
Abstract
This is the first published study to highlight the feasibility of creating customized splints using 3D print technology for fragile neonates.
Neonates with a positional body deformity or joint contractures could experience long-term functional deficits. Deformities can be caused by a variety of problems, including, but not limited to, neuromuscular disorders, congenital defects, in utero or postnatal positioning, fracture, cerebral palsy, and central brain or peripheral nerve injury. Neonates born with congenital anomalies are vulnerable to complications that increase health problems in their pediatric years (Sukanya et al., 2021). In some cases, anatomical deformity and functional deficits can be progressive. Along with passive range-of-motion and stretching exercises (Anderson & Anderson, 1988), splinting may help prevent or reduce contractures, increase range of motion, maintain a resting position, and promote the functional capacity to participate in childhood occupations. Splinting is more likely to achieve correction if the process starts within a few weeks after birth (Verchere et al., 2014).
Although therapeutic exercise is preferred, splinting neonates in the neonatal intensive care unit (NICU) is vital. Anderson and Anderson (1988) made several observations about this. The time required by an occupational therapist to perform therapeutic exercise on neonates far exceeds staff availability in a large, busy NICU. Parents and staff can be trained but are not always available to provide therapeutic exercise at the necessary frequency and duration; neither can they master the appropriate therapeutic techniques. Nurses typically focus on more acute medical issues and care than on exercises and are often afraid to perform a range-of-motion exercise on fragile or deformed joints. Neonates’ unstable medical condition can limit tolerance of exercise and cause stress. Splinting can provide multiple hours of continuous stretch for contractures and promote a balance of asymmetric muscle tone. Splints can also protect weak muscles and joints, and serial molding may allow for constant improvements in functional positioning. Most splinting is done on an outpatient basis by specialized therapists. Neonates with deformities in need of splinting may miss the most beneficial window because of a prolonged NICU stay. Splinting without exercise can also be detrimental, but it can allow early intervention when therapeutic exercise is not possible or sufficient.
Fabricating a splint for neonates requires special considerations. Neonates are more prone to injuries of the nervous and musculoskeletal systems and pressure ulcers because of a lack of fat pads and fragile skin (Anderson & Anderson, 1988). Traditional splinting materials, such as plaster and thermoplastic sheet, are difficult to mold into a perfect fit and are heavily weighted; also, avoiding rough edges can be difficult. Traditional splints are also not cosmetically appealing, which may decrease parental compliance. Noncompliance with splint use can lead to a loss in positional gains made within a few months after splinting has stopped (Jackman et al., 2014).
Three-dimensional (3D) printing is an emerging and innovative technology that positively influences outcomes for many medical specialties (Dodziuk, 2016). It allows for the creation of 3D products from digital images to meet patient-specific needs in a cost-effective manner, making it ideal for pediatric use (Sukanya et al., 2021). In the field of occupational therapy, the use of 3D technology opens a realm of opportunity for ease and customization of cost- effective orthoses. It also creates endless possibilities for the development and creation of adaptive equipment. Research shows that using 3D printed orthoses has many advantages, including improved comfort and fit, proper ventilation, lightweight material, aesthetic features, customization, and greater wearing compliance (Ganesan et al., 2016). Other benefits include cost efficiency based on the materials used and a potential increase in the patient’s level of satisfaction (Choonara et al., 2016).
We describe three case reports in which we evaluate the feasibility of using 3D technology to fabricate customized splints for neonates. These case studies exemplify occupational therapists’ experience with and the challenges of 3D scanning, design, and printing splints.
Method
Setting
This study was conducted in a large academic NICU that is a major referral center for neighboring states for neonates with prenatally diagnosed complex congenital anomalies. A team of occupational therapists assessed and served the neonates in the NICU.
Participants
Neonates admitted to the NICU with body deformities or joint contractures receive ongoing, dynamic occupational therapy. Severe cases are considered for splinting and outpatient orthopedic referral. The three cases discussed here were chosen to have a 3D-printed splint on the basis of the potential benefit of early splinting.
Procedure
The Occupational Therapy Department at the University of Utah School of Medicine started using 3D printing approximately 4 yr ago. The technology was mainly used with the adult population. The printer used was the Fusion3 F410 3D Printer (Fusion3, Greensboro, NC), and the 3D scanner was the Artec Leo (Artec3D, Sana Clara, CA). The software programs used for the projects discussed in this article were Artec Studio (Artec3D, Santa Clara, CA), Meshmixer Version 3.5 for PC (Autodesk, Inc., San Rafael, CA), 3D CAD (Dessault Systèmes SolidWorks Corporation, Waltham, MA), and Simplify3D slicer software for PC (Version 4.1; Simplify3D, Cincinnati, OH). We use many different filaments, but acrylonitrile butadiene styrene (ABS) was used for the neonatal splints. Extensive knowledge of 3D modeling and computer-aided design (CAD) software is needed to complete the process.
Outcome
We monitored the neonates’ comfort while they were wearing the splints and documented any complications from the splints as well as clinical improvement.
Ethics Consideration
The University of Utah institutional review board did not consider this retrospective case report human subjects research. Written parental consents were obtained.
Results
Case 1: Patient K
Patient K was a male neonate born prematurely at 34 wk gestational age with multiple congenital anomalies, including congenital left-sided torticollis from cervical vertebral abnormalities, scoliosis, and an asymmetric mandible and ribs (Figure 1). Prematurity and obstructive urinary tract disease led to his prolonged NICU stay. There was a concern about oral skill development because of his asymmetric jawline, and he started to develop positional plagiocephaly. Therapeutic intervention included torticollis stretches, developmental positioning, and oral–motor activities. Tubular orthosis for torticollis is not recommended until age 4 mo (Gundrathi et al., 2020) because of concerns about airway compression and other safety issues.
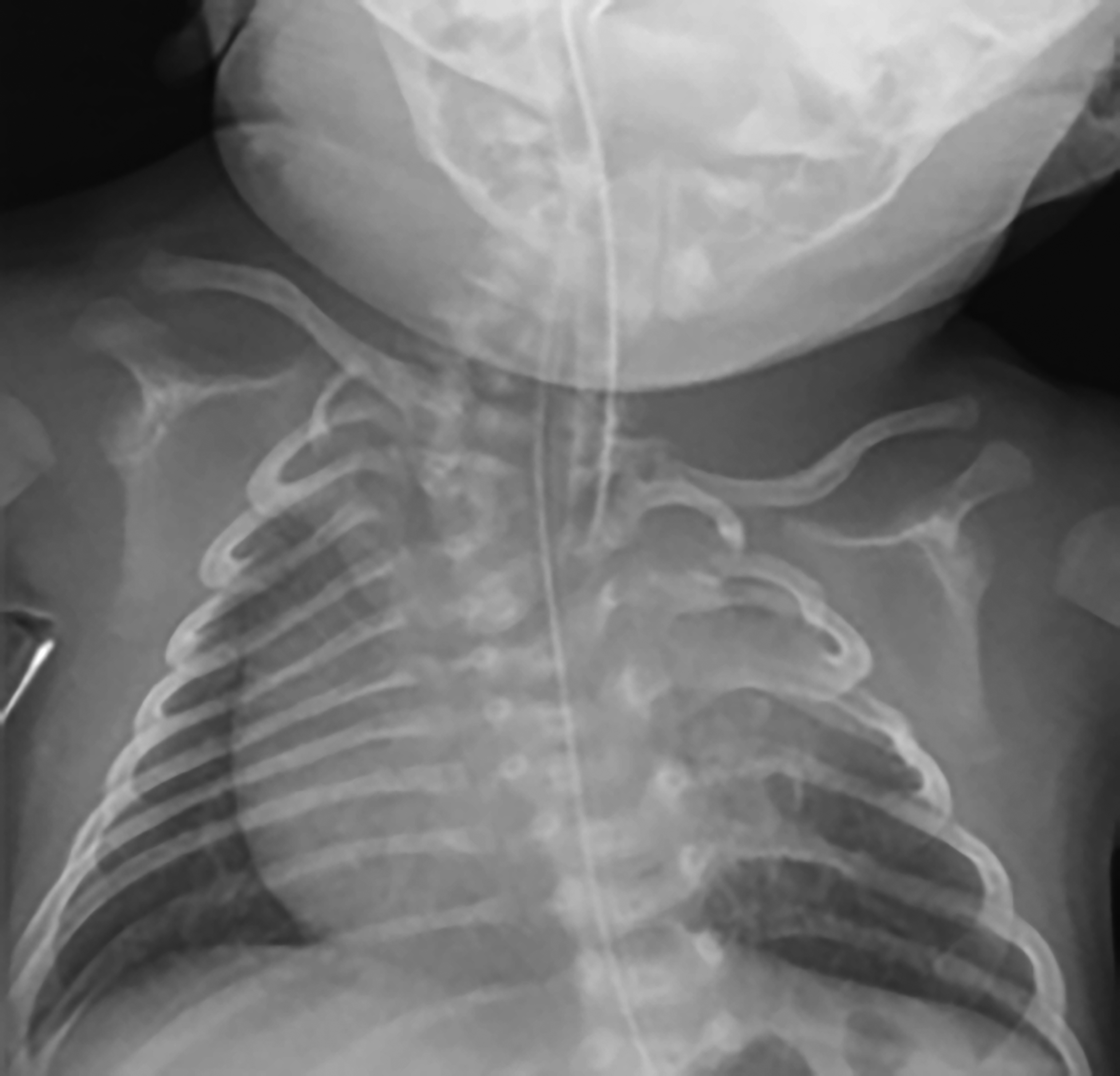
X-ray image of Patient K.
Patient K’s prolonged NICU stay raised concerns regarding a prolonged and untreated abnormal neck position that could affect visual development, feeding skills, and balance as gross motor development progressed. Worsening plagiocephaly could also lead to notable head shape deformity requiring helmet orthosis. Splinting was necessary to provide prolonged stretch and inhibition of preferred position during sleep to prevent further complications and increase functional capacity. The use of this splint during sleep was appropriate only in the NICU setting and was determined safe because he was on continuous cardiopulmonary monitoring and in line of nursing sight 24 hr/day. For this splint, a 3D scan was taken of Patient K in a side-lying position with an occupational therapist holding the head and shoulder in the desired position. After scanning, the digital file was imported into a 3D modeling software program. The digital images were manipulated, smoothed, and then used as a template for the custom splint (Figure 2, Panels A–D).
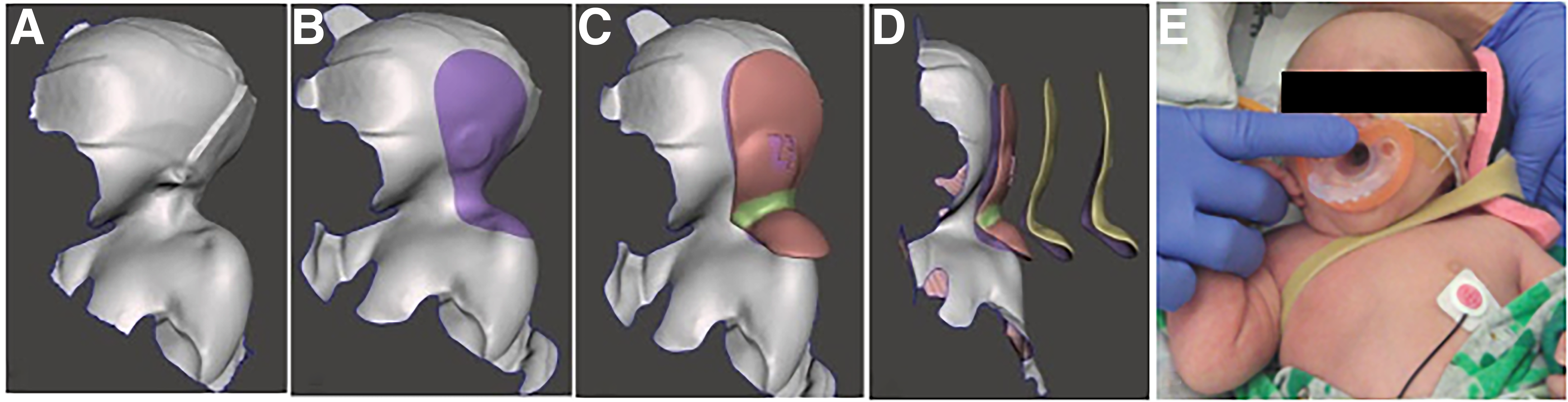
Progression of designing a custom splint from a 3D-scanned digital image.
Once the splint’s desired shape and location were established, we added space between the splint and skin to accommodate padding that would be applied after printing to protect the skin. Also, because of his orthopedic anomalies, Patient K had a very prominent acromioclavicular joint that was visible on the scan. A bump-out for extra space was designed into the splint to allow extra padding and protection to avoid skin ulcers. A second bump-out was designed around his ear to prevent extreme pressures on the ear but still allow needed surface area on his head to hold the desired position.
The end product was an
Case 2: Patient L
Patient L was a male neonate who was born prematurely at 36 wk gestational age with chromosomal abnormalities. Brain structural anomalies led to decreased extremity movement and hypertonia, which occurred in utero. His left upper extremity showed considerable wrist flexion, excessive metacarpophalangeal extension, and tight proximal interphalangeal joint flexion. His right upper extremity showed wrist extension and tight flexion of all phalanges (Figure 3). The therapeutic goal was to increase range of motion to support functional fine motor skill development, such as holding onto a pacifier, grasping, and sucking on fingers for self-coping. An earlier meta-analysis showed that hand splints with adjunct therapy are better than therapy alone (Jackman et al., 2014). Range-of-motion exercise was completed daily by therapists and parents, with minimal progress noted, indicating the need for a prolonged stretch with splinting.

Patient L’s hand deformities.
After many failed attempts at using commercially available and handmade soft splints, our team decided to use 3D technology to make customized hand splints. Various sizes of cylindrical objects were trialed to find the ideal size needed to promote optimal resting hand position. We measured the hands and forearms and then designed the splints using CAD software from those measurements. The first design involved a cylindrical shape of uniform size attached to a forearm support. When tried on Patient L, the size of the cylinder was too large. He could escape the splint because his fingers did not fully wrap around the cylinder, and the fourth and fifth digits escaped entirely, with transitions in behavioral state affecting muscle tone. Changes were made in the CAD software for the next splint version. The revised splint had a smaller conical shape that tapered down in size toward the fourth and fifth digits (Figure 4, Panel A). Now his digits could fully wrap around the cylinder and remain in place when he became upset, and tone increased. Long-term outcome assessment was limited after Patient L was transferred to an outside hospital.
The splint design required approximately 1.5 hr, including brainstorming, taking measurements, and designing the splint with the CAD software. ABS filament material was used. The total cost of the filament needed for the hand splints was approximately $0.50 each. Printing took about 25 min. The splint was covered in 1/8-in. foam padding for comfort and secured using hook-and-loop strapping at the wrist and around the fingers (Figure 4, Panels B and C).
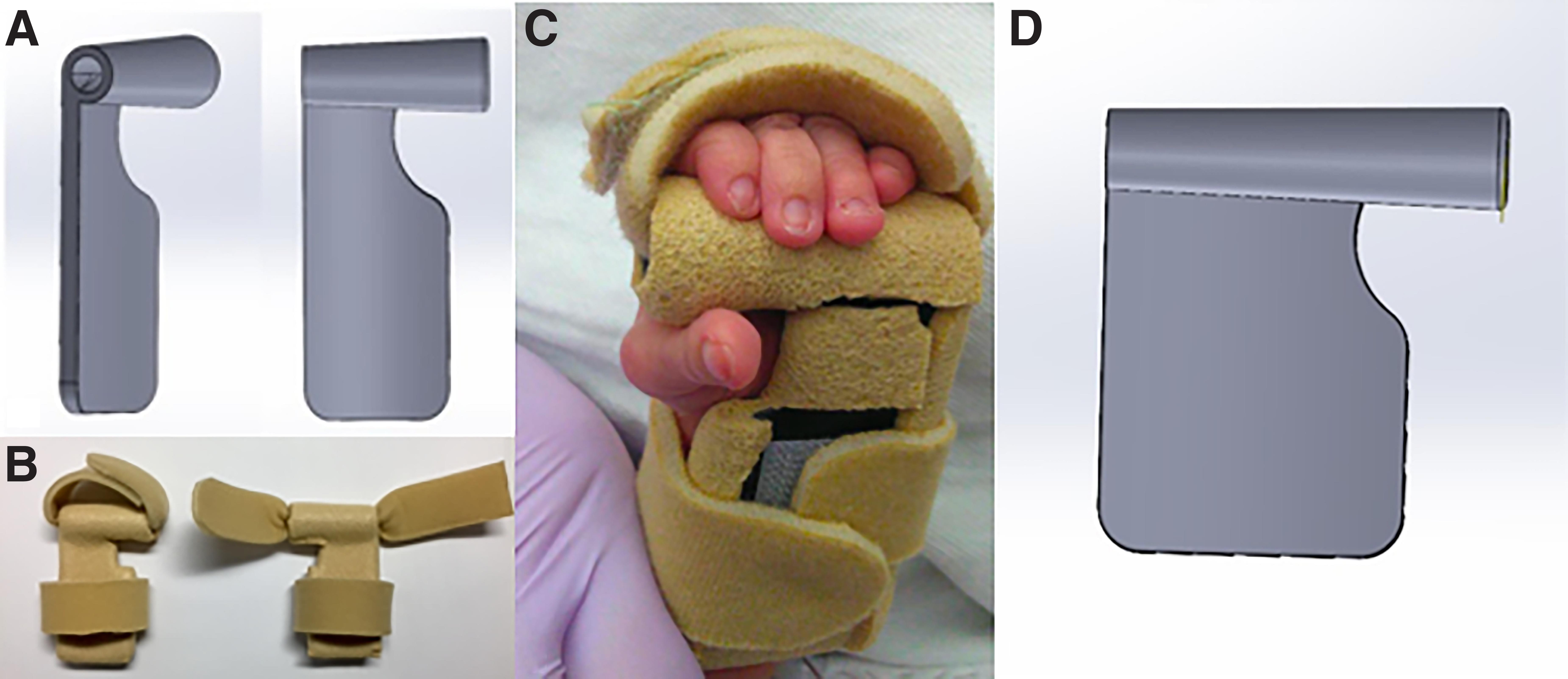
Hand splints built with computer-assisted design software and final splints.
Case 3: Patient H
Patient H was a term male neonate with skeletal dysplasia, a flat nasal bridge, a cleft palate, and micrognathia. A skeletal survey showed slightly shortened long bones of the extremities. The metaphyses were broadening with prominent spurs along the edges. The left hand was fisted, with digits 3 and 4 tightly flexed inside the palm. Splinting was indicated because of the potential for skin breakdown in the palm and to prevent further contractures. We used the digital hand splint design that was made for Patient L as a blueprint for this case. The size and contours were digitally adjusted on the basis of Patient H’s hand measurements. Measurements were taken of the wrist circumference for width, from the fifth digit proximal interphalangeal to the mid-forearm for length, and from the head of the second metacarpal to the head of the fifth metacarpal for hand width. With the previously designed splint in a CAD program, we were able to input these new measurements, and the software adjusted the splint size accordingly (Figure 4, Panel D). The time to make this splint was significantly shorter and required approximately 2 min for measurements of Patient H, 15 min to change measurements in the CAD program, and 30 min to print. The cost was the same as the previous hand splint in Case 2. The splint fit well and was worn on a schedule according to infant care times, alternating 3 hr on and 3 hr off. Patient H had improved active movement and full range of motion in all digits, so the splint was discontinued after 20 days with continued monitoring for regression and range-of-motion exercises performed by the parents.
Discussion
We have discussed three cases of using 3D printing technology to make splints and have shown the feasibility of applying 3D technology to treatment of neonates in a NICU. To our knowledge, this is the first publication to discuss this use of such technology.
Advanced 3D technology can print perfectly contoured splints that are created from the neonate’s scanned body parts. There is a potential for improved outcomes with custom-fitted orthoses (Sukanya et al., 2021). 3D splints are made of lightweight plastic that can be customized with different textures, thicknesses, and strength according to the neonate’s needs. Using 3D scanning in this setting has several advantages. 3D scanning makes exact digital imprints of the anatomy, allowing bony prominences and other areas of concern to be seen and taken into consideration during the design process; also, the fit can be seen virtually before it is physically applied. Handling of the neonate is minimal and required only briefly for positioning during the scan, as opposed to repeated trials and adjustments that require handling the neonate multiple times with traditional splinting. Splints have traditionally been created by applying an imprinting mold directly on the neonate’s fragile skin, and thermoplastic material requires heating. The use of 3D scanning and design allows for customized splints but eliminates direct contact of multiple materials with the fragile skin that occurs during the traditional splint fabrication process.
Splints used by neonates are often soiled, and materials used for the 3D splints allow for easy cleaning, especially in the NICU setting. Multiple backup splints can be replicated in a short amount of time. Special designs can also be made to fit the therapeutic need and for proper skin ventilation. Designing tubular edges into the splint makes possible rounded edges that prevent skin abrasion (Li & Tanaka, 2018). The 3D printed splint can be made in various colors, with added logos or names, making it more cosmetically pleasing, which may improve parental compliance and satisfaction.
Limitations
Although neonatal 3D-printed splinting is feasible, we have described only three customized cases. Widespread implementation of 3D technology for splinting neonates remains challenging for various reasons.
Obtaining an accurate and high-quality scanned image of the body part is necessary to customize and create a perfect fit. Neonates cannot voluntarily hold their body or hand in a certain position during scanning, thus requiring another person to assist with the positioning. The hands of the assistant may cover the anatomical features of the neonate; therefore, for example, Patient L’s hand splints were designed from measurements rather than a direct 3D scan. Motion during a scan also affects image quality. The shadow or wrinkle of small body parts, such as fingers, that the scanning light beam cannot reach will diminish image accuracy (Li & Tanaka, 2018). Postscan modification with advanced 3D software and specialized programming skills may improve image quality (Li & Tanaka, 2018).
At present, only limited resources are available specific to splint design. 3D printing of a large complex splint can take hours (Li & Tanaka, 2018), but printing small splints for neonates takes only 1 hr, 25 min.
Last, although the cost of 3D printing material is low, the initial cost of the scanner, software, and printer is a significant investment. As technology improves, we are hoping for lower costs and more user-friendly programming. Our study was limited by a small sample size and a short study duration. We are unable to generalize the findings to all populations.
Future Research
We have discussed the use of 3D printing only in relation to neck and hand splints. 3D printing can advance medical care and improve patient function for long-term development and participation in occupations. Commercial companies have used 3D technology to create custom-made helmet orthoses to treat positional plagiocephaly (Geoffroy et al., 2018; Leszczynski, 2017). 3D printed airway splints for neonates have proven to be life saving and continue to be researched (Fessenden, 2013; Les et al., 2019). Applying 3D printing technology to neonatal and pediatric care could provide more precise interventions and a better quality of life (Sukanya et al., 2021). More studies are needed to improve technology and ensure safety.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: ▪ 3D technology has the potential to provide novel options for occupational therapy practice in the NICU. ▪ Applying 3D printing technology to neonatal occupational therapy could provide more precise orthoses, earlier intervention, and thus a better quality of life throughout critical developmental milestones. ▪ At present, 3D technology requires advanced software design skills, which limits widespread application.
Conclusion
We have demonstrated the feasibility of using 3D technology to fabricate customized splints for three neonates. Further research and multidisciplinary collaborations are needed to identify eligible neonates, monitor safety, evaluate outcomes, and develop more user-friendly 3D technology to expand the implementation of neonatal 3D-printed splints.
Footnotes
Acknowledgments
We thank Director of Acute Rehabilitation Chris Noren for all of his support. We also thank the families for their participation in this novel approach.