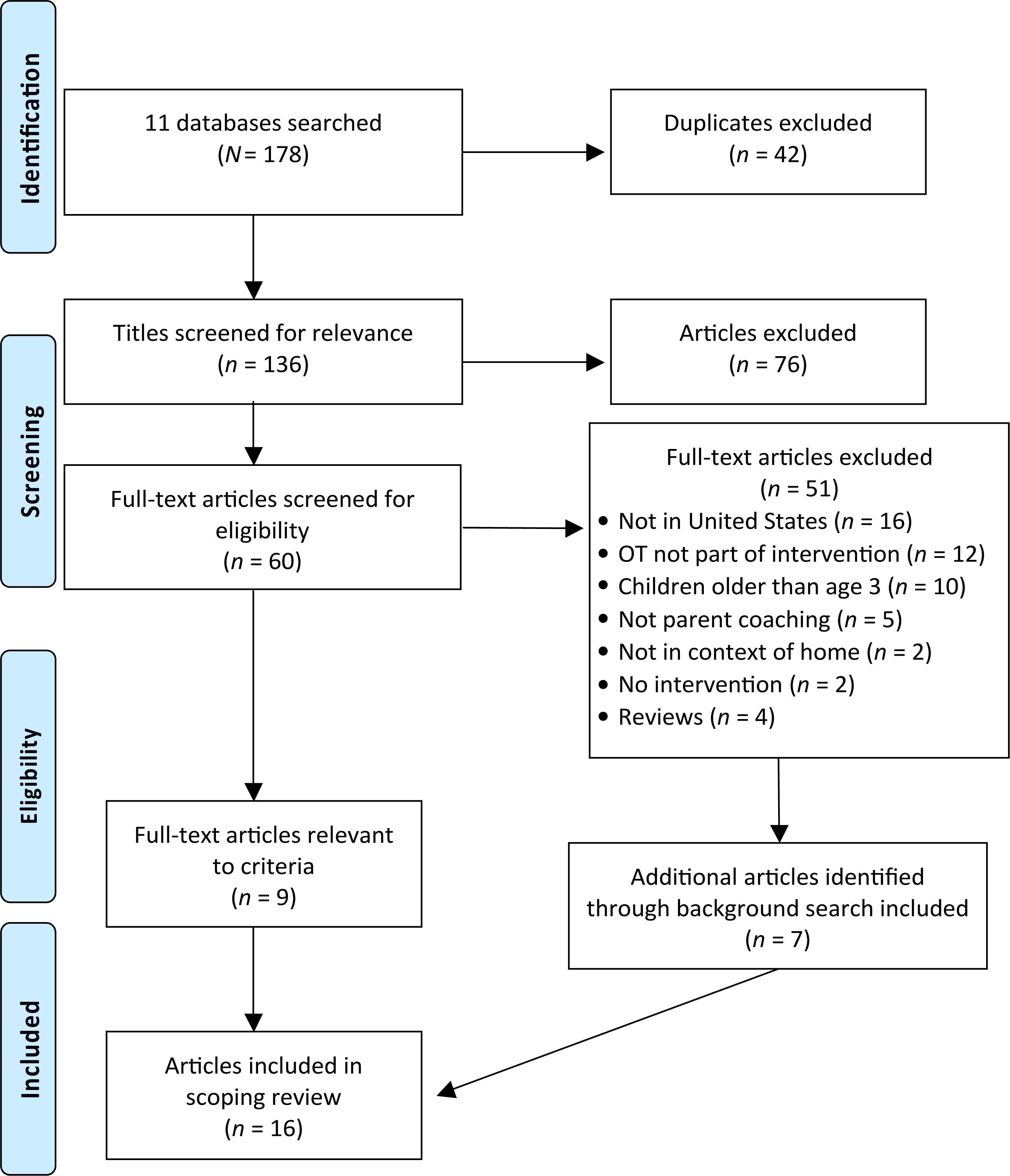
Flow diagram of study selection.
Once articles were selected, each article was reviewed and coded by its initial reviewer with respect to the study’s specific research questions. Once initial coding had been completed, the group collectively collapsed the codes into categories. Thematic analysis was conducted on the resultant categories to address the research questions.
Results
A total of 178 articles were retrieved through our initial database search, and 136 articles remained after duplicates (n = 42) were removed. Seventy-six articles were excluded for irrelevance after title and abstract screening, leaving 60 articles for further review. After the application of inclusion and exclusion criteria, 51 articles were excluded. A background search of the reference lists of the 9 remaining studies and of the systematic and other literature reviews excluded from this scoping review yielded an additional 7 eligible articles, resulting in the inclusion of 16 total articles in this scoping review.
The aim of this scoping review was to examine the current working definition of coaching and how it is used in occupational therapy practice in EI. We found that few studies have explored coaching as an intervention approach in occupational therapy services in EI. Of the 16 articles that fit the criteria for this scoping review, 5 addressed coaching practice specifically within occupational therapy (Colyvas et al., 2010; Fields et al., 2016; Hoyt Drazen et al., 2014; Kramer et al., 2018; Schultz-Krohn & Cara, 2000), and 11 were multidisciplinary studies. Two occupational therapy–specific studies focused specifically on the Parents as Teachers program for children with sickle cell disease (Fields et al., 2016; Hoyt Drazen et al., 2014), and 4 of the multidisciplinary studies focused on the routines-based intervention approach of the Chicago Early Intervention Project program (Salisbury et al., 2010, 2012; Salisbury & Copeland, 2013; Salisbury & Cushing, 2013). Campbell and Sawyer (2009) and Colyvas et al. (2010) examined the use of participation-based practice in EI sessions. Only 2 studies were intervention studies that explored specific child outcomes (Fields et al., 2016; Salisbury & Copeland, 2013), whereas 9 studies focused on provider perceptions and provider-related outcomes (Campbell & Coletti, 2013; Campbell & Sawyer, 2009; Colyvas et al., 2010; Friedman et al., 2012; Marturana & Woods, 2012; Salisbury et al., 2010, 2012; Salisbury & Cushing, 2013; Stewart & Applequist, 2019). The full results of the selected articles are described in Table A.1 in the Supplemental Appendix (available online with this article at https://research.aota.org/ajot).
Definition: What Is Coaching?
The included studies used many overlapping, and sometimes interchangeable, terms, including triadic practice (Salisbury & Cushing, 2013), collaborative consultation (Salisbury et al., 2010; Stewart & Applequist, 2019), nondidactic learning (Schultz-Krohn & Cara, 2000), participation-based (Campbell & Sawyer, 2009; Colyvas et al., 2010), family-guided routines-based practice (Marturana & Woods, 2012; Salisbury & Cushing, 2013), and caregiver teaching (Campbell & Coletti, 2013; Colyvas et al., 2010), with no clear or consistent distinction between the terms and how they relate to coaching as a whole. Still, although the overall objectives of these approaches may differ (e.g., improved parent–child relationship vs. increased child participation in routines), parent or caregiver coaching is viewed as a way of meeting these objectives.
Authors described various methods through which coaching is accomplished, including observation, conversation, information sharing, data collection, problem-oriented reflection, direct teaching, joint interaction, demonstration, sharing feedback, problem solving, planning, caregiver practice with feedback, guided practice, modeling, listening, and prompting. The terms used in the reviewed studies are defined in the Table A.1 note. Several authors emphasized the foundation of coaching practices in theories of adult learning, which include socially and contextually based methods (Schultz-Krohn & Cara, 2000), experiential and scaffolded learning (Friedman et al., 2012; Kramer et al., 2018), reflection (Friedman et al., 2012; Kramer et al., 2018; Marturana & Woods, 2012), and validation of caregiver perspectives (Kramer et al., 2018).
In an attempt to create a standard definition of coaching as a practice in EI, Friedman et al. (2012) developed a taxonomy of behaviors used during intervention sessions, defining and describing the following eight coaching behaviors: (1) conversation and information sharing, (2) observation, (3) joint interaction, (4) direct teaching, (5) demonstration with narrative, (6) guided practice with feedback, (7) caregiver practice with feedback, and (8) reflection and problem solving. Several of the reviewed articles use the definitions noted in the taxonomy to frame their studies but did so partially or using differing terminology. For example, Campbell and Coletti (2013) used five caregiver teaching strategies nearly identical to those identified by Friedman et al. (2012), and Salisbury et al. (2012) omitted joint interaction because it did not promote caregivers as leaders—in their view, the express goal of family-centered coaching practice. Other studies further noted that although conversation and information sharing were predominantly used as part of collaborative consultation, they do not inherently promote child–caregiver relationships in everyday activities (Cambray-Engstrom & Salisbury, 2010; Colyvas et al., 2010; Marturana & Woods, 2012).
Implementation: What Are Occupational Therapy Practitioners Doing?
The reviewed articles reflect that EI providers’ understanding of coaching practices does not always correspond with their use of these practices during intervention. Several of the reviewed articles were conducted with the intention of further understanding this disconnect (Campbell & Coletti, 2013; Salisbury et al., 2010, 2012). The findings were varied, with some studies finding that, although practitioners knew that participation-based services, inclusive of coaching practices, were considered best practice (Campbell & Sawyer, 2009 ; Colyvas et al., 2010), they implemented relatively few coaching strategies in practice (Friedman et al., 2012; Gmmash & Effgen, 2019) or continued to implement a traditional child-focused approach, leading to nominal parent–child facilitated interactions (Campbell & Sawyer, 2009; Colyvas et al., 2010; Stewart & Applequist, 2019).
Other studies found that providers were able to correctly identify and demonstrate coaching strategies (Campbell & Coletti, 2013) and used a range of strategies in practice; however, they underreported their use in documentation, perhaps because of the problem of overly detailed gradations in the defined strategies (Salisbury et al., 2012). Studies that discussed provider perceptions related to coaching in EI identified that providers encountered multiple challenges and barriers to the implementation of coaching practices (Campbell & Sawyer, 2009; Salisbury et al., 2010; Stewart & Applequist, 2019) and revealed EI service providers’ tendency to be apprehensive in implementing a coaching approach during services (Stewart & Applequist, 2019).
When using a coaching model, part of the practitioner’s role is to encourage parents’ sense of self-efficacy and competence by strengthening their ability to confidently teach their own children in the context of family life (Salisbury & Copeland, 2013; Schultz-Krohn & Cara, 2000). The expectation that providers will use the natural environment to consult with, train, and educate caregivers to promote their child’s growth and development within their regular activities and routines, thus embedding coaching strategies into everyday contexts, was a key element emphasized in many of the reviewed studies (e.g., Colyvas et al., 2010; Marturana & Woods, 2012; Salisbury et al., 2010). Cambray-Engstrom and Salisbury (2010) and Salisbury and Copeland (2013) found that caregivers felt more freedom to express themselves and influence intervention results when services occurred in the natural environment.
Even with the emphasis on embedding intervention into family routines, many studies (e.g., Cambray-Engstrom & Salisbury, 2010; Campbell & Coletti, 2013; Marturana & Woods, 2012) found that play was the primary activity used for intervention. Moreover, coaching strategies involving higher levels of active caregiver participation (e.g., caregiver practice with feedback) were more often associated with play activities (Cambray-Engstrom & Salisbury, 2010; Campbell & Coletti, 2013), and discussion and other forms of interaction in which the caregiver is less actively involved were associated with nonplay activities (Campbell & Coletti, 2013). Several authors emphasized the importance of provider training and ongoing continuing education and support to move from awareness to implementation of coaching strategies (Campbell & Sawyer, 2009; Salisbury et al., 2010) in varied contexts and in everyday family routines (Marturana & Woods, 2012).
Studies discussed additional factors that contributed to the successful implementation of coaching strategies, including child characteristics, parent characteristics and expectations (Salisbury et al., 2010), family dynamics (Schultz-Krohn & Cara, 2000), and provider beliefs (Campbell & Sawyer, 2009; Stewart & Applequist, 2019). Notably, the medical complexity of the child’s condition was identified as a potential barrier to coaching practices (Friedman et al., 2012; Salisbury et al., 2010), with Stewart and Applequist (2019) indicating that providers viewed coaching as infeasible, and potentially counterproductive, for families with medically complex children, because they had concerns related to parents’ implementation of certain interventions. However, Campbell and Coletti (2013) and Salisbury et al. (2010) found, in the absence of medical conditions, no significant association between successful coaching implementation and a child’s degree of disability.
Five studies looked specifically at the feasibility, implementation, and effectiveness of coaching in socioeconomically, racially, and ethnically diverse communities (Cambray-Engstrom & Salisbury, 2010; Hoyt Drazen et al., 2014; Kramer et al., 2018; Salisbury et al., 2010; Stewart & Applequist, 2019). Salisbury et al. (2010) described characteristics of family (e.g., composition, living arrangements, and culture) and the built environment that affect practitioners’ perceptions of successful program implementation. Factors affecting practitioners’ ability to implement coaching interventions included culture-specific views of child rearing and the role of providers and therapists, family etiquette, family and space configurations, and conceptual language barriers (Salisbury & Cushing, 2013; Salisbury et al., 2010; Stewart & Applequist, 2019).
Studies demonstrated the feasibility of coaching as an effective intervention to aid parents in identifying environmental barriers to participation in the home and at community and policy levels (Kramer et al., 2018), provide in-home parent education to support parent–child interaction (Fields et al., 2016; Hoyt Drazen et al., 2014), and facilitate children’s developmental milestones in diverse contexts (Hoyt Drazen et al., 2014). Studies found that when goals and interventions are culturally relevant and collaborative, the focus shifts to culturally appropriate developmental milestones, which can lead to increased language development and interaction between parent and child, empowering caregivers and facilitating their ability to express their beliefs and ideas through interactions with their child (Cambray-Engstrom & Salisbury, 2010; Schultz-Krohn & Cara, 2000; Stewart & Applequist, 2019).
Overall, this scoping review revealed the continued absence of a single operational definition of caregiver coaching in EI practice. Despite this, training and professional development to educate providers about coaching strategies and their use has the potential to increase practitioners’ confidence, frequency, and range of strategies used (Friedman et al., 2012; Salisbury et al., 2010; Stewart & Applequist, 2019) as well as their use of strategies in occupations such as caregiving; self-care; and family, community, and preacademic activities (Marturana & Woods, 2012). Studies indicated that the use of coaching strategies by EI service providers can empower caregivers to engage during the intervention process and acquire the necessary skills to actively contribute to their child’s development and participation in daily activities. This scoping review confirms the lack of peer-reviewed literature on the efficacy of parent coaching as it relates to child and family outcomes and, similarly, found that studies of occupational therapy–specific coaching interventions within EI were limited.
Discussion
This scoping review examined the definitions of parent coaching and their application to EI service provision by occupational therapists. The reviewed studies demonstrate that coaching varies widely in practice and terminology. Although providers are familiar with the importance of collaborating with the family during intervention, they are often unsure or skeptical about the use of coaching as an approach to intervention in EI (Campbell & Sawyer, 2009; Stewart & Applequist, 2019). However, when coaching is used effectively, there appear to be core components that can be used flexibly, indicating that coaching is a dynamic framework for service delivery. This flexibility is an important aspect of EI service delivery among diverse families and communities; however, it can also create a lack of clarity as to which strategies will work best or when strategies should be implemented.
When defining coaching itself, the literature has focused on the behaviors associated with coaching, with little attention to the necessity of implementing this intervention approach in the natural context of the child and family. Given, for example, that practitioners have predominantly used play as an activity for intervention in routines-based practice (Cambray-Engstrom & Salisbury, 2010; Campbell & Coletti, 2013; Marturana & Woods, 2012), the contextually based service delivery implicit in coaching models may not be universally understood or embraced. Although play is an important occupation during childhood, children are expected to fulfill multiple roles in the family and to participate in the routines, occupations, and co-occupations associated with each role. Thus, it may bear articulating that definitions of coaching, in addition to its associated behaviors, vary on the basis of context. This viewpoint is consistent with Campbell and Sawyer (2009), who advised that the beliefs and values underlying participation-based practice must be clearly expressed if changes in practice are to be adopted, and also with Schultz-Krohn and Cara (2000), who stated that when practitioners are able to listen and learn about the family’s habits, routines, and unique rituals and mannerisms, they can maximize the family’s strengths in order to administer intervention.
Just as occupational therapists are in a position to leverage their expertise in the area of embedding intervention into clients’ existing habits, routines, and roles and in their distinct contexts and environments (AOTA, 2020), in the delivery of caregiver coaching intervention, Kramer et al. (2018) offered an example of how the application of occupational therapy’s unique scope of practice can potentially expand the conceptual boundaries of caregiver coaching beyond embedded intervention. Kramer et al. (2018) successfully developed an approach in which occupational therapy–implemented parent coaching did not directly involve parent–child interaction but supported parents’ ability to identify environmental barriers to their child’s participation in occupations inside and outside the home and orient themselves to problem solving at the home, community, and policy levels. Thus, the approach promotes parenting skills such as leadership and advocacy, which go beyond one-on-one interaction with their children and are especially relevant for parents of children with disabilities. This example broadens the current conceptualizations of caregiver coaching in natural environments, which focus on strategies used by practitioners to promote caregiver engagement directly with their child.
The intention for participation-based, embedded intervention in EI service provision, and the focus on parent learning specific to EI coaching practices, calls into question the types of goals and assessments typically used in EI practice. In EI, contrary to best practice, IFSPs often contain component-based goals for the child rather than participation-based goals for the child and family. For example, Gmmash and Effgen (2019) found that 89% of physical therapy and occupational therapy providers who treat children with cerebral palsy in early childhood believe caregivers’ goals are the most important piece of developing an EI treatment plan; however, 74% hardly ever or never use outcome measures such as the Canadian Occupational Performance Measure (Law et al., 2019) or goal attainment scaling (Turner-Stokes, 2009) to help caregivers identify priority areas of participation when developing therapy goals for their child. Assessments used to gauge progress on IFSP goals are, likewise, typically component based. This may contribute to the paucity of evidence for the effectiveness of coaching practices and highlights an important gap between research, in which efficacy studies containing child outcomes have been rare, and practice, in which child outcomes are predominantly used in goal planning and progress tracking. Functional and participation-based assessments are needed to accurately determine the effectiveness of coaching practices aimed at increased child participation. Moreover, the fact that assessments are component based rather than function or participation based calls into question the typically child-centered, rather than family-centered, goals typical of IFSPs and whether parent attributes, such as confidence and self-efficacy, and skills, such as ability to use compensatory strategies or adaptive equipment during family routines, should be included as areas for assessment and intervention.
Evidence indicates that caregiver coaching has a positive effect on parents’ self-efficacy and their ability to more effectively address their children’s needs (Salisbury & Copeland, 2013); however, it is also clear that coaching requires parents’ active participation (Salisbury et al., 2010). Coaching is not intuitive (Friedman et al., 2012, Marturana & Woods, 2012; Stewart & Applequist, 2019), and many therapists do not know how to guide caregiver engagement in the process (Salisbury et al., 2010; Schultz-Krohn & Cara, 2000). For families to benefit from coaching interventions, EI service providers must have adequate and ongoing training in order to effectively implement interventions (Campbell & Sawyer, 2009; Friedman et al., 2012; Marturana & Woods, 2012; Stewart & Applequist, 2019).
Training should address the beliefs and values underlying service delivery models (Campbell & Sawyer, 2009), offer providers opportunities to demonstrate the application of new skills and receive performance-based feedback (Marturana & Woods, 2012), and include instruction in culturally responsive practices (Cambray-Engstrom & Salisbury, 2010). Ongoing professional development, support, and reflective practice are necessary to increase implementation of coaching practices (Friedman et al., 2012; Marturana & Woods, 2012; Salisbury et al., 2010), and when combined with training in cultural competence, they can enable practitioners to provide meaningful, comprehensive, and productive family intervention (Cambray-Engstrom & Salisbury, 2010).
Limitations of the Scoping Review
A potential limitation of this review was the exclusion of unpublished reports or government publications on coaching and occupational therapy, as well as any unpublished master’s theses or doctoral dissertations. We exclusively examined peer-reviewed published articles in an effort to gauge the existing established evidence on coaching practices in EI occupational therapy service provision. Nevertheless, valuable perspectives on the topic may have been missed as a result of this exclusion.
The search terms may have led to further limitations. We may have missed some articles because we did not have access to all potentially relevant databases. However, the 11 databases that were deemed most pertinent to occupational therapy were searched in an effort to minimize any potential oversight. Literature on coaching in occupational therapy with potential relevance to practice in the United States may have been published in other countries. The search process excluded articles that did not explicitly describe occupational therapy involvement in the study. Some relevant articles may have been excluded from review because of the tendency in the EI literature to refer simply to providers or interventionists without further specificity.
In addition, some generalizations made may not be specific to occupational therapy because many of the studies discussed used a multidisciplinary model of practice (of which occupational therapy was but one service) and therefore may not accurately depict the distinct role of the occupational therapist. Our exclusionary criteria limited the research to studies with children younger than age 3, therefore eliminating information regarding coaching in education or as used with older children, which may have provided relevant perspectives.
Future Research Directions
This review provides a glimpse at the available literature on EI service provider utilization of coaching strategies during intervention, which has predominantly explored provider perceptions and outcomes in relation to parent coaching. On the basis of study findings, future research should seek to demonstrate the impact of parent coaching on child outcomes (Campbell & Coletti, 2013; Marturana & Woods, 2012) as they relate to goals typical of an IFSP, to truly establish standards of best practice. In addition, future studies might seek to investigate the extent to which caregivers are using strategies taught by providers through coaching, as well as exploring which coaching strategies are appropriate for different interventions (Colyvas et al., 2010).
Occupational therapists are well positioned to engage in coaching practices because they examine the role of context and environment in the system as well as in the family. However, the literature does not reflect the role occupational therapists play in the delivery of parent coaching as an intervention approach, and more occupational therapy-specific research is warranted.
Implications for Occupational Therapy Practice
This scoping review has the following implications for occupational therapy practice: Caregiver coaching in EI has been shown to have a positive effect on parental self-efficacy and capability in attending to their children’s needs. Many EI practitioners remain apprehensive about and require training and ongoing professional development in coaching, inclusive of cultural competency training, in order to successfully implement it. The intended outcomes of parent coaching interventions (i.e., increased child participation, parental self-efficacy) need increased alignment with the goals, assessments, and outcome measures typically used in EI. The principles of caregiver coaching are well aligned with core components of the occupational therapy scope of practice, and occupational therapy practitioners in EI should demonstrate their involvement in the implementation of coaching practices through increased research on the topic.
Conclusion
This scoping review indicated that although EI practitioners are aware of coaching and report finding it a valuable approach to working with families, many remain apprehensive about its implementation due to preference for traditional approaches, lack of training in the application of coaching, and limited knowledge of cultural diversities. The results of this study indicate that there is no consensus on the definition of coaching; however, the concepts used when providing interventions based on coaching are relatively consistent. Coaching offers a promising avenue for practitioners in EI to collaborate with caregivers to ensure that they have the tools necessary to help their child acquire and maintain an active role in family life.
Supplemental Material
Supplementary material for Caregiver Coaching in Early Intervention: A Scoping Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.049143.pdf for Caregiver Coaching in Early Intervention: A Scoping Review by Francine M. Seruya, Emily Feit, Alexys Tirado, Diana Ottomanelli and Melissa Celio in The American Journal of Occupational Therapy
Footnotes
*
Indicates articles included in the scoping review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.