
Abstract
The results of this study can help clinicians identify, assess, and monitor daily activities, performance skills, and symptoms of children and adolescents with heritable disorders of connective tissue (HDCTs) to promote their participation in all aspects of daily life.
Heritable disorders of connective tissue (HDCTs) are a rare and heterogeneous group of disorders with a prevalence of up to 22 per 10,000 (Demmler et al., 2019; Mueller et al., 2016, 2018). Diagnoses include the following: ▪ Hypermobile Ehlers–Danlos syndrome (hEDS) and hypermobility spectrum disorder (HSD), both formerly classified as joint hypermobility syndrome (JHS) or Ehlers–Danlos syndrome– hypermobility type (EDS–HT); ▪ Osteogenesis imperfecta (OI); ▪ Marfan syndrome (MFS); and ▪ Loeys–Dietz syndrome (LDS; Castori & Hakim, 2017; Tofts et al., 2009).
HDCTs are complex conditions characterized by tissue fragility, including bone fragility, skin elasticity, and cardiovascular issues (Tofts et al., 2009). In particular, generalized joint hypermobility (GJH) is a common manifestation (Castori & Hakim, 2017); features of generalized joint hypermobility result in variable phenotypical presentations including musculoskeletal pain, fatigue, and joint instability (Castori & Hakim, 2017; Tofts et al., 2009). Regardless of diagnosis, signs and symptoms begin in early childhood, and parents report negative impacts of symptomatic GJH on their child’s daily life and academic and recreational activities (Pacey et al., 2015; Wesley et al., 2021).
Parents (Wesley et al., 2021) and clinicians (Adib et al., 2005; Pacey et al., 2015) have reported difficulties with hand function associated with GJH in children and adolescents with HDCTs. The impact of GJH-related performance skills and musculoskeletal features on hand function and daily activities for this population is unclear. Adults with hEDS and HSD have reported that hand pain and joint instability significantly affect their ability to carry out daily tasks (Stanitski et al., 2000) and are the primary reason for seeking specialized musculoskeletal care (Connelly et al., 2015).
Poor hand function can delay independence in daily activities, including school performance (McHale & Cermak, 1992; Rosenblum & Gafni-Lachter, 2015), leading to reliance on others in childhood and beyond (Chien et al., 2014, Pehoski et al., 1997). Despite parents’ concerns, however, little research has explored the impact of hand dysfunction, upper limb hypermobility, pain, and fatigue on children with HDCTs (Wesley et al., 2021). Such knowledge can guide the selection of outcome measures and inform interventions for this group. The primary aim of this study was to describe hand impairments and function in children and adolescents with HDCTs and to determine associations with their own perceptions of their hand function in activities of daily living. The secondary aim was to determine the extent to which hand impairment and function explain the variation in self-reported performance for this cohort.
Method
We used a cross-sectional design in this study. We obtained ethics approval (HREC LNR/16/SCHN/450) and written consent and verbal assent from participants and their parents.
Participants
We recruited participants ages 8–18 yr who had a medical diagnosis of osteogenesis imperfecta or Ehlers–Danlos syndrome–hypermobility type from an HDCT specialist clinic at a tertiary pediatric service in Sydney, Australia. Children with phenotypically identical EDS–HT and JHS (Castori et al., 2014) all exhibited GJH meeting the age- and gender-specific Beighton score criterion (≥4/9 for boys and ≥5/9 for girls) established for an Australian population (Singh et al., 2017). At the time of data collection, these children had not yet been reclassified with HSD or hEDS (Malfait et al., 2017).
Excluded were children who could not speak English or were unable to follow assessment instructions, those previously diagnosed with EDS–HT or JHS whose Beighton scores no longer met the Australian normative cutoffs (Singh et al., 2017), and those with comorbidities such as juvenile idiopathic arthritis, cerebral palsy, neuromusculoskeletal disorders, or moderate to severe developmental disability that would confound the effect of their HDCT on hand function.
Procedures
The first author (Alison Wesley), an occupational therapist experienced in administering and interpreting assessments for this diagnostic cohort, collected participants’ demographic, diagnostic, and anthropometric data and patient-reported HDCT-related symptoms. She measured GJH using the revised Beighton score (Juul-Kristensen et al., 2007) and the Upper Limb Hypermobility Assessment Tool (ULHAT; Nicholson & Chan, 2018) and performed a hand function assessment for each participant. She followed established protocols for all assessments. Assessments took place during one 1 1/2-hr session to ensure consistency across participants. A break was provided between each assessment task to minimize the risk of fatigue and permit monitoring for increased pain.
Performance and patient-reported outcome measures included grip strength and lateral and tip pinch using a CITEC handheld dynamometer (CITEC, Arnhem, The Netherlands), the Functional Dexterity Test (FDT; Gogola et al., 2013), the Nine-Hole Peg Test (9-HPT; Poole et al., 2005), the fine motor components of the Bruininks–Oseretsky Test of Motor Proficiency (BOT–2; Bruininks & Bruininks, 2005), the button test from the second edition of the Peabody Developmental Motor Scales (Folio & Fewell, 2000), and the 3-min Handwriting Speed Test (HST; Wallen et al., 1996). Writing endurance was assessed using a 9-min writing task based on the HST (O’Mahony et al., 2008), and pain and fatigue levels were collected using a visual analog scale (VAS) before and after the button and handwriting tests. Self-reported functional performance was measured using the Childhood Health Assessment Questionnaire (CHAQ–38); item scores range from 0 (without difficulty) to 3 (unable, not applicable; Lam et al., 2004). We report Dressing and Grooming (Items 1–4), Eating (Items 7–9), and Grip (Items 21–25) domains separately to describe more specific hand function–related limitations (Hoeksma et al., 2014). See Table A.1 in the Supplemental Appendix, which is available online at https://research.aota.org/ajot, for more detailed descriptions of outcome measures and administration.
Participants’ Physical Characteristics
Note. BMI = body mass index; ULHAT = Upper Limb Hypermobility Assessment Tool.
α = .05; observed power >.80 indicates sufficient sample size to achieve significance (Portney & Watkins, 2009).
Moderate effect size (≥.06).
p ≤ .003.
Data Analysis
We used IBM SSPS Statistics (Version 25) to analyze the data. Normality was established using the Kolmogorov–Smirnov statistic. Descriptive statistics are reported using means and standard deviations for continuous data and frequencies for categorical and dichotomous data.
To describe hand impairment and function, we compared dominant hand scores to normative data and stratified data for comparison between groups within the total cohort. Grip strength and lateral and tip pinch scores were normalized for age and weight (Stansfield et al., 2003). Lateral and tip pinch results were compared to Australian normative data (Kunovsky et al., 2017) because no normative z-score reference values were available. Grip strength, 9-HPT, and FDT age and gender raw scores were converted into dimensionless z scores for standardized comparison (University of Sydney, n.d.). The 9-HPT and FDT z scores were recoded to positive z scores (Burns et al., 2012; McKay et al., 2016, 2017). Using the normal distribution curve, standard distribution z scores more than 2 SD below the mean were considered impaired and those more than 3 SD below the mean were considered significantly impaired (Portney & Watkins, 2009).
Because the prevalence of GJH varies with age and sex, and because maturity is expected to result in improved hand function, scores were stratified for comparison of hypermobility between boys and girls (Singh et al., 2017) and between primary students (ages 8–12 yr) and secondary students (ages 13–18 yr). Scores were also stratified between two major diagnostic groups, OI and EDS–HT/JHS, because it has not been established whether type of HDCT affects performance and function. Independent sample t tests were used to evaluate differences between groups. To control for the familywise error rate, the Bonferroni-corrected significance level was set at p ≤ .003. The observed power was calculated to determine whether the group size was sufficient to achieve a significant difference (observed power >.80) between groups (Greenland, 2012; Portney & Watkins, 2009). Box plot representation was used to compare grip strength, 9-HPT, and FDT z scores between primary and secondary student groups. Paired t tests were used to compare change in pain and fatigue for the button test and the HST and change in letters written per minute, pain, and fatigue between the first and last 3 min of the 9-min writing task.
To determine the extent to which hand impairment and function explain the variation in self-reported functional performance, independent variables were entered into a multiple regression model and analyzed using adjusted R 2. Correlations between outcome measures were established (rs > .65) to minimize collinearity (Taylor, 1990).
Results
Participants
Ninety eligible participants were invited to participate between May 2017 and August 2019. Fourteen declined, and 3 were excluded—2 did not meet the GJH age- and gender-specific criteria for EDS–HT/JHS, and 1 had a concurrent diagnosis of Graves’ disease. Therefore, 73 participants (31 male, 60 right-hand dominant) were included. Participants were ages 8.0–17.8 yr (M = 13.1, SD = 3.2); 35 were in primary and 38 in secondary school. The majority were diagnosed with either OI (47%) or EDS–HT/JHS (41%) and the remainder with MFS (7%), unclassified HDCT (4%), and LDS (1%). Half of participants reported difficulties with hand function, attributing the cause to pain (67%) and/or fatigue (60%). The majority of OI participants (91%) had a history of bisphosphonate treatment, which is standard practice in the medical management of OI (Dwan et al., 2016). Participants’ physical characteristics are summarized in Table 1.
Tests of Hypermobility
For the tests of hypermobility, mean scores were significantly lower for boys than for girls (Table 1). Of the 48 (66%) participants who met the Beighton score cutoff, 27 (56%) were female and 14 (29%) had a diagnosis of OI. Of the 18 (25%) participants who met the ULHAT ≥7/12 cutoff score, the majority (n = 15; 83%) were female; there were no significant differences between children of differing diagnostic or age groups (all ps > .60).
Clinical Measures of Hand Function
Comparisons of performance-based and patient- reported outcome measures between primary and secondary age groups are provided in Table 2. Grip strength, 9-HPT, and FDT mean z scores were below expected norms, with no significant differences between groups (Table 2; see also Figure 1). Grip strength z scores for 18 participants (25%) were >2 SD below the mean; 10 were primary students and 8 secondary students, with an even distribution of those with OI and those with EDS–HT/JHS. Fourteen (19%) had z scores >2 SD below the normative mean for the 9-HPT, and 7 (10%) had z scores >2 SD below the normative mean for the FDT. Fine motor integration and fine motor precision mean-scaled scores were below expected norms; secondary students performed significantly worse than primary students in both (Table 2).
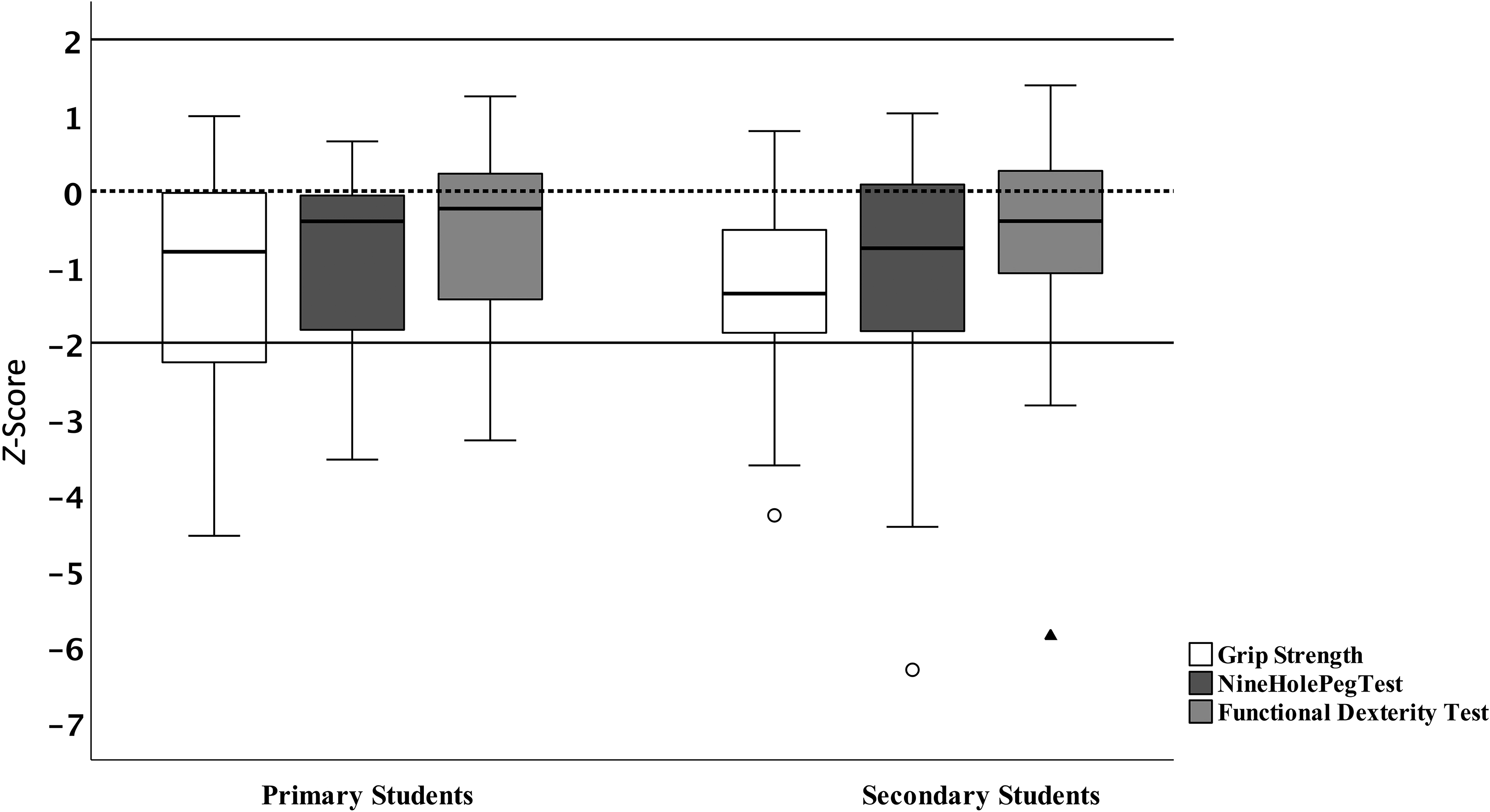
Box plot representation of z scores for grip strength, Nine-Hole Peg Test, and Functional Dexterity Test.
Assessment Scores, With Comparison Between Age Groups
Note. BOT–2 = Bruininks–Oseretsky Test of Motor Proficiency, 2nd ed.; CHAQ–38 = Childhood Health Assessment Questionnaire; HST = 3-min Handwriting Speed Test; LPM = letters per min; N = newtons; NA = not available; PMDS–2 = Peabody Developmental Motor Scales, 2nd ed.
α = .05; observed power >.80 indicates sufficient sample size to achieve significance (Portney & Watkins, 2009).
α = .05; effect size >.06 is moderate to large.
N = 66, t(64); no Australian normative data are available.
p < .003.
Pain and Fatigue With Function Tasks
The button test mean score was within expected norms, with no significant differences in pain or fatigue between differing diagnostic or age groups (all ps > .40; Figure 2). On the HST, the mean number of letters written in 3 min was below that of a control group of similar-age typically developing Australian children (Kunovsky et al., 2017); 19% of the sample had HST scaled scores below expected norms (Wallen et al., 1996). Four participants (ages 16–17 yr) had scaled scores ≤3, indicating significantly impaired handwriting speed. Despite no significant difference between participants with OI and those with EDS–HT/JHS (p > .20), secondary students had significantly lower scaled scores on the HST than primary students (Table 2).
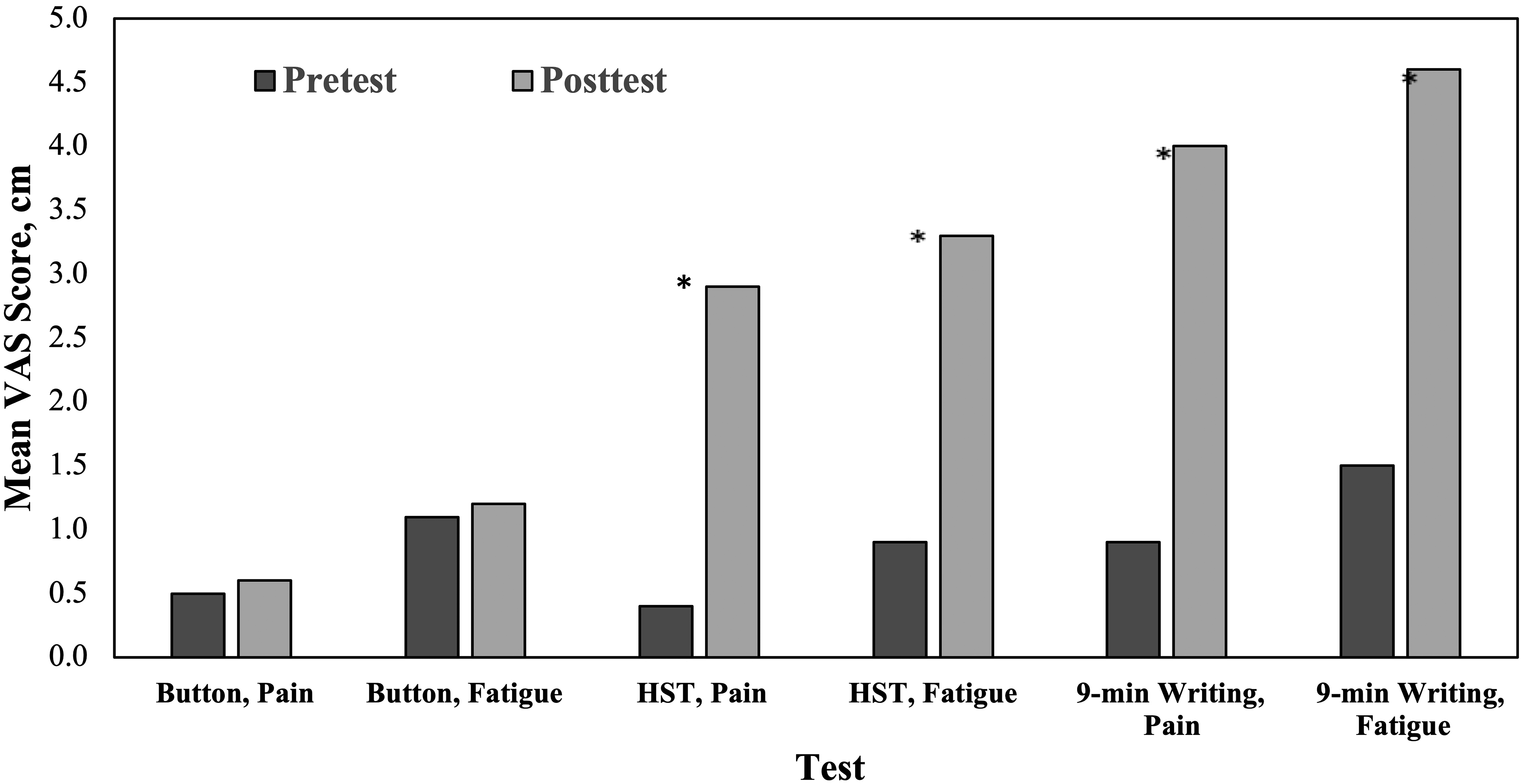
Pretest and posttest pain and fatigue scores on the button test, Handwriting Speed Test, and 9-min writing task.
Regarding the 9-min writing task, 20% of participants (n = 15) did not complete it. Six primary students and 1 secondary student did not attempt the task because of pain and/or fatigue. Of the 66 participants who commenced the task, 5 primary and 3 secondary students did not complete it, citing pain (n = 2), fatigue (n = 2), or no reason (n = 4). Writing output in letters per minute decreased significantly from the first 3 min of the task (M = 94.0, SD = 36.3) to the last 3 min (M = 75.1, SD = 46.8), t(65) = 5.6, M deviation = 19, 95% confidence interval [CI] [12.1, 25.5], p < .001, with a large effect size (η2 = .33). Participants reported significant increases in pain and fatigue after completing both the 3-min HST and the 9-min writing task (p < .001), as shown in Figure 2.
Patient-Reported Functional Performance
Our participants demonstrated difficulty with functional performance compared with norms for the CHAQ–38 total score, with the greatest difficulty in the Dressing and Grooming domain (Table 2). We found no significant difference between primary and secondary students in total CHAQ–38 scores; however, primary students performed significantly worse than secondary students for the Dressing and Grooming domain and the Eating domain (Table 2). Applying a disability index established for children with juvenile idiopathic arthritis (Dempster et al., 2001), the mean score of 0.50 for our sample fits into the mild to moderate disability level (0.63) on that index, with 7% showing no disability (0), 18% mild disability (0.13), 49% mild to moderate disability (0.63), 25% moderate disability (1.75), and 1% more than moderate disability (>1.75).
Impact of Hand Impairment and Function on Self-Reported Functional Performance
To minimize collinearity, we determined correlations between measures of hand impairment and function before entering the independent variables into a multiple regression analysis. Six independent variables representing different constructs of hand impairment and function (grip strength, 9-HPT, and FDT z scores; HST scaled score; button test average speed; and ULHAT score) were entered into a stepwise regression with CHAQ–38 scores as the dependent variable. Grip strength accounted for 6% of the variation in the CHAQ–38 total score (β = –0.27, p = .02), with no other constructs predicting variability in this measure. Stepwise regression analyses performed on the three CHAQ–38 domains associated with hand function revealed the following: ULHAT (β = 0.36, p < .001) and FDT (β = –0.22, p = .047) scores explained 16% of the variability in the Eating domain, with upper limb hypermobility predicting more variability in performance than dexterity. Upper limb hypermobility accounted for 8% of the variability in the Grip domain (ULHAT β = 0.3, p = .01). Buttoning speed accounted for 4% of the variability in the Dressing and Grooming domain (β = 0.24, p = .04).
Discussion
In this cross-sectional study, we explored hand impairment and function in children and adolescents with HDCTs. Overall, our participants had poorer hand function than a normative sample of typically developing peers. Hand pain and fatigue interfered with participants’ performance of daily activities, including handwriting. The large variability in hand function we found reflects the heterogeneous nature of participants’ conditions while also highlighting shared musculoskeletal features, including reduced grip strength and dexterity and upper limb hypermobility, which have a negative effect on functional performance.
It remains unclear why secondary students had grip strength scores, which are expected to increase with age, similar to those of primary students (McKay et al., 2016). Muscle weakness has been described as part of EDS–HT disease progression (Castori et al., 2012), and reduced muscle strength and endurance in adults have been linked to pain and reduced activity (Coussens et al., 2021). Occupational therapy practitioners can develop and implement specific interventions that target impaired hand function, especially hand and grip strengthening. Despite their grip strength deficit, secondary students’ functional hand performance was better than that of primary students. Older children may have sufficient cognitive maturity and self-determination (Deci & Ryan, 2000) to use compensatory strategies to become independent in self-care activities. Nevertheless, upper limb impairment can have a detrimental effect on hand function regardless of age.
Hand pain and fatigue, poor grip strength, and lack of endurance appear to be factors influencing hand function for children and adolescents with HDCTs. Participants were able to complete a short buttoning task within the expected time without symptoms. Performance was poorer for writing tasks; many participants were unable to complete the longer writing task and reported significantly increased levels of pain and fatigue. Upper limb hypermobility and joint instability (Castori & Hakim, 2017) may reduce the ability to sustain a pen grasp, causing hand pain and fatigue over time (Pacey et al., 2014). Hand pain and fatigue during sustained grasping tasks, such as maintaining a pen grip during note taking, completing timed assessments, or grasping cutlery to cut food, should be monitored throughout the secondary school years within a comprehensive hand function assessment.
Only a small proportion of the variation in self- reported functional performance was explained by objective functional measures of grip strength, upper limb hypermobility, and dexterity. A generic functional measure such as the CHAQ–38 may not be as sensitive to differences in physical capacity as a disease-specific measure would be. In addition, the CHAQ–38 is a self-report measure requiring subjective interpretation of function in contrast rather than objective measures of performance; CHAQ–38 scores thus may not be a good indicator of true functional capacity. For example, parental assistance beyond the age of independence (Chien et al., 2014) and use of compensatory strategies (e.g., hook-and-loop fasteners instead of buttons) may result in a mismatch between perception of and actual function. Further, the CHAQ–38 encompasses whole-body functional performance, so other factors associated with HDCTs that were not assessed in this study, such as joint instability and laxity at other joints (Castori & Hakim, 2017), bony deformities (Mueller et al., 2018), or poor proprioception (Sahin et al., 2008), might also account for variability in self-reported functional performance.
Limitations
Many participants had difficulty maintaining a steady hold on the digital pinch grip attachment (Burns et al., 2012), which may have affected the results. A more sensitive tip pinch measure could provide more accurate results. Our sample was relatively small, although larger than those of similar studies; the small sample size reduced the power for finding significant between-sex differences in hypermobility and significant age group differences in fine motor precision, fine motor integration, and handwriting speed. A longitudinal study would provide greater insights into the progression and natural history of hand function over time.
Implications for Occupational Therapy Practice
This study provides insights into performance skills and musculoskeletal features associated with generalized joint hypermobility that influence hand function and daily activities for children and adolescents with HDCTs. Implications of this study for occupational therapy practice include the following: ▪ Children and adolescents with HDCTs have poor hand function compared with typically developing age-matched peers; reduced grip strength and hand pain and fatigue affect performance. ▪ Monitoring of hand function is warranted throughout schooling because secondary students may continue to experience difficulties. ▪ Evaluation of hand impairment and function using performance and physical outcome measures can guide clinical practice in the context of a multidisciplinary approach for children and adolescents with HDCTs.
Conclusion
This study provides preliminary evidence that children and adolescents with heritable disorders of connective tissue have poor hand function compared with their peers. Reduced grip strength and hand pain and fatigue negatively impact hand function. A comprehensive evaluation of hand impairment and function and ongoing monitoring throughout the school years are warranted to identify students who fall behind, regardless of age, and provide intervention to reduce impairment and improve function (Pacey et al., 2014). Further research is needed to guide clinical practice.
Supplemental Material
Supplementary material for Hand Impairment and Function in Children and Adolescents With Heritable Disorders of Connective Tissue
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.049282.pdf for Hand Impairment and Function in Children and Adolescents With Heritable Disorders of Connective Tissue by Alison Wesley, Paula Bray, Verity Pacey, Cliffton Chan and Leslie L. Nicholson in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank Professor Craig Munns for contributions to the design phase of the study, ConnecTeD Foundation for providing funding to purchase assessments, and participants and their families for their invaluable time.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.