
Abstract
This study highlights positive patient outcomes in measuring instrumental activities of daily living (IADL) skills over time after participation in occupation-based group programs.
A goal of inpatient rehabilitation is to improve the function of patients with an impairment, participation restriction, or activity limitation resulting from a health condition (American Academy of Physical Medicine and Rehabilitation, 2012). For occupational therapists, this entails addressing health, well-being, and participation through engagement in occupations (American Occupational Therapy Association [AOTA], 2020). Occupational therapists use occupation-based practice to address individual function, with occupation as the therapeutic agent of change (Fisher, 2014; Gray, 1998). Research has demonstrated the effectiveness of occupation-based interventions in rehabilitation settings to improve health outcomes (Ciro et al., 2014; Dikmen et al., 2003; Hackett et al., 2000; Pellegrini et al., 2018; Pillastrini et al., 2008). A randomized controlled trial by Skubik-Peplaski et al. (2017) used occupation-based interventions and repetitive task practice to investigate occupational performance recovery among stroke survivors. Their results demonstrated that occupation-based interventions were equally as effective as repetitive task practice, and they noted that patients who directed their intervention enhanced their involvement and outcomes.
Groups enable practitioners to enhance the amount and intensity of intervention, and they are used in rehabilitation settings to provide more scheduled therapy time and enhance outcomes. Previous research has focused on structured, scheduled impairment-based therapy such as group circuit classes to improve functional outcomes of walking ability, arm function, and quality of life (Lohse et al., 2014; Schneider et al., 2016; Veerbeek et al., 2014). A recent scoping review (Spalding et al., 2020) found that little research has explored the impact of occupation-based groups on patient outcomes, with the literature focusing on group formation and delivery. Complex occupations such as home management and community living are often addressed; however, the impact on outcomes requires further exploration (Spalding et al., 2020).
Occupation-based groups can enable more opportunities to practice, and understanding the impact that these groups have on participation and engagement in occupation beyond the group setting is required. The first aim of this study was to investigate the effect of an occupation-based group on patient outcomes of goal achievement and performance of, satisfaction with, and self-efficacy in instrumental activities of daily living (IADL) skills by measuring whether (1) a change in scores occurs from preintervention to postintervention and (2) the change is maintained from postintervention to 30-day and 90-day follow-ups. The second aim was to investigate whether age or diagnosis had an influence on patient outcomes postintervention.
Method
This cohort study with longitudinal follow-up and within-group comparisons was approved by the Griffith University (Ref. No. 2019/498) and Royal Brisbane and Women’s Hospital (LNR/2019/QRBW/53152) human research ethics committees.
Setting
The occupation-based LifeSkills group operates in the general rehabilitation ward of a large metropolitan hospital (Royal Brisbane and Women’s Hospital, Brisbane, Queensland, Australia). The LifeSkills group focuses on repetitive practice of occupations to enhance overall performance of preferred IADLs. The group was developed using an evidence-based framework. Guiding principles include collaborative goal setting, in which the use of patient-centered goals is correlated with higher occupational performance and achievement (Radomski, 2002); engagement in meaningful and purposeful occupations to improve participation, motivation, and overall skill acquisition (Trombly, 1995); frequency and intensity of practice to improve neural plasticity (Kleim & Jones, 2008); and motor learning with a focus on using the stages of learning, type of task, and feedback to influence motor recovery (Muratori et al., 2013). The group runs for 60 min 4 days per week and is led by occupational therapy students under the guidance of the treating therapist.
Participants
Consecutive sampling was used to recruit participants from among the patients referred to the LifeSkills group. Inclusion criteria were as follows: adult (age >18 yr); English speaking (because of the lack of an interpretation service); planned discharge to home; ability to identify up to five goal areas related to IADLs; and ability to work under the semisupervised conditions required for group process implementation. Participants were excluded from the study if their planned discharge destination was a residential care facility. A minimum sample size of 30 participants was sought, consistent with those of previous studies using similar methodology and outcome measures (Doig et al., 2010; Schindler, 2010).
Measures
The demographic data collected included age, gender, diagnosis, rehabilitation length of stay, living arrangement, and use of supportive service.
The Canadian Occupational Performance Measure (COPM; Law et al., 2019) was used to measure the participants’ self-perceived performance of and satisfaction with their IADL occupations. The COPM has been used across the lifespan of people with a variety of disabilities, including stroke, dementia, and traumatic brain injury (Doig et al., 2010; Enemark Larsen & Carlsson, 2012; McColl et al., 2000). A change of ≥2 points is considered clinically significant (Law et al., 2019; McColl et al., 2000), and total COPM Performance and Satisfaction subscale scores were obtained by dividing the sum of the Performance or Satisfaction score by the number of goals.
Goal Attainment Scaling (GAS; Rockwood et al., 2003) is a therapist-rated, objective outcome measure of participants’ performance that is sensitive to change in general rehabilitation. GAS is based on participants’ COPM goals, and an ordinal measure is used to break each COPM goal into five possible scenarios: much less than expected (−2), somewhat less than expected (−1), expected (0), somewhat more than expected (1), and much more than expected (2). The GAS total score, or GAS T score, has a M of 50 and a SD of 10 and can be calculated using a formula described by Kiresuk et al. (1994). T scores of 50 indicate expected levels of performance, and T scores above and below 50 indicate higher and lower than expected levels of performance, respectively. Researchers have successfully used GAS in combination with the COPM to measure clinical change in adults with traumatic brain injury and dementia (Ciro et al., 2014; Doig et al., 2010).
The Lawton IADL scale is used to assess a person’s ability to perform IADLs, such as using the telephone, shopping, preparing food, housekeeping, or doing laundry (Lawton & Brody, 1969). The scale contains eight items with a summary score that ranges from 0 (low function) to 8 (high function). Each item is rated dichotomously (0 = less able, 1 = more able). The higher the summary score, the greater the person’s abilities. It is a moderately strong predictor of functioning of older adults (Vittengl et al., 2006)
A validated self-efficacy measure specific enough for the purposes of this study was lacking. Building on current literature (Gage et al., 1994), the research team developed a self-efficacy scale of IADL skills. This Likert-type rating scale ranged from 1 (not confident) to 5 (very confident), was patient specific, and was used to examine participants’ confidence in performing the IADL occupations identified with the COPM.
Procedure
Figure 1 illustrates the full study procedure. All patients referred to the LifeSkills group were screened against the inclusion criteria. If eligible, the participant information and consent form was provided and discussed, and patients were given 24 hr to consider participating. It was made explicitly clear that involvement in any aspect of the study would have no direct benefit to the clinical care provided. All data collection was conducted by the principal investigator (Kaitlyn Spalding), who was not involved in direct clinical treatment of participants.
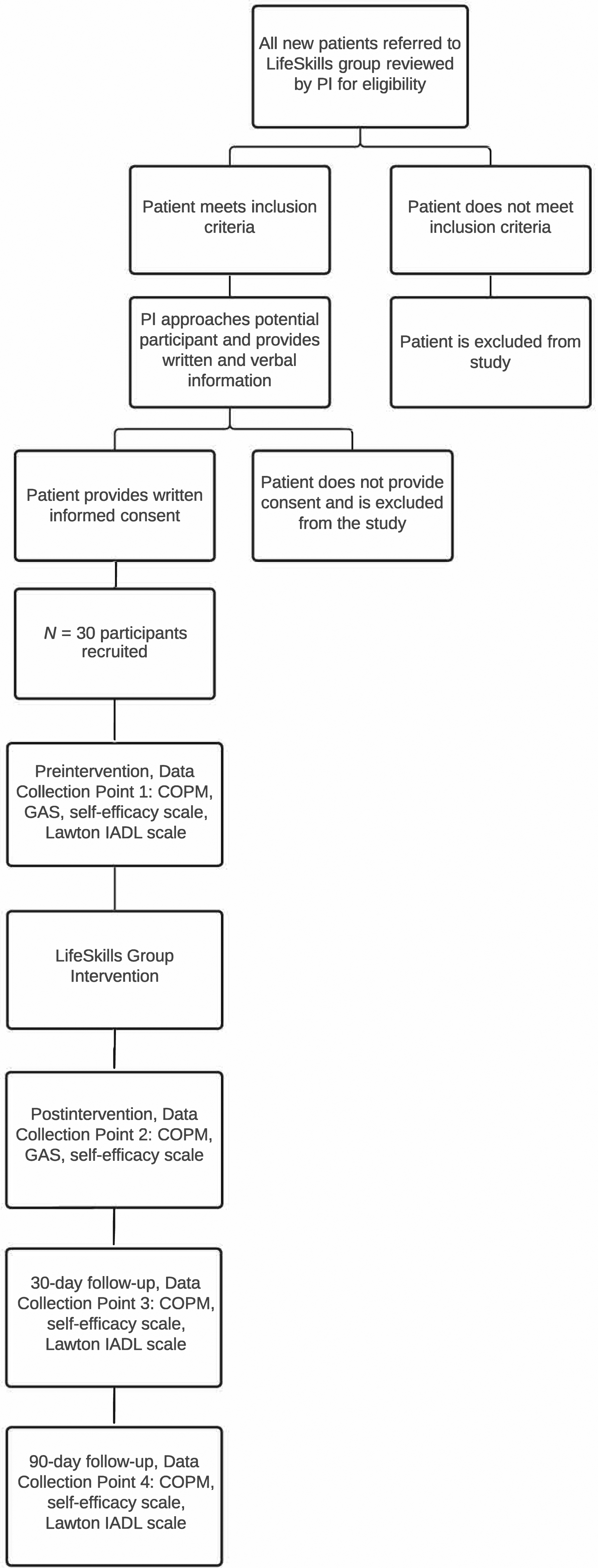
Study procedure.
The participants identified up to five IADL goals using the COPM and rated their performance and satisfaction; potential outcomes on the GAS were derived as per Ottenbacher and Cusick (1990). The self-efficacy scale was used to rate participants’ current confidence in performing the identified IADL goals. The Lawton IADL scale was used to rate prehospitalization performance. Participation in the LifeSkills group was tailored to participants’ identified goals. The COPM, GAS, and self-efficacy scale were readministered immediately postintervention. Participants were telephoned by the principal investigator at 30 days and 90 days postdischarge for follow-up data collection.
Data Analysis
IBM SPSS Statistics (Version 27) was used for data analysis. A significance level of α = .05 was set for all analyses, according to conventional statistics procedures. Descriptive statistics summarized demographic information and calculated total change scale scores for outcome measures from pre- to postintervention, postintervention to 30-day follow-up, and postintervention to 90-day follow-up. Change scores for the Lawton IADL scale were analyzed from preintervention to 30-day follow-up and preintervention to 90-day follow-up. Before analysis, the normality of distributions was reviewed using quantile–quantile plots and histograms. Data were negatively skewed and could not be corrected; therefore, a related-samples Wilcoxon signed-rank test was used to examine sensitivity to change across all data points. An independent-samples Mann–Whitney U test was used to determine differences in scores between key demographic characteristics of diagnosis (neurological and non-neurological) and age (<65 yr and >65 yr) for the COPM, GAS, and self-efficacy scale. The 5 participants with missing data at the 30-day and 90-day follow-ups were comparable to the other participants at baseline and were considered missing at random.
Results
Demographic and Group Intervention Data
Data were collected from February 2020 to February 2021. All potential participants (N = 31) agreed to participate in the study. One participant dropped out before the intervention because of illness and was not included in overall data analysis. The participants were 21 women and 9 men ages 35 to 91 yr (M = 68.87 yr, SD = 14.78), with a mean length of rehabilitation stay of 32.03 days (SD = 16.74). A total of 85 occupation-based IADL tasks were practiced: meal preparation (n = 31), laundry (n = 24), shopping (n = 8), dish washing (n = 5), making the bed (n = 4), household cleaning (n = 4), computer use (n = 4), community access (n = 4), and medication management (n = 1). The average number of group sessions attended was 5.97 (SD = 3.81), and the average number of tasks practiced in each session was 3.5 (SD = 1.2). Additional demographic characteristics are provided in Table 1.
Participant Demographics
Note. N = 30.
n = 25.
Change Scores Pre- and Postintervention
Participants had a statistically significant increase in COPM Performance, COPM Satisfaction, GAS T, and self-efficacy scores after group attendance (Table 2). The change scores for the COPM were above the minimal clinically important difference (MCID) of 2 points (Law et al., 2019; McColl et al., 2000)—in specific, 53.3% met or exceeded the MCID for COPM Performance and 70.0% met or exceeded MCID for COPM Satisfaction. For the GAS, a median T score of 50.00 at discharge indicated the expected level of performance.
Pre- and Postintervention Group Median Scores on the COPM, GAS T, and Self-Efficacy Scale
Note. All z scores significantly different at p < .05. COPM = Canadian Occupational Performance Measure; GAS T score = Goal Attainment Scaling total score; IQR = interquartile range; Mdn = median.
Outcomes at 30-Day and 90-Day Follow-Ups
Participants showed an increase in COPM Performance, COPM Satisfaction, and self-efficacy scale median scores at the 30-day follow-up; however, this increase was not statistically significant. At the 90-day follow-up, there was a statistically significant increase in COPM Performance and self-efficacy scale scores compared with postintervention (Table 3). Lawton IADL scale scores before hospitalization (Mdn = 8, interquartile range [IQR] = 1) were significantly higher than the median of 6 (IQR = 3) reported at both 30-day (p < .001) and 90-day (p = .002) follow-ups.
Comparison of Group Median Scores on COPM and Self-Efficacy Between Postintervention and 30-Day and 90-Day Follow-Ups
Note. COPM = Canadian Occupational Performance Measure; IQR = interquartile range; Mdn = median.
Significant difference at p < .05.
Outcomes Based on Age and Diagnostic Group
Participants with neurological and non-neurological conditions had no significant differences in outcomes on the COPM Performance (U = 99.5, z = −.521, p = .608) and Satisfaction (U = 118.5, z = .271, p = .790) subscales, GAS (U = 114.5, z = .104, p = .918), and self-efficacy scale (U = 125, z = .557, p = .608) after group attendance.
Participants younger than age 65 yr and those older than age 65 yr had no significant differences in outcomes on the COPM Performance (U = 107, z = .108, p = .933) and Satisfaction (U = 91.5, z = −.561, p = .582) subscales, GAS (U = 84.5, z = −.861, p = .395), and self-efficacy scale (U = 84.5, z = −.887, p = .395) after group attendance.
Discussion
Occupation-based groups occur in rehabilitation practice; however, the literature has primarily reported on group design, process outcomes, and participant experiences (Spalding et al., 2020). The objectives of this study were to go further and examine patient outcomes. The findings indicate that the LifeSkills group supports goal achievement in chosen IADLs, and this achievement is maintained at follow-up. A clinically significant change of 2 points or more on the COPM at all timepoints and a GAS T score of 50, the expected level of performance, at postintervention are compelling indicators of the effect of this group intervention in the clinical setting.
A multidisciplinary approach to rehabilitation can have beneficial patient outcomes, and these outcomes are often achieved with one-to-one therapy. Previous mapping of occupational therapy in inpatient rehabilitation has identified that more time is spent in prefunctional one-to-one therapy than in functional activities (Ballinger et al., 1999; Gustafsson et al., 2012; Latham et al., 2006; Richards et al., 2005; Smallfield & Karges, 2009). Reflecting changes in occupational therapy practice (AOTA, 2020), the group intervention in this study focused on occupation with due consideration of personal and environmental contexts. The results support that contemporary occupational therapy for IADLs in a group setting can achieve positive outcomes.
The outcomes of this study may also have positive impacts on organizational resourcing. In a scoping review by Spalding et al. (2020), increased access to activity for therapeutic and economic values was a common reason for using occupation-based groups; however, only one study has formally evaluated cost-effectiveness. Cost savings with no effect on outcome effectiveness have been demonstrated in balance, cardiac rehabilitation, and fatigue management group programs (Shields et al., 2018; Thomas et al., 2013; Treacy et al., 2018). Occupation-based groups may be cost-effective, and further research to establish this effectiveness is required.
Participants demonstrated different trajectories for IADL outcomes on the COPM and Lawton IADL scale. First, participants’ scores on the Lawton IADL scale decreased from preintervention to postintervention follow-ups. This widely used measure includes scores for community-based IADLs such as transport and shopping, goals that were less prevalent in the LifeSkills group. Although we did not directly explore community participation, the follow-up points aligned with coronavirus disease 2019 restrictions, which reduced participants’ movements within the community and perhaps led to increased use of external supports.
The Lawton IADL scale is also a high-level scale; although participants may consider themselves independent, they may score low on some questions. For example, for food preparation, a person can only score a 1 if the meal is planned, prepared, and served independently. A score of 0 is received if the person is supplied with ingredients or heats up a prepared meal. Using a microwave oven to prepare a meal was a common goal identified by study participants, and a higher score on GAS or the COPM may have been recorded. Alternatively, the findings may indicate a reduced sensitivity of general measures such as the Lawton IADL scale to changes indicated by individualized COPM, GAS, and self-efficacy scale scores. This is consistent with the results of previous research that measured confidence in skills with a general measure, the Self-Efficacy Gauge (SEG; Gustafsson & McKenna, 2010), and reported low scores at follow-up, in contrast to the increased self-efficacy ratings in this study. These collective findings highlight the importance of using person-centered measures to demonstrate change and improvement rather than general measures such as the SEG and Lawton IADL scale.
Understanding whether patient-related factors have an impact on outcomes is critical so that therapists can tailor interventions accordingly. In geriatric rehabilitation, variables such as age, premorbid function, mobility, and cognition have been shown to have an impact on functional improvement (Calle et al., 2018). The literature on occupation-based interventions has commonly focused on reporting patient outcomes specific to diagnosis, such as traumatic brain injury (Powell et al., 2016), psychiatric diagnoses (Schindler, 2010), and stroke (Wolf et al., 2015). It is encouraging that people in different diagnosis and age groups benefited equally from the occupation-based group reported on in this study, suggesting that clinicians could consider this occupation-based group a useful tool when creating a therapy program, especially in a general rehabilitation population.
Future Research Directions
The literature to date has attributed positive experiences of group programs to the patient-centered, goal-focused nature of the group design (Patterson et al., 2017). Further exploration of active components and causal mechanisms would be beneficial to understand for whom, why, and how this occupation-based group works. These findings may also form a platform for future larger scale rigorous studies examining economic value and cause–effect relationships and assessing the generalizability of the intervention’s effectiveness across varied inpatient rehabilitation settings.
Limitations
These results should be viewed cautiously given the uncontrolled, nonrandomized design. Without a control group, it is difficult to draw any conclusions about the specific benefits of the program, and therefore only descriptive benefits can be reported. A heterogeneous sample can also bring limitations to outcomes research, and average scores may not adequately express the complexity of rehabilitation populations. We acknowledge the impact of a small sample size while noting that previous studies using similar methodology and measures (Doig et al., 2010; Schindler, 2010) have demonstrated clinically relevant outcomes.
Implications for Occupational Therapy Practice
It is important for occupational therapists to embrace evidence-based practice. This study has the following implications for occupational therapy practice: Occupation-based groups facilitate goal achievement and improve self-reported performance of and satisfaction with IADL skills at discharge, irrespective of diagnosis or age, providing a resource option for addressing skills retraining in a general rehabilitation population. An occupation-based group intervention could be an alternative to providing the same intervention one-to-one. Consideration should be taken to using individualized measures to capture the impact of an intervention.
Conclusion
The LifeSkills group resulted in significant improvement in goal achievement, occupational performance, satisfaction, and self-efficacy at hospital discharge, and this improvement was maintained over time. With no significant differences found between participants on diagnosis and age, these findings indicate that an occupation-based group program has promising application in a general inpatient rehabilitation practice. One of the goals of inpatient rehabilitation is to improve occupational performance, so occupational therapists may find using an occupation-based group to be a valuable therapeutic option.
Footnotes
Acknowledgments
This work was supported by the Royal Brisbane and Women’s Hospital (RBWH) Research Scholarship. We acknowledge the RBWH occupational therapists and student occupational therapists who delivered the group program.