
Abstract
The authors found evidence to support occupational therapy interventions that align with value-based measures in three outcome areas: functional status, medication reconciliation, and skin integrity.
In 2001, the U.S. Department of Health and Human Services and the Centers for Medicare & Medicaid Services (CMS; 2020a) initiated programs to improve the quality of health care. These programs aimed to assist consumers in making health care decisions by publicly reporting quality data from hospitals, nursing homes, and other health care settings. Value-based programs began to provide monetary incentives to health care systems and providers on the basis of the quality of care given to Medicare beneficiaries (CMS, 2020b). Since 2001, legislation including the Patient Protection and Affordable Care Act (2010; Pub. L. 111-148) and programs such as the Merit-Based Incentive Payment System have continued to fuel CMS’s (2020b) value-based payment and quality strategies to achieve its goal of improving care at the individual and population levels while lowering the cost of health care.
Following these important steps toward promoting the quality of health care, the Improving Medicare Post-Acute Care Transformation (IMPACT) Act (Pub. L. 113-185) was signed into law in 2014. The law was designed to standardize data across postacute care (PAC) settings including skilled nursing facilities, rehabilitation hospitals, home health services, and long-term care hospitals (CMS, 2021). To regulate data, the IMPACT Act mandated the use of a standardized patient assessment tool, Section GG, across PAC settings to promote uniformity of assessment and care. The collection of standardized assessment and quality data supported CMS’s shift to value-based payment, public reporting, and ranking of PAC providers. Ultimately, the IMPACT Act aimed “to improve Medicare beneficiary outcomes through shared-decision making [sic], care coordination, and enhanced discharge planning” (CMS, 2021, para. 2).
Most of the occupational therapy literature related to the IMPACT Act relates to the importance of data collection and advocacy, and the American Occupational Therapy Association (AOTA; 2021) supports practitioners in addressing value-based initiatives. Sandhu et al. (2018) asserted that contributing to quality measures is essential for reimbursement. Other literature (e.g., Giles et al., 2017) has suggested that functional cognition should be part of regular occupational therapy patient assessments for data collected by the IMPACT Act. Kroll and Fisher (2018) provided perspectives on the Continuity Assessment and Evaluation (CARE) Tool, a standardized assessment measuring health and functional status for Medicare patients at acute hospital discharge and admission to and discharge from postacute settings; they discussed the need for further research and advocacy related to the ideal rehabilitation intensity.
This study is Part 2 of a two-part systematic review of the effectiveness of occupational therapy interventions related to the quality and resource use domains of the IMPACT Act (see Lucas Molitor et al., 2022, for Part 1 of the systematic review). In Part 2, we address three IMPACT Act outcome areas identified by CMS (2021): functional status, medication reconciliation, and skin integrity. We used the following operational definitions to guide the review: Functional status: level of ability to perform “specific areas of function (i.e., self-care, mobility, cognition, communication, and bladder continence)” (CMS, 2014, p. 3) Medication reconciliation: identification and review of accurate list of current medications as well as medication-related strategies, including “medication teaching for patients and caregivers [and] development of medication list for patients and their health care providers” (CMS, 2019, p. 11) Skin integrity: degree of development of pressure ulcers, which require prevention strategies, close monitoring, and appropriate treatment (CMS, 2018).
This systematic review of interventions occupational therapy practitioners have provided in these areas can inform practitioners about their effectiveness in order to promote best practice, advocacy, and continued research and ultimately to align practice with current health care and reimbursement systems. The review questions for this study were as follows: What is the effectiveness of occupational therapy interventions to facilitate function, including cognitive performance, among adults? What is the effectiveness of occupational therapy interventions to promote medication management and reconciliation among adults? What is the effectiveness of occupational therapy interventions to improve and maintain skin integrity among adults?
Method
We conducted a systematic review of the available evidence on our review questions using the Cochrane methodology (Higgins et al., 2016) and our operational definitions. Systematic review authors use an organized approach to collect and critically analyze research findings through qualitative synthesis (Portney, 2020). We used this approach to address each of the three review questions.
First, a health science research librarian skilled in database searching conducted a thorough search of the available literature at an academic institution. Databases included CINAHL, Cochrane, MEDLINE, PsycINFO, OTseeker, and Scopus. Databases were searched within “all fields,” and all search terms were exploded, when applicable, to locate as many articles as possible; articles were then limited by publication year and language. We included peer-reviewed articles published between 2009 and 2019 in English that described studies involving adult clients or populations receiving occupational therapy services, used an occupational therapy professional as the interventionist (or member of the intervention team), and addressed the review question. We did not limit our literature search to services provided in PAC settings because we wanted to capture all occupational therapy interventions related to the three outcome areas of the IMPACT Act. We felt that broadening our search to any setting providing services to adult individuals, groups, or populations would allow us to better determine effectiveness and draw conclusions from the available research. Table 1 lists the search terms used for this article.
Key Terms and Search Terms
We used the Oxford Centre for Evidence-Based Medicine (2009) classifications for level of evidence. Articles selected for inclusion described intervention studies providing Level 1b, 2b, and 3b evidence. We excluded systematic reviews and meta-analyses but hand searched the articles they included and screened them for inclusion in our review. Studies included in this review provide evidence at the following levels: Level 1b: well-designed randomized controlled trials (RCTs) Level 2b: prospective cohort studies; lower quality RCTs; or two-group, nonrandomized studies Level 3b: retrospective case–control studies; one-group, nonrandomized pretest–posttest studies; or cohort studies.
In groups of two study authors, we independently screened articles for inclusion on the basis of the study title and abstract and sorted them into three categories: yes, no, or maybe. We then met as a group to compare screening results and discuss any discrepancies between reviewers; for articles the reviewers still disagreed on, we obtained the full text for further review. We obtained full-text articles categorized as yes or maybe and sorted them by review question in a shared file. Next, in groups of two, we independently screened all full-text articles to ensure they met all inclusion criteria. If the two reviewers were unable to reach consensus on inclusion, a third reviewer reviewed the article, and together they reached an agreement on whether to include it in the review. Throughout the screening process, we documented the number of articles and duplicates and the reasons for exclusion, which are presented in Figure 1 (Moher et al., 2009).
Because the search results yielded many relevant articles on functional status, we narrowed the publication date inclusion criterion for this review question to 2015 to 2019 to include only the most up-to-date evidence. The data in Figure 1 reflect the narrowed publication time frame for this review question.
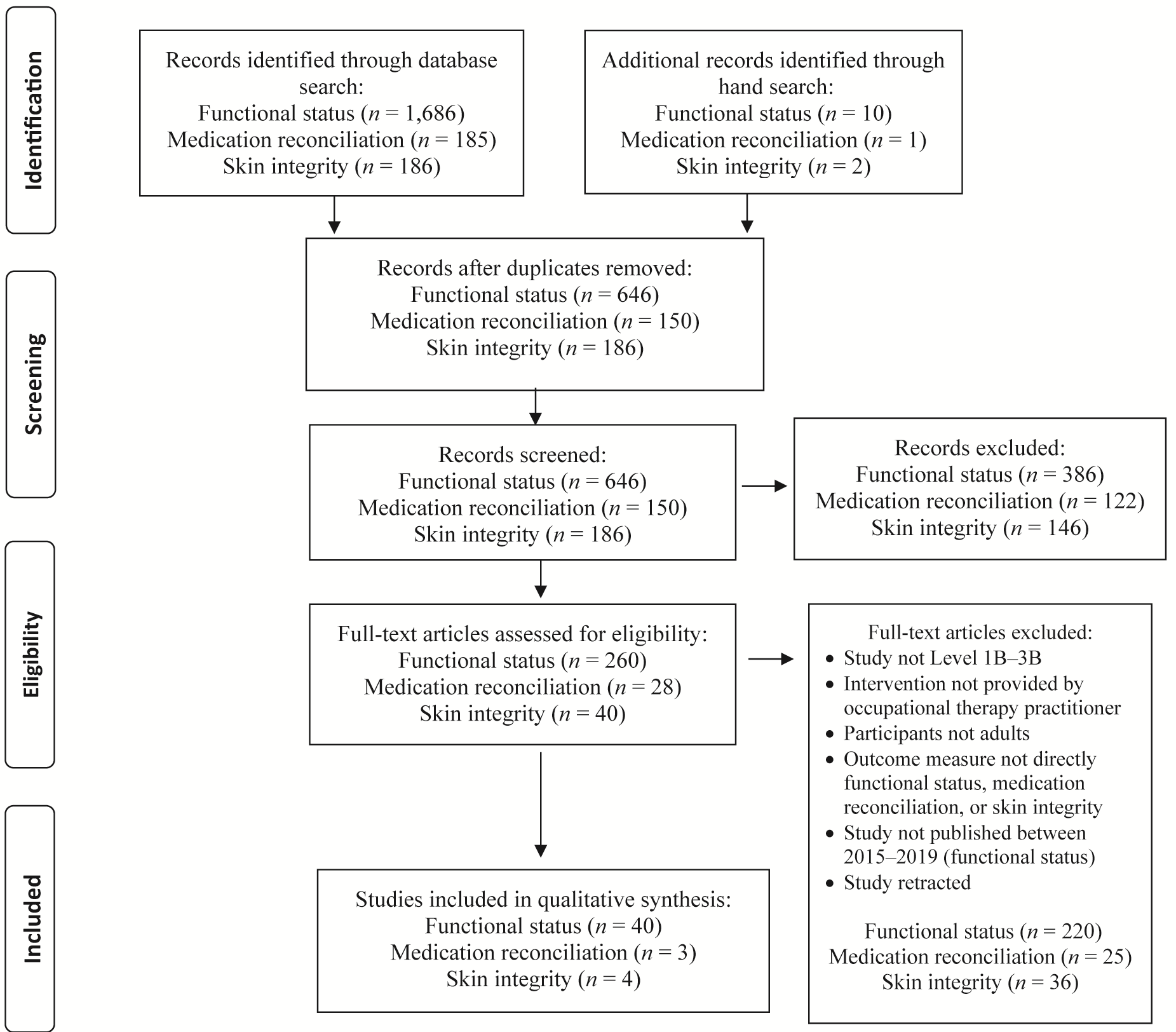
Flow diagram for inclusion and exclusion of studies in the systematic review.
Data Extraction and Quality Assessment
We divided the articles that met the inclusion criteria among all authors and individually extracted information into an evidence table (Supplemental Table A.1, available in the Supplemental Appendix online with this article at https://research.aota.org/ajot). We assessed each article for risk of bias using the format appropriate for the study design (Higgins et al., 2016; National Heart, Lung, and Blood Institute, 2014). To ensure the quality of our results, a second author reviewed the data extraction and assessment of risk of bias; together, the two authors reached an agreement on the level of evidence and risk of bias. When the two authors could not agree, a third author reviewed the article and independently assessed the level of evidence and risk of bias, and the three authors then met to discuss findings and reach an agreement. For each domain of interest, we analyzed the populations, interventions, settings, and outcomes of the studies to establish themes agreed on by all authors. We rated the strength of evidence for each review question and theme on the basis of the study results for each.
We used the U.S. Preventive Services Task Force (2018) recommendations, in combination with our risk-of-bias assessment results, as a guide in determining the strength of evidence in our findings: Strong: includes two or more well-designed and -conducted Level 1a or 1b studies that report consistent results. The findings are not likely to be questioned by the results of future studies. Moderate: includes at least one high-quality study (Level 1a or 1b) or multiple moderate-quality studies (Level 2a, 2b, 3a, or 3b) providing enough evidence to determine health outcomes. Because these studies have small sample sizes, lower quality, or inconsistency in findings across studies, the findings may be questioned in future research. Low: includes few low-level studies with flaws in design or high risk of bias, providing insufficient evidence to assess effects on health outcomes.
Results
The literature search yielded 40 studies for functional status, 3 studies for medication reconciliation, and 4 studies for skin integrity that met the inclusion criteria (see Figure 1). Details of the studies, sorted by research question and theme, can be found in Supplemental Table A.1.
Functional Status
We grouped the 40 articles that addressed functional status into themes according to intervention type and outcome area. Four themes emerged: activities of daily living (ADLs), cognition, functional mobility, and vision.
Activities of Daily Living
We found 33 studies on interventions focused on ADL outcomes for people with various medical conditions. We developed three subthemes based on diagnosis: neurological conditions, musculoskeletal conditions, and other conditions.
Neurological conditions
Twenty-two studies (5 Level 1b, 16 Level 2b, 1 Level 3b) examined ADL interventions for people with a neurological condition, including stroke, multiple sclerosis, traumatic brain injury, median and ulnar nerve injuries, and brain tumor.
In 10 studies, the sole focus of intervention was on functional or task-oriented approaches to promote independence in ADLs. Three studies used a structured program, including a nine-step client-centered ADL process (Guidetti et al., 2015, Level 1b), manual dexterity training adapted from the Arm Ability Training program (Kamm et al., 2015, Level 2b), and the Accelerated Skill Acquisition Program (ASAP; Lewthwaite et al., 2018, Level 1b); approaches used in other studies were self-regulation training (Liu & Chan, 2014, Level 2b) and guided and direct skill training (Skidmore et al., 2017, Level 2b). Five studies looked more broadly at the effectiveness of occupational therapy services compared with a control condition of no occupational therapy (Almhdawi et al., 2016, Level 2b; Sackley et al., 2015, Level 1b; Taule et al., 2015, Level 1b; Trevena-Peters et al., 2018, Level 1b) or impairment-based intervention (Tomori et al., 2015, Level 2b). All but 1 study (Sackley et al., 2015, Level 1b) found statistically significant improvements as a result of occupational therapy interventions; however, in most studies, both the intervention and control groups improved significantly after receiving occupational therapy, with few significant between-group differences.
Twelve studies combined functional ADL occupational therapy intervention with additional intervention strategies, including virtual reality (Chen et al., 2015, Level 2b; Choi et al., 2016, Level 2b; Kim, Cho, et al., 2018, Level 2b; Yoon et al., 2015, Level 2b), electrical stimulation (Kim et al., 2016, Level 2b; Lee, Lin, Wu, et al., 2015, Level 2b), robotic therapy (Kim et al., 2015, Level 3b; Lee et al., 2018, Level 2b), a combination of electrical stimulation and robotic therapy (Lee, Lin, Cheng, et al., 2015, Level 2b), transcranial direct current stimulation (Mortensen et al., 2016, Level 2b), constraint-induced movement therapy (CIMT; Rostami et al., 2017, Level 2b), and modified CIMT (mCIMT) with mental practice (Kim, Yoo, et al., 2018, Level 2b). All studies found significant improvements within groups; however, only 5 studies found significant between-group improvements compared with control groups that received occupational therapy consisting of rote exercise.
In summary, we found an abundance of high-level research on ADL functional interventions for people with neurological conditions, with generally low risk of bias but some inconsistencies in results. Therefore, moderate strength of evidence supports individualized and occupation-based interventions targeting ADL functional outcomes for clients with neurological conditions. Low strength of evidence is available for interventions using structured programs rather than usual functional occupational therapy interventions and incorporating electrical stimulation, robotic therapy, occupation-based CIMT, and mCIMT with mental practice to improve functional outcomes for people with neurological conditions.
Musculoskeletal conditions
Four studies (3 Level 2b, 1 Level 3b) examined ADL interventions for people with a musculoskeletal condition (osteoarthritis or fibromyalgia). Two studies provided assistive device training to aid ADL performance (Amaral et al., 2018, Level 2b; Jame Bozorgi et al., 2016, Level 2b), and two provided psychomotor skill training (Gonzalez Gonzalez et al., 2015, Level 3b; Pérez-Mármol et al., 2017, Level 2b). Although the findings for assistive device training were positive, the studies had small sample sizes. Findings related to ADL performance after psychomotor intervention were inconsistent.
In summary, low strength of evidence was found to support interventions to promote ADL performance in clients with musculoskeletal conditions.
Other conditions
Seven studies (2 Level 1b, 5 Level 2b) were conducted with participants who had a diagnosis other than a neurological or musculoskeletal condition, including weakness in older adults (Imanishi et al., 2017, Level 2b; Liu et al., 2017, Level 2b; Nagayama et al., 2016, Level 2b; Stark et al., 2018, Level 1b), chronic obstructive pulmonary disease (Martinsen et al., 2017, Level 2b), advanced cancer (Pilegaard et al., 2018, Level 1b), and complex conditions (Pellegrini et al., 2018, Level 2b). Two studies (Pilegaard et al., 2018; Stark et al., 2018) incorporated home modifications and compared outcomes to a sham or usual home care control; findings were inconsistent. Three studies (Martinsen et al., 2017; Nagayama et al., 2016; Pellegrini et al., 2018) examined individualized and occupation-based treatment and establishment of goals. Whereas Nagayama et al. (2016) and Pellegrini et al. (2018) found significant improvements after treatment compared with impairment-based and therapist-directed care groups, Martinsen et al. (2017) found no benefit of occupational therapy over standard medical management. Functional ADL training combined with exercise (Liu et al., 2017) and leisure and mobility training (Imanishi et al., 2017) resulted in significant benefits.
In summary, we found low strength of evidence for occupational therapy interventions to promote ADL performance for clients with other conditions.
Cognition
Five studies (1 Level 1b, 2 Level 2b, 2 Level 3b) examined cognitive training interventions, including group interventions (Kaizerman-Dinerman et al., 2018, Level 2b; Reilly & Hynes, 2018, Level 3b), online training (Li et al., 2015, Level 3b), home visits (Callahan et al., 2017, Level 1b), and Cognitive Orientation to daily Occupational Performance (Poulin et al., 2017, Level 2b). Significant improvements were found in recall of daily life goals, efficiency, and strategy use (Kaizerman-Dinerman et al., 2018; Reilly & Hynes, 2018). Home visits did not result in significantly improved cognitive function. Although 2 studies found significant improvement in ADLs and overall occupational performance as a result of cognitive intervention (Kaizerman-Dinerman et al., 2018; Poulin et al., 2017), this was inconsistent with Li et al. (2015), who found that improvements in cognition-specific outcomes did not transfer to functional improvement in medication sorting. In summary, we found low strength of evidence for the use of cognitive interventions to promote functional performance.
Functional Mobility
One Level 2b study (Hashimoto et al., 2015) explored a movement-based intervention to promote functional mobility performance. Community-dwelling participants with Parkinson’s disease were allocated to an intervention group who participated in dance or exercise and a control group who received usual care and no occupational therapy intervention. Participants who received the 14-wk dance intervention showed significant improvements in functional mobility.
In summary, because this was a single study with a small sample, low strength of evidence is available for functional mobility interventions to improve functional status.
Vision
One Level 1b study (Deemer et al., 2017) provided a visual intervention to improve functional status. In a sample of older adults with macular degeneration and mild depression, the researchers compared behavioral activation combined with low vision rehabilitation provided by an occupational therapist to supportive therapy consisting of in-home visits from a social worker or counselor. The behavioral activation group showed significant within-group increases in inside-the-home and outside-the-home activity participation and significant differences compared with the supportive therapy group.
In summary, moderate strength of evidence supports the use of visual interventions to promote functional status.
Medication Management and Reconciliation
Three articles (2 Level 1b, 1 Level 2b) addressed medication management and reconciliation. In a small Level 2b study, Schwartz and Smith (2016) compared one 30-min occupational therapy session based on the Integrative Medication Self-Management intervention to a 30-min general medication management education session delivered by an occupational therapist for people with a chronic health condition. Half of the intervention participants experienced a significant improvement in medication adherence. In a large RCT, Shimada and colleagues (2018, Level 1b) compared individualized and group occupational therapy to group occupational therapy alone to promote medication adherence among people with schizophrenia or schizoaffective disorder. Individualized therapy consisted of goal-oriented motivational interviewing, self-monitoring, crafts, psychoeducation, and discharge planning. The researchers also completed a 2-yr follow-up study (Shimada et al., 2019, Level 1b). Both studies found significant improvements in medication adherence for the intervention groups.
In summary, strong strength of evidence supports individualized occupational therapy to facilitate medication adherence.
Skin Integrity
Four studies (1 Level 1b, 1 Level 2b, 2 Level 3b) examined occupational therapy interventions to promote skin integrity by addressing pressure ulcers. A pressure ulcer prevention program (PUPP) or initiative (PUPI) was used in all four studies. Carlson et al. (2019, Level 1b) studied the effectiveness of a 12-mo lifestyle-based PUPP in reducing the incidence of medically serious (Stage 3 or 4) pressure ulcers. Similarly, Cobb et al. (2014, Level 3b) implemented a PUPI and analyzed results retrospectively. Martin et al. (2017, Level 2b) and Scovil et al. (2019, Level 3b) studied prevention programs in which occupational therapy was part of an interprofessional team; Martin et al. compared the prevalence of pressure ulcers among hospital inpatients before and 1 yr after implementing a PUPP, whereas Scovil and colleagues used a retrospective chart review with pre–post comparison to study pressure ulcer incidence, location, stage, and prevalence. Results were mixed across studies and in general did not show significant improvements in skin integrity.
In summary, low strength of evidence because of inconsistent findings is available regarding the use of pressure ulcer prevention interventions by occupational therapy practitioners, especially if they are the only treating health care provider.
Discussion
The purpose of this study was to determine the current state of evidence related to three outcome areas of the IMPACT Act: functional status, medication reconciliation, and skin integrity. For people with neurological conditions, moderate strength of evidence supports individualized interventions to promote ADL outcomes. Considerable evidence indicates that functional status can improve after interventions that both are individualized to meet the distinct factors of each client and reflect a task-oriented and occupation-based approach, as opposed to impairment- and exercise-focused approaches. This finding was not surprising and reflects what is currently known about task-oriented training (Arya et al., 2012; Rensink et al., 2009; Wolf & Nilsen, 2015). A task-oriented (or task-specific) approach promotes client engagement in active, repeated practice to relearn motor skills they require for engagement in meaningful occupations (Hubbard et al., 2009). Such interventions involve motor and sensory demands, pose present and ongoing challenges (e.g., using the just-right approach), and require dedicated practice of skills to reach client-selected goals.
Less evidence is available for interventions other than individualized task-oriented approaches that aim to promote functional outcomes among people with neurological conditions, including mCIMT with mental practice, electrical stimulation, robotic therapy, or physical exercise through virtual reality and structured programs. Because our review included evidence only from interventions carried out by an occupational therapy practitioner, the conclusion of low strength of evidence for use of these interventions to support ADLs for people with neurological conditions differs from the evidence presented in the current guidelines for practice with adults with stroke, which include interventions that are within the scope of occupational therapy practice but may have been conducted by another rehabilitation professional (Wolf & Nilsen, 2015). In the practice guidelines, however, the outcome of focus was motor skill development, rather than functional performance; we excluded research reporting outcomes from interventions to promote isolated motor or sensory skills.
For people with musculoskeletal and other conditions, there was less evidence available and inconsistencies among studies, which limited the ability to draw strong conclusions. Studies of assistive device training to support ADL performance for people with musculoskeletal conditions showed positive results, but these studies had small sample sizes. A systematic review by Roll and Hardison (2017) explored the effectiveness of occupational therapy interventions for adults with upper extremity musculoskeletal conditions. They concluded that very few studies examined occupation-based interventions, indicating a need for research in this area. This is consistent with the findings of this systematic review, which were limited to occupational therapy intervention to support ADL performance among people with musculoskeletal conditions. For other conditions, the available evidence was again limited, and findings of available studies were inconsistent to support individualized occupational therapy intervention over impairment-based or medical management for improving ADLs. Small studies did show promise for functional ADL training combined with exercise and mobility training.
We found little evidence in the occupational therapy literature base to support interventions to improve functional status related to cognition, functional mobility, and vision. We excluded some studies on these topics because they did not report a link to function consistent with AOTA’s recommendation for the Choosing Wisely campaign that cognitive interventions have a direct application to occupational performance (Gillen et al., 2019). Our literature search found articles describing studies that used paper-and-pencil assessments (e.g., the Montreal Cognitive Assessment) to measure functional status without indicating how the results were related to increased, decreased, or no change in functional status; we excluded these studies from the review.
Strong strength of evidence supports a combination of individualized and group occupational therapy interventions to facilitate medication management and promote adherence. The tasks of managing and reconciling medications can be complex, and practitioners must tailor intervention to clients’ contexts, skills, and preferences. Although our findings on this topic are aligned with and support best-practice recommendations within the profession (AOTA, 2017), the scarcity of research we found is consistent with the observations of other researchers (Schwartz & Smith, 2017). Incorporating medication reconciliation and management into interventions is within the occupational therapy scope of practice, and research should focus on the outcomes of these interventions, especially as they relate to function.
Little has been published regarding occupational therapy interventions related to skin integrity, and inconsistencies among existing studies result in low strength of evidence for these interventions. One Level 2b study showed significant improvements, but the other 3 (1 Level 1b and 2 Level 3b) did not. The study designs, variations in interventions, and inconsistent findings prevent firm practice recommendations. Despite the extensive knowledge base related to skin integrity (Garber, 2016), recent occupational therapy research on this topic is sparse. What we did find supports the efficacy of staff training, assessment of risk, and frequent skin monitoring to prevent the development of pressure ulcers in postacute settings. Future research should examine outcomes of manualized programs (Blanche et al., 2011) and of collaborative interventions that incorporate an interprofessional team.
Strengths and Limitations
This systematic review of research relating occupational therapy interventions to the value-based outcomes of functional status, medication reconciliation, and skin integrity can help promote public awareness and the perceived importance of the profession. Our team of five coauthors provided varied perspectives and used a system of checks and balances during the review process, ensuring consistency and rigor. Because the intent of this study was to answer review questions specific to outcome areas of the IMPACT Act, not all findings may be relevant in all practice delivery settings. Additional limitations are the inclusion only of articles published in English and the fact that few articles met the inclusion criteria for two of the review questions.
Implications for Occupational Therapy Practice
Occupational therapy practitioners should actively review and advocate for health care policy and legislation that affect patients and the profession. Additionally, by conducting assessments and reporting quality-based measures related to functional status (including cognition), medication reconciliation, and skin integrity, practitioners facilitate justification for and reimbursement of occupational therapy services. The findings of this study support the following recommended interventions for occupational therapy practice: To promote functional status related to ADLs, practitioners should routinely incorporate interventions that are individualized, occupation focused, and goal based. Behavioral activation combined with low vision rehabilitation should be considered to promote inside-the-home and outside-the-home activity participation for people with macular degeneration. Practitioners should consider providing a combination of individualized and group interventions to promote medication adherence. As practitioners provide services related to functional status, medication reconciliation, and skin integrity, they should consider the evidence provided in this review, in combination with their experience, their professional reasoning, and the client’s goals, to promote best practice.
Conclusion
Much of the occupational therapy literature related to the IMPACT Act has focused on advocacy and policy rather than research findings related to this legislation. We foresee that the reporting of value-based outcomes will extend far into the future. Research studies that aim to test novel interventions should measure occupation-based outcomes to support occupational therapy practitioners in incorporating evidence-based research findings into their practice. Such evidence is necessary for our profession to show that the interventions we use in practice promote quality of life and facilitate occupational performance. Continued advocacy for the value of occupational therapy is an ongoing need within the profession and to the public. The findings of this review are a step toward aligning these perspectives and promoting the value of occupational therapy interventions in supporting quality outcomes.
Supplemental Material
Supplementary material for Occupational Therapy and the IMPACT Act: Part 2. A Systematic Review of Evidence for Functional Status, Medication Reconciliation, and Skin Integrity Interventions
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.049324.pdf for Occupational Therapy and the IMPACT Act: Part 2. A Systematic Review of Evidence for Functional Status, Medication Reconciliation, and Skin Integrity Interventions by Diana R. Feldhacker, Whitney Lucas Molitor, Lou Jensen, Helene Lohman and Angela M. Lampe in The American Journal of Occupational Therapy
Footnotes
*
Indicates articles included in the systematic review.
Acknowledgments
All authors participated in the conceptual design of the study, engaged in data collection, and were involved in drafting and editing of the manuscript. None of the authors declare competing financial interests. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.