
Abstract
This review supports the use of the available literature for client education, upper extremity training, and cognitive training alongside clinical reasoning to improve work, leisure, and social participation outcomes among clients poststroke.
Cerebrovascular accidents, otherwise known as strokes, are a result of either a blockage of blood flow to the brain or a ruptured blood vessel in the brain (Virani et al., 2021). With improvements in acute stroke interventions, nearly 85% of people survive the initial blockage or rupture event (Virani et al., 2021). Nearly 25% of adults who experience a stroke each year are still of working age, and almost 50% of those living with a stroke are younger than age 65 yr (Virani et al., 2021). The total cost of stroke globally is estimated at about $49.8 billion annually (Virani et al., 2021). Part of this high amount is the indirect cost of stroke because of lost wages from people not being able to return to work or a family member stopping employment and taking on a caregiving role (Joo et al., 2014). Motor, cognitive, sensory, and other body structure and function impairments are common and can affect performance and participation in everyday occupations. People poststroke desire to return to or engage in new occupations, such as attending a weekly luncheon, hosting game night, or visiting their grandkids on the weekend (American Occupational Therapy Association [AOTA], 2020).
After a stroke, the changes and disruptions to the person’s life can substantially affect social participation, and the process of reengaging in occupations is dynamic and continuous (Woodman et al., 2014). As described in the Occupational Therapy Practice Framework: Domain and Process (4th ed.; AOTA, 2020), social participation is defined as “activities that involve social interaction with others, including family, friends, peers, and community members, and that support social interdependence” (p. 34). Working-age adults often desire to and attempt to return to work, sometimes unsuccessfully (Wolf et al., 2009). In addition to spending time at work and in volunteer activities, adults poststroke can have limitations participating in leisure occupations that are nonobligatory, such as fishing, playing cards, or reading a book. Occupational therapy practitioners can address limitations in work, leisure, and social participation with those who have experienced a stroke through a variety of approaches, such as problem solving and education (Wolf et al., 2015). The purpose of this systematic review was to answer the following clinical question: “What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve social participation, work, and leisure among adults poststroke?”
Method
This systematic review was conducted according to the Cochrane Collaboration methodology (Higgins et al., 2019) and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting a systematic review (Moher et al., 2009). The protocol was developed a priori with input from experts in the area, a research methodologist, and AOTA staff (CDR 420220161214).
Literature Search and Study Selection
The authors, outside experts, a medical librarian, a research methodologist, and the AOTA Evidence-Based Practice Program team collaborated to identify the research question and search terms (see Supplemental Table A.1 in the Supplemental Appendix, available online with this systematic review at https://research.aota.org/ajot). The medical research librarian performed a search of the MEDLINE, PsycINFO, CINAHL, OTseeker, and Cochrane databases for articles published between January 1, 2009, and December 31, 2019. An initial review of article titles was conducted by the research methodologist, and duplicates and any articles clearly not meeting inclusion criteria (Table 1) were removed (i.e., wrong population, wrong publication year, not research). The remaining articles were then provided to the authors for review.
Inclusion and Exclusion Criteria for the Systematic Review
Note. AOTA = American Occupational Therapy Association; RCT = randomized controlled trial.
The authors screened the remaining studies using abstracts and finally full texts to confirm eligibility. All stages of the review were conducted by a minimum of two people. An independent review, followed by a joint comparative review, resulted in confirmation of eligibility. Disagreements were resolved by consensus, and a third person was consulted if there was difficulty reaching a final decision. In addition, hand searches of article reference lists were conducted to ensure that all relevant articles were included.
Data Extraction
For each of the included articles, key information (e.g., level of evidence, participant criteria, intervention description) was extracted. Anna Boone and Rachel Proffitt performed the evaluation and information extraction process (Supplemental Table A.2).
Risk of Bias
Boone and Proffitt independently evaluated each study for risk of bias using the Cochrane risk-of-bias guidelines for multi-group studies (Higgins et al., 2019) and the National Heart, Lung, and Blood Institute (2014) guidelines for single-group studies. The authors then compared findings and discussed any discrepancies until a consensus was reached (Supplemental Table A.3).
Narrative Synthesis
The authors evaluated the final evidence to identify commonalities and differences for final theme development and to evaluate the strength of evidence for each theme (level of certainty). The narrative synthesis followed the U.S. Preventive Services Task Force (2018) guidelines (Supplemental Table A.4).
Results
For this systematic review, 392 articles were retrieved for full-text review. Two authors (AB and RP) reached 100% agreement on article inclusion. Forty-seven articles met the inclusion criteria (see Supplemental Table A.2); 43 studies were related to social participation outcomes, 3 were related to work outcomes, 3 were related to leisure outcomes, and 2 studies were each included in two categories (Figure 1). The emerging themes in social participation were aligned by intervention approach and were categorized into the following overarching approach types: occupation-based approaches, metacognitive strategy training, education and training approaches, impairment-based approaches, and enriched environment approaches. In this review, Bertilsson et al. (2014) reported adverse effects of the client-centered activities of daily living (ADL) intervention group because they scored higher on emotions on the Stroke Impact Scale (SIS). One patient in Dehem et al.’s (2019) study reported shoulder pain, but whether it was related to treatment was unknown. Three participants in Stock et al.’s (2018) study reported shoulder pain. One participant in Thrane et al.’s (2015) study reported shoulder capsulitis from constraint-induced movement therapy (CIMT). The remaining studies did not report any adverse events.
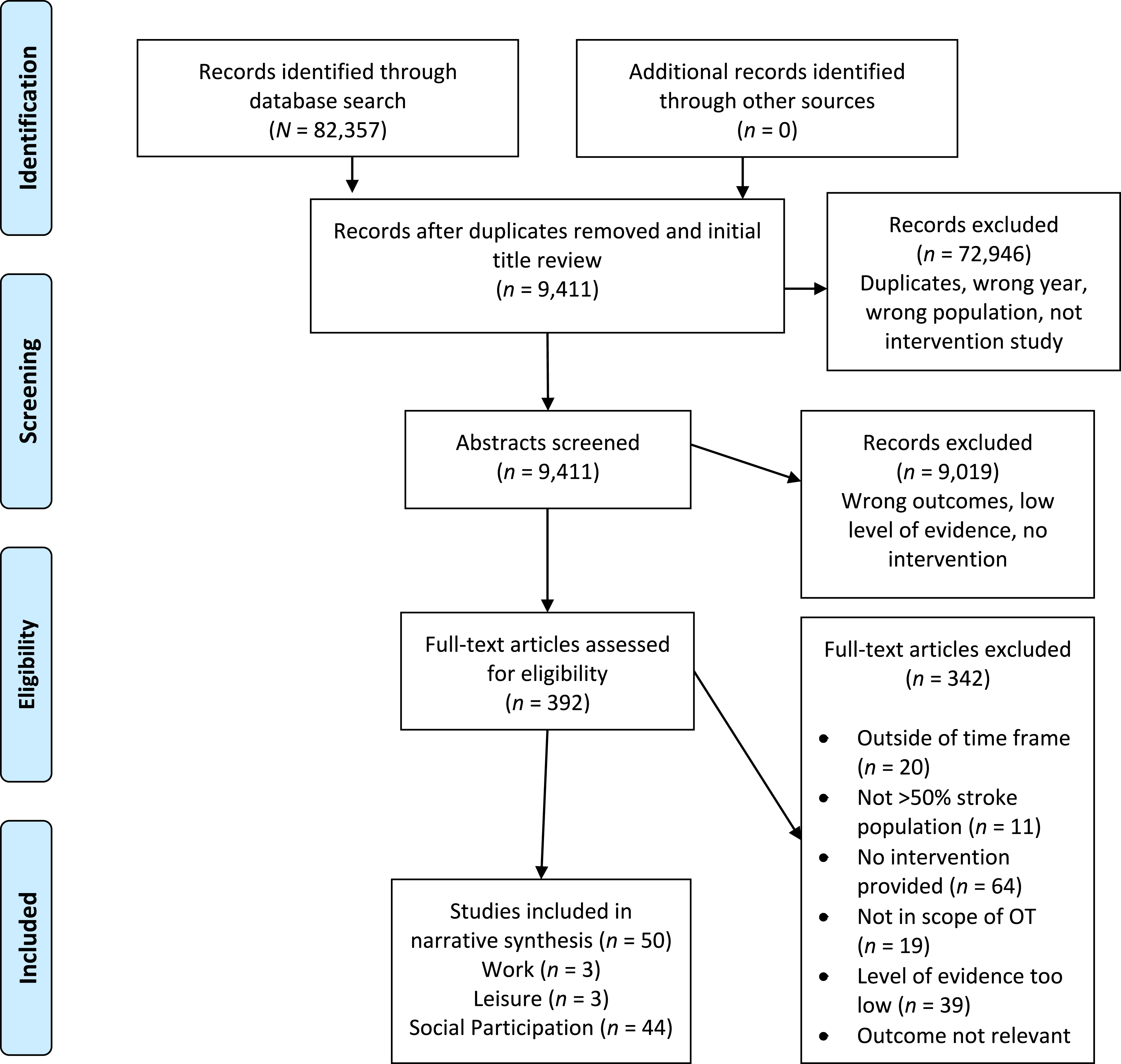
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
Social Participation: Occupation-Based Approaches
Four Level 2b studies (Beinotti et al., 2013; Ho et al., 2016; Shinohara et al., 2012; Tomori et al., 2015) tested occupation-based interventions (i.e., interventions that used occupations as the basis for the intervention, such as gardening, ADL performance) and evaluated social participation outcomes. Because of the limited number of studies available and the inconsistent results, there is low strength of evidence to support this type of intervention.
One Level 2b study (Beinotti et al., 2013) compared a control of conventional therapy with an intervention that included a combination of conventional therapy and horseback riding therapy. No differences were found between the groups in social function on the 36-item Short Form Survey (SF–36) at posttest (p = .53), and both groups improved.
Another Level 2b study (Ho et al., 2016) examined a gardening activity with plants of varying long- and short-term life cycles among people with stroke and found that the short-term plant group demonstrated significantly greater improvement in social role quality of life (p = .015) than the long-term plant group.
A Level 2b study conducted by Shinohara et al. (2012) evaluated a Model of Human Occupation (MOHO)–driven intervention in an inpatient rehabilitation setting. Occupational therapy practitioners administered MOHO assessments to guide intervention choices (i.e., content and structure of occupation-based activities) with a focus on volition, role performance, and changes to the physical environment. When compared with a control intervention (biomechanical approach), the experimental group demonstrated significant improvements in social relationships on the 26-item World Health Organization Quality of Life (QOL–26, Japanese version; p = .000) and had significantly better scores on social relationships than the control group (p = .000); moreover, improvement on the SF–36 was significantly better (at 3 mo postintervention, p = .012).
A Level 2b study conducted by Tomori et al. (2015) evaluated an occupation-based therapy intervention to assess outcomes in social function compared with traditional therapy. The experimental intervention focused on occupation-based practice, and more than two-thirds of treatment time was allocated to occupational practice (e.g., ADLs, cooking, knitting). These authors found no difference between the groups in social functioning (p = .85) as measured with the SF–36. Neither group was significantly different at postintervention (experimental, p = .60; control, p = .44).
Social Participation: Metacognitive Strategy Training
Individual-Focused Interventions
Problem solving
There is low strength of evidence, from 1 Level 1b and 2 Level 2b studies, supporting a metacognitive problem-solving intervention to improve social participation for adults poststroke because of the number of studies and the nonsignificant findings. One Level 1b study (two articles) investigated a metacognitive strategy training intervention and conducted a long-term follow-up (Bertilsson et al., 2014; Guidetti et al., 2015). Metacognitive problem-solving interventions teach the client a global problem-solving approach for everyday activities. The global problem-solving intervention addressed improving ADL performance, with a secondary outcome of social participation (Bertilsson et al., 2014). Compared with usual care, no significant differences were found between the two groups on the SIS Social Participation subscale (p = .72) at the primary study endpoint (3 mo after enrollment) or at the 12-mo follow-up (p = .098; Guidetti et al., 2015).
In addition, an ecosystem-focused therapy that involved a problem-solving approach for people with poststroke depression was compared with standard patient education (Alexopoulos et al., 2012). No difference was found between the groups in social participation as measured with the World Health Organization Disability Assessment Schedule 2.0 (p = .73). Kamwesiga et al. (2018) tested a family-centered, problem-solving F@CE™ intervention that involved a problem-solving “target–plan–perform–improve” approach. No significant differences were found between the intervention and control arms on social participation as measured with the SIS (p = .40).
Cognitive Orientation to daily Occupational Performance
Because of the level of evidence and the lack of significant findings, there is low strength of evidence from 3 Level 2b studies (McEwen et al., 2015; Poulin et al., 2017; Song et al., 2019) for the use of the Cognitive Orientation to daily Occupational Performance (CO–OP) metacognitive strategy training intervention to improve social participation among the stroke population.
McEwen et al. (2015) explored occupational therapy using the CO–OP approach compared with usual outpatient occupational therapy. At 3-mo follow-up, a medium effect was found on social participation (d = 0.05). Poulin et al. (2017) investigated the CO–OP approach compared with computer-based executive function training. Although the CO–OP intervention group did improve according to the Canadian Occupational Performance Measure (COPM; Law et al., 1990; p < .05), no significant differences were found in social participation on the Assessment of Life Habits (LIFE-H; Noreau et al., 2002) either within groups or between groups (p > .05). Song et al. (2019) found that a 4-wk CO–OP approach for upper extremity function was not better than the control (task-oriented approach with no metacognitive component; p = .079). Both groups had significant improvement on community integration as measured by the Community Integration Questionnaire (p < .05).
Group-Based Interventions
There is low strength of evidence from 3 Level 1b studies (Lund et al., 2012; Tielemans et al., 2015; Wolf et al., 2017) for the use of group self-management interventions to improve social participation because of the lack of significant findings. Wolf et al. (2017) explored the efficacy of a 6-wk chronic disease self-management program in comparison with a control intervention. A small effect (d = 0.10) of the intervention was found on social and recreational activities compared with the control group, and a small effect (d = 0.16) was found on social relations for the intervention group.
Two studies were conducted to determine the effectiveness of group Lifestyle Redesign® and self-management interventions on quality of life and social functioning after a stroke (Lund et al., 2012; Tielemans et al., 2015). Lund et al. (2012) found no significant differences in any of the outcome measures, including social functioning, between the Lifestyle Redesign provided by the intervention group in conjunction with a physical activity group and the control group (physical activity group only; p = .63). Tielemans et al. (2015) implemented a self-management program aimed at teaching proactive action strategies within four themes: handling negative emotions, social relations and support, participation in society, and less visible stroke consequences. The control group was an information education group. No significant difference was found between the groups in social participation on the Utrecht Scale for Evaluation of Rehabilitation (USER)–Participation instrument (p = .612).
Social Participation: Education and Training
Client Education
Short term
There is low strength of evidence from 1 Level 1b study (Sabariego et al., 2013) examining the effect of client education programs on outcomes poststroke. The intervention was developed on the basis of the World Health Organization’s International Classification of Functioning, Disability and Health with the client taking part in developing a tailored intervention based on need. After individual development, the intervention was conducted in a small group format over 5 days. The purpose of the study was to allow participants to better understand their diagnoses of stroke and to improve their self-efficacy. No significant difference was found between the intervention and control groups (no p value reported).
Community based with follow-up
There is moderate strength of evidence from 1 Level 1b (Rochette et al., 2013) and 2 Level 2b studies (Geng et al., 2019; Ru et al., 2017) supporting community-based education with a follow-up period to improve social participation outcomes after a stroke.
A transitional care approach to stroke rehabilitation that combined traditional education with transitional care from hospital to home involving additional phone calls and in-home visits was compared with standard client education after discharge from the hospital (Geng et al., 2019). A significant improvement was found in the intervention group compared with the control group after 6 mo in social participation as measured by the SF–36 (p = .003) and in interpersonal relations as measured by the Health Promoting Lifestyle II scale (p < .001). In another study (Ru et al., 2017), a community-based, rehabilitation-appropriate technique involving extensive patient education over a 2-yr period for people with stroke was compared with a control group who received no community-based intervention after a stroke. A significant change was found on the Social Functional Activities Questionnaire postintervention compared with preintervention in the intervention group, but only for those age 50 yr and older (p < .05). A Level 1b study (Rochette et al., 2013) was conducted to determine whether providing health care education could reduce the number of unplanned health care visits, whereas secondary outcome measures looked at quality of life, depression, and life habits. No significant difference was found between the groups in social participation as measured with the LIFE-H (p = .30) or with the Quality of Life Index (p = .47).
Caregiver Education
There is low strength of evidence from 1 Level 1b study (Chinchai et al., 2010) to support the effects of home health care and rehabilitation programs provided for caregivers of people poststroke to improve social relationships. No significant difference was found between the intervention and control groups, and neither group improved in terms of scores on the Social Relationship domain of the World Health Organization Quality of Life scale (p = .293).
Social Participation: Impairment-Based Approaches
Upper Extremity Training
There is moderate strength of evidence from 1 Level 1b study (Shin et al., 2016) supporting occupational therapy combined with virtual reality (VR) for upper extremity function and social participation (SIS subdomain). The group who received the VR intervention that used a wearable glove paired with computer games had significantly better Social Participation scores than the control group (p = .02).
There is low strength of evidence from 1 Level 1b study (Lewthwaite et al., 2018) to support an accelerated skill acquisition program–based task-oriented approach to improve social participation. No significant differences were found between the intervention and control groups on the SIS Social Participation subscale (p = .32).
There is low strength of evidence from a Level 1b study (Zheng et al., 2015) that VR combined with repetitive transcranial magnetic stimulation (rTMS) improves social function for people with upper extremity dysfunction poststroke. No significant difference was found in social functioning as measured with the SF–36 after a VR intervention paired with rTMS (p > .05) for the intervention group, and no difference was found when compared with a control group (p > .05).
Because of inconsistent results, there is low strength of evidence from 3 Level 2b studies (Park et al., 2019; Shin et al., 2015; Şimşek & Çekok, 2016) to support a VR upper extremity intervention to improve activity and participation for adults with upper extremity dysfunction after a stroke. Park et al. (2019) found significant improvement for upper extremity function; however, no significant improvement was found between the intervention and control groups for activity and participation. Shin et al. (2015) found that a game-based (VR) rehabilitation intervention in addition to an occupational therapy intervention led to significant improvement in role limitations because of physical problems compared with the control group (p = .031). In Şimşek and Çekok’s (2016) study, one group of patients with subacute stroke received Nintendo Wii™–based balance and upper extremity training, whereas the other group received neurodevelopmental treatment and Bobath treatment for ADLs and quality of life. Both groups improved, and no significant difference was found between groups (p = .30).
There is low strength of evidence from 3 Level 2b studies (Lin et al., 2009; Stock et al., 2018; Thrane et al., 2015) to support long-term effects of CIMT to improve social participation for people poststroke. CIMT was used as an intervention 6 mo after stroke compared with 28 days poststroke (Stock et al., 2018; Thrane et al., 2015). In both studies, no statistical difference was found between groups at 6 mo on the SIS Social Participation subscale (p > .05, Stock et al., 2018; p = .919, Thrane et al., 2015). In another study, Lin et al. (2009) looked at the effectiveness of CIMT compared with traditional occupational therapy intervention and found no significant difference between the groups on the SIS Social Participation subscale (p = .25).
Because of the level of evidence and inconsistent findings, there is low strength of evidence from 2 Level 2b studies (Dehem et al., 2019; Wu, Yang, et al., 2012) to support the use of robotic and exoskeleton devices for improving social participation for people poststroke. In 1 study, Dehem et al. (2019) tested an upper extremity robotic-assisted therapy combined with conventional therapy and conventional therapy only focused on motor rehabilitation during early stroke rehabilitation. At 6-mo poststroke, a significant improvement was found in the intervention group compared with the control group for social participation (p = .01). In another study, Wu, Yang, et al. (2012) used the Bi-Manu-Track robot-assisted arm trainer. Participants practiced identical tasks with each arm simultaneously as well as a variety of bilateral functional tasks, and they received feedback for results and performance. No statistically significant difference was found on the SIS Social Participation subscale between the intervention and control groups (p = .35).
There is low strength of evidence from 1 Level 2b study (Page et al., 2013) to support an electromyography-controlled brace paired with task training to improve social participation for people poststroke. No significant improvement was found in the intervention group compared with the control group for social participation (p = .49).
Cognitive Training
There is moderate strength of evidence from 1 Level 1b study (Liu et al., 2019) to support the use of group-based cognitive–behavioral therapy (CBT) combined with task-oriented balance training to reduce fear of falling. The study showed a significant improvement in community integration when compared with a control group (p = .016).
There is low strength of evidence from 1 Level 2b study (Faria et al., 2016) to support a VR-based simulation of ADLs set in a virtual city. This intervention was not significantly better than cognitive training in terms of social participation because both groups improved (p = 1.0).
There is low strength of evidence from 1 Level 2b study (van de Ven et al., 2017) supporting a web-based, self-directed cognitive intervention related to memory, attention, and reasoning to improve social participation. Van de Ven et al. (2017) found no significant improvement in social participation as measured with the USER–Participation instrument (p = .26).
There is low strength of evidence from 1 Level 2b study (Kootker et al., 2017) to support CBT in addition to traditional outpatient occupational therapy to improve social participation levels. Results showed that the intervention had no significant effect on social participation scores (p values not reported).
Visual Scanning Training
There is low strength of evidence from 1 Level 2b study (Crotty et al., 2018) to support a standardized therapy intervention focused on static visual scanning for stroke survivors with homonymous hemianopia training. Crotty et al. (2018) found no significant differences between groups in social functioning as measured by the National Eye Institute Visual Functioning Questionnaire at 7 wk (p = .655) and 3 mo (p = .921) postintervention.
Exercise and Balance Training
Individual intervention
Because of inconsistent findings, there is low strength of evidence from 2 Level 1b studies (Brouwer et al., 2018; Logan et al., 2014) and 1 Level 2b study (Aidar et al., 2016) to support individual exercise and balance training combined with education to improve community integration. In 1 study, Logan et al. (2014) investigated the effect of targeted occupational therapy sessions that included verbal education, handouts, exercises, and outdoor mobility training compared with basic verbal education and handouts over the course of 4 mo. No significant between-groups differences were found in SF–36 social functioning (M difference = 1.24, 95% confidence interval [−6.67, 4.10]). In another study, Brouwer et al. (2018) used an in-home “tune-up” or maintenance therapy intervention to focus on client-centered mobility goals. Subjective Index of Physical and Social Outcome (SIPSO) social integration subscores increased for both the intervention and control groups, indicating no significant differences between the groups at 12 mo (p = .66) and 15 mo (p = .34) postintervention. In a Level 2b study, Aidar et al. (2016) found that regular strength training improved physical strength and health as well as quality of life and social functioning via the SF–36 compared with the control group (p < .05).
Group intervention
There is moderate strength of evidence from 2 Level 1b (Harrington et al., 2010; Stuart et al., 2009) and 1 Level 2b (Holmgren et al., 2010) studies supporting group-based exercise programs to improve social participation. Participants receiving a group-based occupational therapy intervention had higher levels of social functioning as measured with the SIPSO (Harrington et al., 2010), and the intervention group had a statistically significant increase on participant-reported community mobility measures and social participation (p = .001; Stuart et al., 2009). Holmgren et al. (2010) found that the intervention group receiving exercise training and educational information did not significantly improve in social functioning compared with the control group, who received education only (p > .05).
Social Participation: Enriched Environments
Because of the limited number of studies, there is low strength of evidence from 1 Level 2b study (Rosbergen et al., 2019) to support providing an enriched environment (communal sitting in public spaces, stimulating equipment) in combination with tailored individual and group activities (education, physical activity) to improve social participation. The intervention group demonstrated a significant increase compared with the control group in overall activity in communal activity times (p < .001), communal socializing (p = .001), and listening (p = .007).
Work
There is moderate strength of evidence from 1 Level 1b study (Ntsiea et al., 2015) supporting a tailored workplace rehabilitation intervention to improve return-to-work rates for adults poststroke. A tailored intervention for stroke survivors was created according to each participant’s specific functional ability and workplace challenges. At 6-mo follow-up, the intervention group demonstrated a significantly higher return-to-work rate than a control group receiving usual occupational therapy services after stroke (p < .001). After the intervention, participants who returned to work had significantly better quality of life than those who did not.
There is low strength of evidence from 1 Level 2b study (Wu, Chen, et al., 2012) to support CIMT paired with trunk restraint to improve work outcomes. Wu, Chen et al., (2012) compared CIMT with trunk restraint to a control of standard CIMT and a control of usual care. No significant differences were found in terms of improvement in work outcomes between groups (p = .37), and all pairwise comparisons were not significant (p = .88, .24, and .20, respectively) on the combined Work/Leisure subdomain of the Frenchay Activities Index.
Because of the limited number of studies, there is low strength of evidence from 1 Level 2b study (Grau-Sánchez et al., 2018) supporting the use of music- supported therapy in addition to standard occupational and physical therapy to improve work outcomes. When compared with a control group, participants in the treatment group demonstrated greater improvements in productivity (p < .005) as measured by the Work/Productivity subdomain of the Stroke-Specific Quality of Life Questionnaire.
Leisure
There is low strength of evidence from 2 Level 2b studies (Page et al., 2013; Vanroy et al., 2019) supporting the use of devices for a bottom-up motor approach to improve leisure for adults poststroke. Page et al. (2013) used an electromyography-controlled brace on the affected upper extremity combined with bilateral task specific training as the intervention. No significant differences were found on the COPM in performance (p = .43) or satisfaction (p = .23) measures of leisure. Vanroy et al. (2019) conducted a second study to determine whether cycling on a MOTOmed leg trainer combined with education and participant coaching—including goal setting, increasing autonomy, and motivational interviewing—would affect outcomes on the Baecke Questionnaire of Habitual Physical Activity. No significant improvements were found on leisure scores at 12-mo compared with baseline (p = .132) or when compared with a MOTOmed leg trainer group without the addition of coaching (p = .388).
There is low strength of evidence from 1 Level 2b study (Wu, Chen, et al., 2012) to support distributed CIMT paired with trunk restraint to improve leisure outcomes for adults poststroke. Wu, Chen et al. (2012) compared CIMT paired with trunk restraint with both a standard CIMT group and a usual-care control group. No significant differences were found within groups (p = .37) or between groups (ps = .20, .22).
Discussion
The purpose of this systematic review is to report findings evaluating the effectiveness of interventions within the scope of occupational therapy practice to improve social participation, work, and leisure among adults poststroke. Results indicate that a variety of approaches and interventions that can improve social participation fall within the scope of occupational therapy practice. Improvements in social participation, social functioning, or social roles were primarily found in occupation-based studies (McEwen et al., 2015; Shinohara et al., 2012; Wolf et al., 2017). Metacognitive strategy training approaches generally reported good outcomes related to social participation. Additionally, studies that investigated gardening demonstrated positive outcomes (Beinotti et al., 2013; Ho et al., 2016). These approaches are naturally group based and encourage social interactions among participants. Many of the group-based or family-centered approaches also demonstrated positive social participation outcomes.
Despite the traditional work-heavy focus in Western culture, there has been a recent press for renewed work–life balance effort and prioritization of leisure (Sirgy & Lee, 2018). Leisure activities are intrinsically motivating occupations that are not obligatory in nature (AOTA, 2020). In this systematic review, we identified 3 studies addressing work outcomes and 3 studies addressing leisure outcomes from among the literature published from 2009 to 2019. Although this review included only intervention studies within the scope of occupational therapy, it is notable that we looked across several multidisciplinary databases to identify articles. There is a stark mismatch between the value we ascribe to return to work and leisure and the amount of literature to support addressing these outcomes clinically.
Evidence from this systematic review identified no significant differences between groups on leisure outcomes for impairment-based interventions (e.g., leg trainer + coaching, CIMT; Vanroy et al., 2019; Wu, Chen et al., 2012). This finding highlights the importance of moving beyond impairment-based interventions to improve leisure outcomes.
Impairment-based interventions generally had nonsignificant social participation, work, and leisure outcomes. Occupational therapy practitioners should strive to directly address social participation, work, and leisure in their choice of intervention approaches and not assume that those outcomes will inadvertently improve.
For most of the included studies, the primary outcome was not social participation. Most studies used the SF–36, Stroke-Specific Quality of Life questionnaire, or the SIS Social Participation/Function/Role subscales to assess social participation. This measurement approach is woefully inadequate to capture the full construct of social participation. Social participation encompasses community participation, family participation, friendships, intimate partner relationships, and peer group participation. Occupational therapy practitioners and researchers wanting to assess social participation should consider focused measures such as the Patient-Reported Outcomes Measurement Information System social function items (Cella et al., 2010) or the LIFE-H (Noreau et al., 2002). The Occupational Performance History Interview–II (Kielhofner et al., 2001) or an interview-guided assessment such as the COPM (Law et al., 2019) can provide additional details on and goals for social participation that are not captured in a standardized measure.
Choice of assessment is only one component of assessing outcomes. As a construct, social participation is broad, and change very often does not occur in the short time frame of most research studies or rehabilitation encounters. Few of the studies in this systematic review included follow-up measures. Those studies that did reported positive findings (Dehem et al., 2019; Geng et al., 2019; McEwen et al., 2015; Ntsiea et al., 2015; Ru et al., 2017; Shinohara et al., 2012). Researchers are encouraged to consider adding follow-up assessment time points at 3-mo, 6-mo, and 1-yr postintervention for constructs such as social participation, work-related outcomes, and community integration and reintegration. Additionally, in most studies work and leisure were primarily distal, secondary outcomes (with the exception of Ntsiea et al., 2015); more studies are required that evaluate interventions seeking to improve work or leisure as primary outcomes.
Strengths and Weaknesses of the Systematic Review
We conducted this systematic review using best practice methodology. However, it is possible that relevant articles were missed in the search. The potential for publication bias also exists, so unpublished studies may be missing that would provide important information. The moderate risk of bias for those studies included in this review is a limitation. Numerous studies fit the criteria for this review; however, the interventions varied widely, resulting in less ability to group them and find strong strength of evidence to better guide practitioners.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice: Occupational therapy practitioners should strive for occupation-based approaches to improve clients’ social participation after a stroke. Social participation is a subjective construct, and occupational therapy practitioners should consider a variety of assessments, including an occupational interview. Client-driven intervention approaches that promote autonomy and client choice may lead to improved and sustained social participation for clients poststroke. Intentional approaches to intervention and measurement of work and leisure outcomes are critical in building the evidence base for occupational therapy practice.
Conclusion
This systematic review provides low strength of evidence for occupation-based and problem-solving approaches and moderate evidence for group-based approaches to improve clients’ social participation after a stroke. Research shows that interventions targeting social participation are successful in reducing depression, increasing quality of life, and facilitating community reintegration. For this reason, occupational therapy practitioners should be mindful to assess and address social participation when treating people poststroke. Further research is needed to strengthen the evidence for occupational therapy interventions to address social participation, work, and leisure outcomes after a stroke.
Footnotes
*
Indicates studies included in the systematic review.
Acknowledgments
We thank Lauren Alldredge, Susan Cahill, Brianna Carter, Katie Cox, and Deborah Lieberman for their assistance with this project. This project was supported by the American Occupational Therapy Association Practice Improvement and Evidence-Based Practice Divisions.