
Abstract
The findings of this study support the use of weighted blankets, in conjunction with occupational therapy interventions, as potentially a beneficial non-pharmacological option for patients with anorexia nervosa (AN) and avoidant–restrictive food intake disorder (ARFID).
Anorexia nervosa (AN) and avoidant–restrictive food intake disorder (ARFID) are psychiatric disorders that can result in serious medical complications, often requiring medical stabilization in an inpatient setting (Hoek, 2006; Kästner et al., 2018; Mehler & Anderson, 2010; Nakai et al., 2016; Watson & Bulik, 2013). Anxiety is a prevalent psychiatric comorbidity of AN and ARFID; however, little is known regarding the efficacy of interventions aimed at reducing anxiety among hospitalized patients with AN and ARFID (Kaye et al., 2004; Meier et al., 2015). Given that anxiety is a common comorbidity, it is appropriate to examine interventions that have demonstrated potential for treating anxiety in broader populations (Eron et al., 2020). Moreover, AN, ARFID, and anxiety all affect people’s ability to function in daily life; therefore, occupational therapy interventions have the potential to reduce the adverse impact these conditions have on daily functioning and health outcomes (Clark & Nayar, 2012; Osuch et al., 2019). An appropriate focus that is gaining more exposure in nonpharmacological interventions for treating anxiety is deep pressure touch stimulation (DPTS) modalities, such as weighted blankets (Edelson et al., 1999; Grandin, 1992; Mullen et al., 2008; VandenBerg, 2001). The primary objective of this pilot study was to determine whether the use of weighted blankets decreases self-reported anxiety symptoms among patients with AN, including the restricting (AN–R) and binge–purge (AN–BP) subtypes, and ARFID.
Deep Pressure Touch Stimulation
DPTS is a form of tactile sensory input or pressure applied to the body that replicates the sensation of a firm hug, swaddle, or squeeze (Chen et al., 2013; Edelson et al., 1999; Grandin, 1992; Krauss, 1987). DPTS can potentially decrease anxiety and improve emotional regulation, allowing some people to feel more relaxed, secure, comfortable, safe, and calm (Edelson et al., 1999; Grandin, 1992; Mullen et al., 2008; VandenBerg, 2001). A mechanism for this improvement is DPTS’s reduction of sympathetic arousal, resulting in an increase in parasympathetic arousal of the autonomic nervous system (Chen et al., 2013; Reynolds et al., 2015). DPTS is typically used to manage anxiety among various populations, including people with sensory modulation, cognitive, or psychological disorders or diagnoses (Chen et al., 2013; Krauss, 1987; Mullen et al., 2008; Zissermann, 1992).
Occupational Therapy and Anxiety Reduction
DPTS modalities, such as weighted blankets, are commonly used by occupational therapists to reduce anxiety and improve daily functioning among various populations (Eron et al., 2020). Encompassing a biopsychosocial model of practice, occupational therapy interventions are individualized to optimize daily functioning by addressing the intersection among biological, psychological, and social factors (Gentry et al., 2018). As a result, occupational therapy interventions empower the return to meaningful health by promoting daily activities that restore function in everyday life (American Occupational Therapy Association [AOTA], 2020). Occupational therapy interventions aim to reduce anxiety as a standard of care for clients with eating disorders (Clark & Nayar, 2012; Osuch et al., 2019; Robinson et al., 2005). Although not exhaustive because of the individualized nature of the occupational therapy process (AOTA, 2020), some examples of anxiety reduction interventions we have used are diaphragmatic breathing training, restorative yoga, mindfulness activities, assessment and exploration of sensory processing, development of self-regulation skills through use of sensory tools, and structuring purposeful leisure participation to reduce preoccupation with eating disorder thoughts and behaviors.
Method
Trial Design
This was a single-center, two-arm parallel-groups randomized controlled trial (RCT). Patients were randomized into the intervention or control group.
Study Setting
This study took place at the Acute Center for Eating Disorders at Denver Health (ACUTE). ACUTE is a 30-bed inpatient unit for medically compromised patients with severe eating disorders that require definitive medical stabilization. ACUTE provides a unique opportunity to examine the use and efficacy of weighted blankets for anxiety among patients diagnosed with AN or ARFID.
Inclusion Criteria
Patients were eligible for study inclusion if they had been clinically diagnosed by an ACUTE psychologist with AN or ARFID, per the criteria of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; American Psychiatric Association, 2013); were exhibiting moderate anxiety, as indicated by a Beck Anxiety Inventory (BAI) score of >22; and if the occupational therapist determined they could safely participate. Patients were excluded if they were younger than age 18 yr, had an active infection control concern, had clinically significant skin breakdown, were unable to perform safe bed mobility, or were at risk for increased eating disorder behaviors related to weighted blanket use.
Informed Consent Process
Per usual standard of care, each patient received an initial occupational therapy visit within 72 hr of their admission. During this initial evaluation, patients were screened for inclusion and exclusion criteria and appropriateness to participate in the study by their primary practicing occupational therapist (Rachel Ohene or Christina Logan). The research team was then notified if the patient was eligible. A trained member of the research team provided the patient with information on the study and obtained written consent. The patient was then randomized into either the control or the intervention group.
Intervention
Patients in both groups were treated per the usual unit protocols, including client-centered occupational therapy plans of care developed in collaboration with the patient. Usual-care interventions are aimed at rehabilitating a patient’s capacity to participate safely and effectively in their daily activities and to successfully meet the activity demands of a lower acuity level of care. Occupational therapy interventions included training, education, and therapeutic activities, including relaxation strategies. Specifically, these interventions included diaphragmatic and yogic breathing exercises, mindfulness-based cognitive therapy (MBCT) education and exercises, therapeutic restorative yoga activities, occupational therapy group participation, aromatherapy, identifying and promoting engagement in meaningful leisure activities, client-centered sensory diets to provide patients with consistent preferred sensory experiences, and individualized checklists and schedules to grade the self-initiation of effective coping strategies. Interventions chosen by the occupational therapist were client centered, with an emphasis on positive coping strategies.
Per usual care, occupational therapists continued to perform reassessments and ongoing consultation to optimize patients’ engagement in anxiety-reducing activities and routines. During their admission, patients received occupational therapy services anywhere from one to five times per week, and they typically had a reduction in visit frequency as their independence in daily occupations improved. The frequency and duration of visits and patient needs were ultimately determined by the occupational therapist’s plan of care.
Patients in the intervention group received both usual care and a weighted blanket. The appropriate assigned weighted blanket weight was within 1 lb ± 10% of the patient’s admission weight (Chen et al., 2013). During the initial occupational therapy assessment, the weighted blanket was used as an intervention, and patients were asked to use it for at least 5 min and reflect on their experience. During this assessment, patients were asked to lay supine with the head of the bed elevated. The patient covered themselves with the weighted blanket either fully or partially. The occupational therapist provided education to the patient on the use of the weighted blanket for the rest of their admission. Patients were free to use the weighted blanket at their discretion; however, use was not permitted during meals and ambulation. Occupational therapists continued to conduct follow-up evaluations and consultations in which they educated, answered questions from, and reminded patients of the utility of using their weighted blanket. After this initial assessment, patients could use their weighted blanket to cover themselves as needed.
Outcomes
All study participants completed the BAI during the initial occupational therapy evaluation and again within 72 hr of discharge. The BAI is a validated scale that consists of a list of 21 identified symptoms of anxiety, spanning both physiological and psychological experiences. Respondents are asked to rate the severity of how much each symptom had bothered them within the previous month on the following scale: 0 (not at all), 1 (minimum, it bothers me a little), 2 (moderately, it is not pleasant at times), and 3 (severely, it bothers me a lot). The total score ranges from 0 to 63; scores ranging from 0 to 21 indicate low anxiety; 22 to 35, moderate anxiety, and ≥36, severe anxiety. The BAI has high internal consistency (Cronbach’s α = .92) and a test–retest reliability over 1 wk of .75 (Beck et al., 1988).
The Subjective Units of Distress Scale (SUDS) is a self-report instrument that allows patients to rank their level of anxiety, discomfort, and distress in increments of 10, ranging from 0 (totally relaxed) to 100 (highest distress/fear/anxiety/discomfort that you have ever felt). The SUDS was administered during the initial occupational therapy evaluation and during subsequent occupational therapy treatment sessions. Across both groups, SUDS scores were collected at the start and end of each session to measure the change in anxiety in response to occupational therapy interventions. The SUDS was also administered to the intervention group by the occupational therapist, immediately before the initial weighted blanket administration and again after 5 min of use (Tanner, 2012; Wolpe, 1982).
Demographic Variables
Demographic variables were collected via chart review. These included age, length of hospitalization, admission body mass index (BMI), and admission percentage of ideal body weight (IBW).
Randomization and Sample Size
Randomization was used to provide chronological balance between treatment arms during patient enrollment with respect to measured and unmeasured patient characteristics and the number of patients allocated to each treatment arm; thus, the treatment groups were balanced with respect to possible changes in the mix of patients over time. A statistician generated the randomization schedule and implemented it through an automated process. The randomization schedule consisted of balanced blocks within strata to ensure relative equality of assignment across treatment groups. The block sizes were varied and randomly permuted to prevent the possibility that assignments might be influenced by predicting the next assignment, which is heightened when a fixed block size is used. The block size was not revealed to the investigators and was randomly selected from a small number of different block sizes to help reduce the likelihood of an investigator predicting the next treatment assignment. Assignments were created before patient enrollment and sealed in envelopes that were used during the informed consent process.
Power analysis suggested that 24 participants would detect a moderate difference with a power of .80 and α of .05. Moreover, this number of participants was determined to be the most feasible, given the unit size, availability of weighted blankets, and the unit’s admission rate. This study was approved by the Colorado Multiple Institutional Review Board and retrospectively registered through ClinicalTrials.gov (NCT04191720).
Statistical Analysis
Univariate and bivariate analyses consisting of frequencies, percentages, means, and standard deviations were conducted. We conducted bivariate analysis on demographics and outcomes to test differences between the control and intervention groups. The Shapiro–Wilks test was used to test for normality, and t, Wilcoxon, and χ2 tests were used, as appropriate.
In analyzing the results from the BAI, we conducted a generalized linear model with random effects. Model inputs included a group variable that indicated whether the observation was in the control or intervention group, a time variable indicating admission or discharge BAI score, and an interaction term. A random intercept effect at the subject level was added to the model. Available case analysis was conducted for missing data. For the SUDS results, we created a negative binomial mixed regression model to assess the impact of weighted blankets, adjusting for the number of occupational therapy visits. Incident rate was estimated from these models. We considered p < .05 statistically significant, and all analyses were completed using R (Version 3.3.2; R Core Team, 2016).
Results
From November 1, 2018, through March 25, 2019, 96 patients were screened for inclusion; 59 patients did not meet criteria, 8 were not approached because the treatment team felt their participation would not be beneficial to them, and 5 declined (Figure 1). Twenty-four participants were enrolled in the study; however, 1 participant had a change in diagnosis that warranted exclusion. There were 12 patients (52.2%) in the control group and 11 patients (47.8%) in the intervention group. At admission, mean BMI was 13.9 kg/m2 (SD = 1.3) and 13.7 kg/m2 (SD = 1.3) for the control and intervention groups, respectively, and the percentage of IBW was 66.0% (SD = 6.7) and 64.9% (SD = 6.7), respectively. The cohort consisted of mostly women (n = 21; 91.3%), who were, on average, age 27 yr (SD = 10.6). Most patients were diagnosed with AN–R (n = 12; 52.2%). There were no significant differences in demographics between the control and intervention groups (Table 1).
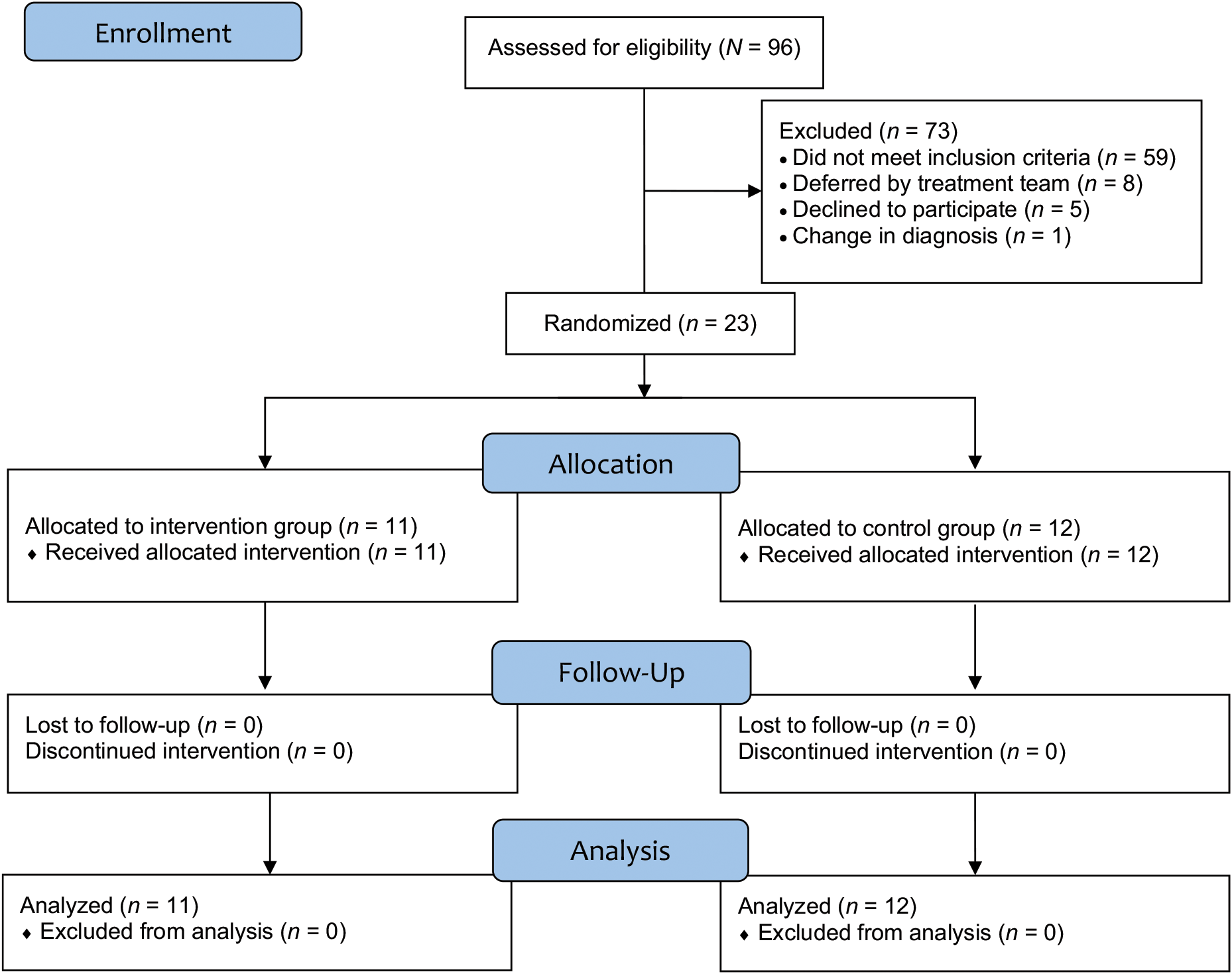
Patient enrollment and data collection workflow.
Bivariate Comparisons Between Groups on Selected Demographics and Outcomes (N = 23)
Note. Percentages may not total 100 because of rounding. AN = anorexia nervosa; AN–BP = anorexia nervosa–binge purge subtype); AN–R = anorexia nervosa–restricting subtype; ARFID = avoidant–restrictive food intake disorder; BAI = Beck Anxiety Inventory; BMI = body mass index; % IBW = percentage of ideal body weight; n/a = not applicable; SUDS = Subjective Units of Distress Scale; WB = weighted blanket.
p value calculated by t test, Wilcoxon, or χ2 test, as appropriate.
p value calculated by a paired t test between preintervention SUDS and postintervention SUDS for initial weighted blanket use.
Average admission BAI score for the control and intervention groups was 36.9 (SD = 8.1) and 34.4 (SD = 8.9), respectively, t(22) = 0.72, p = .47. There was a significant reduction in SUDS score before (M = 47.3, SD = 28.7) and after (M = 32.7, SD = 21.7) the initial use of the weighted blanket, t(22) = −5.03, p < .001.
For preintervention SUDS, there was a non–statistically significant difference between the control group (M = 61.5, SD = 17.9) and the intervention group (M = 52.9, SD = 27.1), t(66) = 1.76, p = .08. The negative binomial mixed-effects model suggested an incident rate ratio of .81 (95% confidence interval [CI] [0.59, 1.05]). This indicated that for patients in the intervention group, the SUDS score was expected to decrease by 19% compared with patients in the control group (p = .12).
Mixed regression models suggested a reduction in BAI scores across time and between groups. Between admission and discharge, there was a statistically significant reduction of 7.99 points in BAI score (95% CI [−1.55, −0.6], p = .04). Between the control and intervention groups, there was a reduction of 1.21 points in BAI score (95% CI [−18.4, 15.9], p = .88; Table 2). In addition, the results show that the intervention group had a greater decrease in BAI score over time compared with the control group (1.16 points; 95% CI [−12.3, 9.93], p = .83). Figure 2 displays the bar plots for BAI scores by group and time.
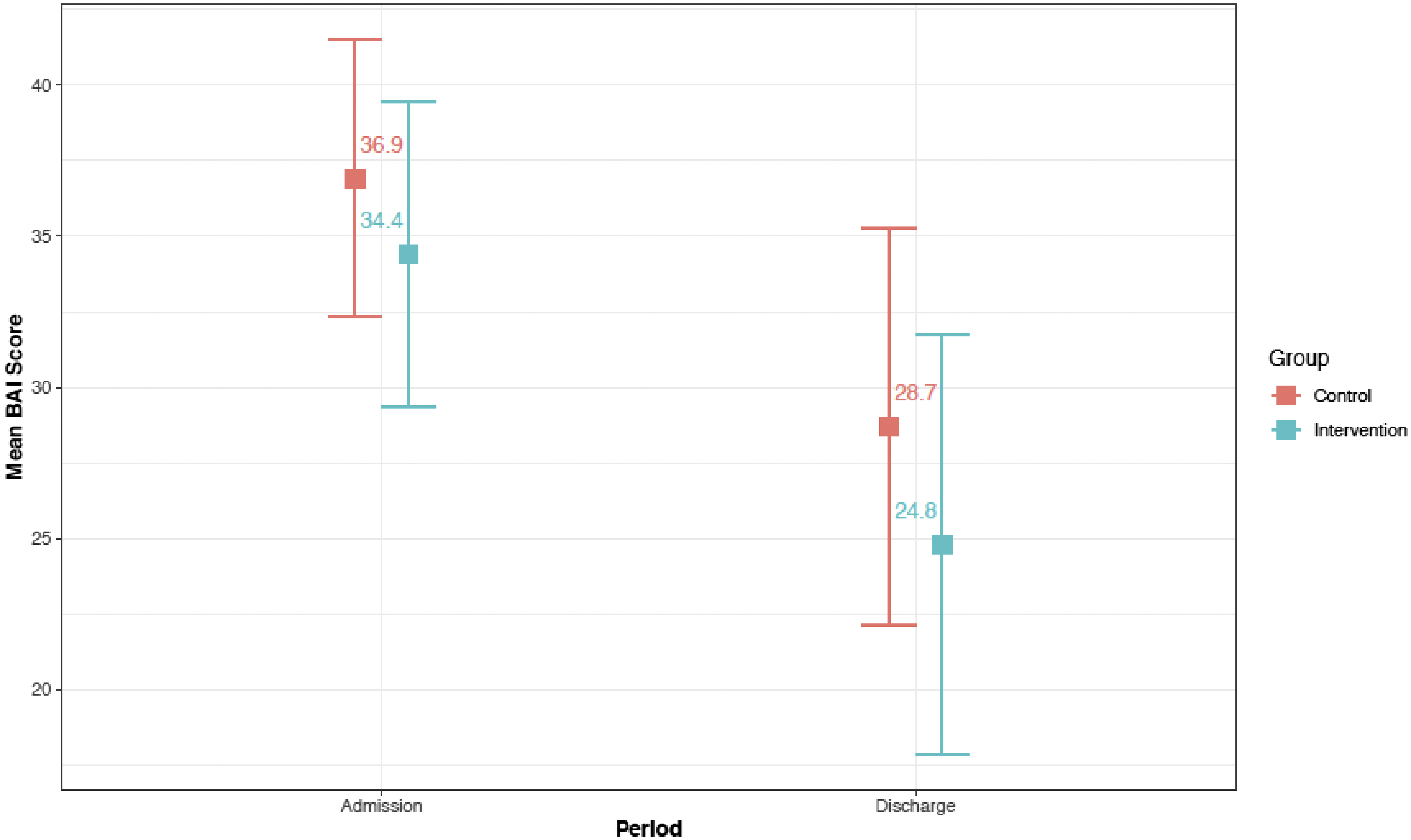
Box plot demonstrating change in BAI score for the control and intervention groups from admission to discharge.
Parameter Estimates From Specific Adjusted Models for BAI and SUDs
Note. BAI = Beck Anxiety Inventory; CI = confidence interval; OT = occupational therapy; SUDS = Subjective Units of Distress Scale.
Estimates calculated from a mixed-effects linear model with subject random effects.
Estimates calculated from a mixed-effects negative binomial model with subject random effects.
Discussion
This pilot study sought to demonstrate the effect of weighted blankets as a treatment modality for anxiety among hospitalized patients diagnosed with AN–R, AN–BP, or ARFID. The results suggest a decrease in anxiety between the control and intervention groups, as well as across time from admission to discharge. Moreover, scores on the BAI and SUDS indicated a decrease in anxiety symptoms.
From the BAI results, the biggest decrease in anxiety symptoms (by 7.99 points), regardless of group assignment, was observed between admission and discharge. A possible reason for this result may in part be the inpatient treatment the patients receive. ACUTE implements a multidisciplinary team approach that incorporates medicine, nursing, occupational therapy, physical therapy, registered dietitians, social work, psychology, and psychiatry to medically stabilize patients and promote weight restoration. Each discipline is integral to the eating disorder treatment team and patient care.
To date, primary management and treatment of AN and ARFID predominantly focus on pharmacological therapies, nutritional rehabilitation, and psychotherapy (Chakraborty & Basu, 2010; Watson & Bulik, 2013). Pharmacological therapies to manage anxiety are somewhat limited with this patient population because of patient refusal, low body weight, and the complexity of their medical instability (Flament et al., 2012; Halmi et al., 2005). Multidisciplinary treatment of eating disorders does not routinely include occupational therapy. Yet, because the role and aim of occupational therapy are to effectively assess and treat a wide range of physical, cognitive, functional, and psychological deficits, this discipline is well suited to meet the unique needs of those with severe eating disorders, including anxiety reduction. In this study setting, with the goal of preparing patients to succeed after discharge, the occupational therapists directly addressed anxiety reduction through client-centered interventions in order to better equip patients to meet self-care and treatment activity demands. The change in SUDS score from pre- to postintervention may demonstrate a reduction in anxiety in response to occupational therapy interventions across both groups, providing evidence to suggest that occupational therapy services contributed to the decrease in anxiety to some extent.
The results of this pilot RCT show a non–statistically significant reduction in anxiety between the control and intervention groups of 1.21 points on the BAI. The initial use of the weighted blanket during an occupational therapy visit resulted in a statistically significant reduction in preintervention and postintervention SUDS scores. This reduction in anxiety coincides with results reported in the current literature. For example, among eight weighted blanket studies we examined, five evaluated the use of weighted blankets for anxiety (Eron et al., 2020). Four studies found that weighted blankets decreased anxiety, and the fifth showed inconclusive results in a small sample of 3 participants (Champagne et al., 2015; Chen et al., 2013, 2016; Losinski et al., 2017, Mullen et al., 2008). Moreover, for certain individuals, a 1.21-point difference in BAI score could mean a change from severe to moderate anxiety or from moderate to low anxiety, suggesting potential clinical significance on a case-by-case basis (Guyatt et al., 2002). In practice, this drop in BAI score could result in a patient being less anxious enough to eat more, sleep better, or engage in a health-promoting activity. Thus, the results of this RCT suggest that weighted blankets could be a readily available tool, allowing those with AN or ARFID who might otherwise be limited by high or moderate anxiety to participate in treatment activities. However, further research is needed to fully assess the effectiveness of weighted blankets in this population.
This pilot RCT is the first study to evaluate the effectiveness of weighted blankets in reducing anxiety among patients diagnosed with AN and ARFID. However, it has limitations. This population may be unique in their medical acuity, limiting the generalizability of the results to this specific population. The subjective nature of the tools used to assess anxiety may not have captured patients who minimized their anxiety, were diagnosed with anxiety, or were observed to present with behaviors consistent with anxiety. Finally, use of the weighted blanket could not be minutely captured, particularly with respect to time used. Weighted blanket use was observed by staff, but capturing the data was difficult. However, from a qualitative standpoint, the occupational therapists found that patients were generally amenable to using the weighted blanket as needed.
The opportunities for further research on this topic are vast. Further exploration of how weighted blankets affect specific daily activities, such as sleep and meal completion, could more accurately determine functional implications and help achieve better overall outcomes for people with AN or ARFID. This sensory intervention could also show promise for decreasing the sensory–perceptual factors of body image disturbance and sensory modulation symptoms that are often associated with eating disorders (Merwin et al., 2013; Zucker et al., 2013). Additional exploration of this tool across multiple sites and levels of care could also better determine its efficacy and effectiveness at various stages of weight restoration.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: ▪ Including occupational therapy on a highly versatile, multidisciplinary treatment team can elevate the standard of care for people with severe eating disorders. ▪ Occupational therapy practitioners should advocate for inclusion in the treatment team as a standard of care for this population because of the potential benefit of sensory interventions, such as DPTS, in decreasing anxiety and optimizing functioning for necessary occupations. ▪ The use of weighted blankets may be an efficacious intervention for reducing anxiety, although further research is indicated. ▪ Severe malnutrition is associated with physical limitations; thus, for safety reasons, DPTS interventions should be introduced by clinicians trained in both mental and physical functioning; occupational therapy practitioners are uniquely suited for this.
Conclusion
For those with eating disorders, anxiety can impede participation in meaningful life activities; thus, finding strategies to mitigate anxiety to support function is an example of how occupational therapists are well suited to address anxiety among this population (Clark & Nayar, 2012). This study shows that DPTS, specifically weighted blankets, may be an effective tool for reducing anxiety among patients with AN or ARFID. Because of the physical limitations associated with severe malnutrition, for this population it is important for DPTS interventions to be introduced by clinicians trained in both mental and physical functioning for safety reasons, for which occupational therapists are uniquely suited. This study shows promise that the use of weighted blankets may be an efficacious intervention for reducing distress and anxiety; however, further testing is indicated. Finally, establishing occupational therapy standards of care through rigorous research inquiry for those with eating disorders is necessary in order to further develop best practice treatment approaches.
Footnotes
Acknowledgments
We thank Melissa Weisner-Rose, MS, OTR, CAC III; Lindsey Kohnert, MEd, OTD, OTR/L; Jane Marshall, OTD, OTR/L; and Krista Hovde, BSN, for their contributions to the study design and data collection. The data that support the findings of this study are available from the corresponding author upon reasonable request. This study was retrospectively registered through ![]() (NCT04191720).
(NCT04191720).