
Abstract
This systematic review highlights evidence to support that occupational therapy interventions delivered via telehealth are similarly effective as those delivered face-to-face, especially for neurological and pain conditions.
With changing health care environments and policies, demands for health care services, including occupational therapy, to adopt a telehealth service delivery mechanism are increasing. Telehealth is “the use of electronic information and telecommunications technologies to support and promote long distance clinical health care, patient and professional health-related education, public health, and health administration” (Health Resources and Services Administration, n.d., para. 3). The use of telehealth has been prompted by advancing technologies and other social determinants that add increasing complexity to people’s ability to access needed health care, such as transportation, finances, health professional shortages in rural and underserved areas, and cultural barriers (American Occupational Therapy Association [AOTA], 2013).
Before the coronavirus disease 2019 (COVID-19) pandemic, which is when this systematic review was initiated, interest in telehealth as a viable approach for delivery of occupational therapy services was developing (Cason & Jacobs, 2014). This interest was evidenced by an occupational therapy position paper (AOTA, 2013) and bills introduced in Congress (e.g., CONNECT for Health Act, 2019a, 2019b) to include telehealth coverage for therapy under Medicare Part B, although these bills were not passed. Concurrently, in some states Medicaid payment for occupational therapy services delivered using telehealth was a covered benefit. However, data on Medicaid state adoptions of telehealth for occupational therapy practitioners are inconsistent and unclear (Abbott-Gaffney, 2018).
After data were collected and analyzed for this review, COVID-19 became a public health emergency (PHE), and the use of telehealth (e.g., remote video, virtual check-in, telephone assessment) was accelerated, with new allowances on a temporary emergency basis to allow intervention with social distancing for many previously uncovered services, including occupational therapy. These allowances provided payment for outpatient therapy services via telehealth under Medicare Part B (Centers for Medicaid & Medicare Services [CMS], 2020a). States and some private insurers also made provisions to pay for therapy provided via telehealth as a result of the national emergency (AOTA, 2020b, 2020c). Before this PHE, only certain health practitioners, such as physicians, physician assistants, and nurse practitioners, were reimbursed through Medicare for interventions provided via telehealth (CMS, 2020b).
With increasing evidence regarding the efficacy and feasibility of telehealth services, it is imperative to synthesize the existing telehealth evidence to examine the effectiveness of interventions and inform practitioners and reimbursement entities. Hung Kn and Fong (2019) systematically examined the effectiveness of rehabilitation interventions provided by occupational therapy practitioners via telehealth. Although they noted general positive effects for telehealth interventions, the evidence to support intervention effectiveness was insufficient because of the lack of rigor in study designs. Moreover, their review did not include services provided by occupational therapy on an interdisciplinary team, nor did it consider the breadth of interventions within occupational therapy’s scope of practice, including health promotion, disease prevention, and other wellness strategies. Therefore, as a result of the recent increase in the need for, delivery of, and research on telehealth interventions, an updated systematic review was warranted. The specific research question was “What is the effectiveness of occupational therapy interventions, when provided using telehealth as the mode of service delivery, for occupation-based outcomes?”
Method
Search Strategy
This systematic review was conducted using the Cochrane methodology (Higgins et al., 2016) and followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews (Moher et al., 2009). Search terms (Supplemental Table A.1 in the Supplemental Appendix, available online with this systematic review at https://research.aota.org/ajot) were established by four of the researchers (Diana R. Feldhacker, Vanessa D. Jewell, Marion Russell, Helene Lohman) in conjunction with a health science librarian. These terms were derived from the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; OTPF–3; AOTA, 2014) to reflect occupational therapy’s scope of practice. Searches were conducted in CINAHL, SAGE, Cochrane, MEDLINE, PsycInfo, OTseeker, and OT Search.
Eligibility Criteria
Articles were included in the review if they were peer reviewed, written in English, published between 2009 and 2019, and included the population of recipients of telehealth services, occupational therapy intervention, and occupational outcomes within the scope of occupational therapy practice. The Oxford Centre for Evidence-Based Medicine (OCEBM; 2009) levels of evidence were used to classify levels of evidence. Articles that used an intervention (Level 1b, 2b, and 3b evidence) were included: ▪ Level 1b: well-designed randomized controlled trials (RCTs) ▪ Level 2b: prospective cohort studies; lower quality RCTs; two-group nonrandomized studies ▪ Level 3b: retrospective case–control studies; one-group, nonrandomized pretest–posttest studies; cohort studies.
Articles reporting a systematic review or meta-analysis (Levels 1a, 2a, and 3a) were collected for hand search purposes only but were not otherwise included in the review. Data from conference abstracts, presentations, non–peer-reviewed literature, Level 4 or 5 studies, dissertations, white papers, Delphi reviews, unpublished papers, or psychometric studies were excluded.
The intervention approaches examined were those provided by occupational therapy, as the only intervening discipline or as part of an interdisciplinary team, and focused on outcomes related to occupational therapy’s scope of practice. Outcomes were defined using the OTPF–3 (AOTA, 2014) and included activities of daily living (ADLs), instrumental activities of daily living (IADLs), rest and sleep, education, work, play, leisure, and social participation. Interventions must have been provided to service recipients of occupational therapy across the lifespan using telehealth, as defined by the World Health Organization and International Telecommunications Union (2022): “delivery of health care services, where patients and providers are separated by distance . . . [using] information and communication technology” (p. v).
Procedure and Data Extraction
In November 2019, Diana R. Feldhacker, along with a trained doctoral student research assistant, Sadie Jung LeSage, conducted the searches in collaboration and consultation with a health science librarian with expertise in completing systematic review searches. Searches were conducted using terms and databases outlined earlier. Databases were searched in “all fields,” and all search terms were exploded, where applicable, to locate as many articles as possible. After duplicates were removed, at least two researchers independently reviewed the titles and abstracts of search results. Using the inclusion and exclusion criteria, each article was given a rating of yes, no, or maybe. Ratings were compared between reviewers, with discussion among the entire research team regarding any discrepancies to reach consensus for inclusion. Full texts were obtained for any articles marked yes or maybe. As noted earlier, systematic reviews and meta-analyses were not included, but hand searches were completed of each review or meta-analysis that resulted from the search, and full texts of relevant articles were gathered if they were not already included. In addition, hand searches of three journals related to occupational therapy and telehealth, Occupational Therapy Journal of Research, American Journal of Occupational Therapy, and International Journal of Telerehabilitation, were completed for the publication year 2019, and any relevant full texts were collected. These journals were chosen because of their history of publishing related content. Finally, a Scopus search of known occupational therapy telehealth researchers yielded 4 additional articles.
After collection of full-text articles, at least two researchers completed a second independent screening of full texts using the inclusion criteria and rating each article as yes, no, or maybe. Disagreements were addressed by involving the entire research team in a discussion to reach a consensus. Likewise, all articles marked maybe were discussed and analyzed by the entire research team to determine consensus on inclusion or exclusion.
Once agreement was reached on all articles that were deemed to meet the inclusion criteria, they were divided among the authors, and key information from the final articles was compiled into an evidence table (Supplemental Table A.2 in the Supplemental Appendix) following AOTA’s (2020a) Guidelines for Systematic Reviews. Risk of bias was assessed for each article using Higgins et al. (2016) and the National Heart, Lung, and Blood Institute (2014) guidelines for controlled and noncontrolled studies, respectively. Risk-of-bias results are included in the evidence table (see Supplemental Table A.2). In instances in which there was uncertainty in assigning risk of bias, a second author reviewed the article, data extraction, and risk-of-bias assessment. The two researchers then engaged in a discussion until an agreement on the ranking was established. Extracted information in the evidence table was analyzed on the basis of the population, intervention, setting, and outcomes and was synthesized into themes that were agreed upon by the entire research team. Figure 1 contains the flow diagram for study inclusion and exclusion.
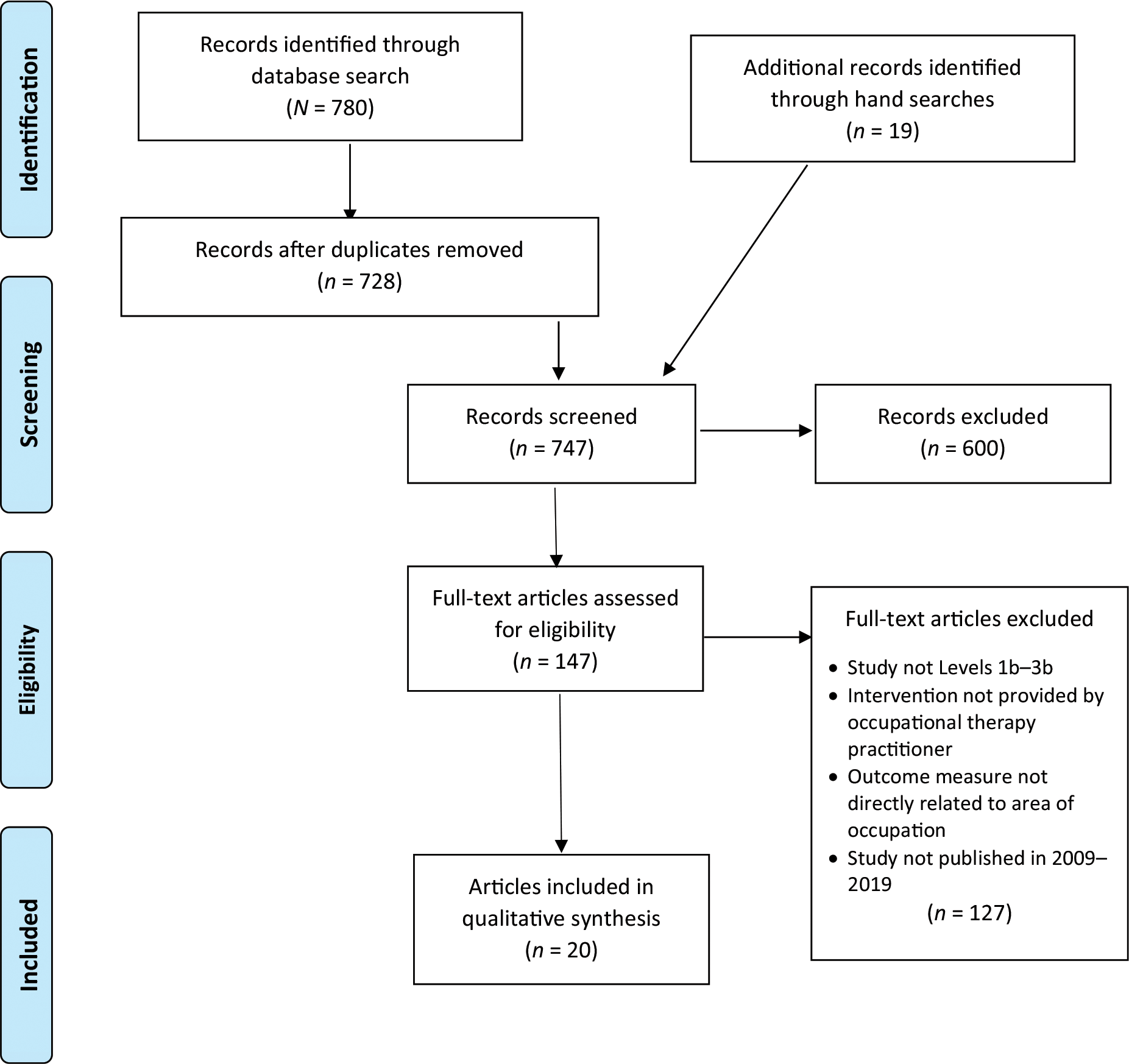
Flow diagram for inclusion and exclusion of studies in the systematic review.
Analysis
Each theme was analyzed for strength of evidence using study design, findings, and risk of bias as recommended by AOTA (2020a) guidelines, which are based on the U.S. Preventive Services Task Force (2018) guidelines. Strength of evidence was rated as follows: ▪ Strong: Includes 2 or more Level 1a or 1b studies that report consistent results. Studies are well designed and well conducted. Results are unlikely to be called into question by the results of future studies. ▪ Moderate: Includes at least 1 Level 1a or 1b high-quality study or multiple moderate-quality studies (Level 2a or 2b, Level 3a or 3b). Evidence is sufficient to determine health outcomes, but there may be issues with the number, size, or quality of the studies or inconsistency in the findings. ▪ Low: Includes a small number of low-level studies. Evidence is insufficient to assess effects on health outcomes because of a limited number of studies, flaws in design or methodology, or inconsistency.
Results
The initial database searches resulted in the identification of 780 articles. After removal of duplicates, 728 articles remained. An additional 19 articles were identified through hand searches. In total, 747 abstracts were screened for inclusion criteria, and 600 articles were excluded. We assessed 147 full-text articles for eligibility; 20 met the inclusion criteria and were included in this systematic review (see Figure 1). The final qualitative synthesis of occupational therapy interventions for recipients of telehealth to address occupational outcomes included 8 Level 1b RCTs, 9 Level 2b studies, and 3 Level 3b studies (see Supplemental Table A.2).
The final 20 articles were evaluated for level of evidence, study design, risk of bias, participants, study setting, intervention and control, outcome measures, and results, including significance of the findings. All included studies were assessed for risk of bias using the methods described previously. A risk-of-bias table was constructed based on the AOTA (2020a) guidelines. Risk-of-bias results for controlled and noncontrolled studies are included in Supplemental Table A.2.
When articles were viewed as a collective whole, the results indicated that telehealth services were used to address a variety of occupational performance issues, including those related to strength, balance, pain, cognition, mobility, motor control, dexterity, educational performance, quality of life, ADLs, IADLs, caregiver stress, depression, fatigue, and overall activity participation and occupational performance, among others. Interventions were provided across the lifespan for children (n = 5) and adults (n = 15) with a variety of conditions. Studies included examination of occupational therapy by both a sole provider (n = 9) and as part of an interprofessional team (n = 11) along with dieticians, nurses, pharmacists, physical therapists, psychologists, social workers, and speech-language pathologists.
Examined collectively, all 20 studies found statistically significant improvements in areas of occupational performance and associated client factors with use of telehealth interventions. The results indicated strong strength of evidence with low to moderate risk of bias supporting occupational therapy interventions for recipients of telehealth to address outcomes within the scope of occupational therapy practice. Several studies found no statistically significant differences between groups when comparing telehealth with face-to-face therapy interventions but did demonstrate statistically significant within-group improvements. After analysis of all studies, four main themes were identified and organized by condition: neurological (n = 9), pain (n = 3), developmental disorders (n = 4), and conditions not otherwise specified (n = 4). Further details of interventions are provided in the discussion of each theme and in Supplemental Table A.2.
Neurological Conditions
Nine studies included participants with neurological conditions. There were 6 Level 1b, 1 Level 2b, and 2 Level 3b studies; 5 had a low risk of bias, and 4 had a moderate risk of bias (see Table A.2). Five involved an adult neurological population with stroke (Chen et al., 2017, Level 1b; Dodakian et al., 2017, Level 3b; Kamwesiga et al., 2018, Level 2b; Linder et al., 2015, Level 1b; Wolf et al., 2015, Level 1b), and 1 each involved adults with multiple sclerosis (Finlayson et al., 2011, Level 1b), dementia (Gitlin et al., 2010, Level 1b), and spinal cord injury (Yuen, 2013, Level 3b). One included a pediatric neurological population of children with acquired brain injury (Baque et al., 2017, Level 1b).
Telehealth approaches varied by study and included therapist remote instrument monitoring (Chen et al., 2017, Level 1b; Linder et al., 2015, Level 1b), live videoconferencing (Dodakian et al., 2017, Level 3b; Finlayson et al., 2011, Level 1b; Yuen, 2013, Level 3b), web-based platforms (Baque et al., 2017, Level 1b), and telephone or text message delivery (Gitlin et al., 2010, Level 1b; Kamwesiga et al., 2018, Level 2b; Wolf et al., 2015, Level 1b). Interventions provided by occupational therapy practitioners addressed a variety of outcomes within occupational therapy’s scope of practice: quality of life, overall occupational performance, functional mobility, ADLs, movement function, psychosocial function, strength, balance, caregiver stress, fatigue and energy conservation, and behavior problems.
All 9 studies demonstrated statistically significant improvements in telehealth intervention groups for at least one outcome of interest. Level 1b studies with low and moderate risk of bias demonstrated statistically significant improvements for people with neurological conditions who received telehealth occupational therapy interventions. These interventions included remote neuromuscular electrical stimulation for biofeedback to improve ADLs, balance, and caregiver stress (Chen et al., 2017); web-based upper limb training to increase strength (Baque et al., 2017); environmental modifications and caregiver training to improve patient behaviors and caregiver psychosocial function (Gitlin et al., 2010); robotic upper extremity training to improve psychosocial function (Linder et al., 2015) and movement functions (Wolf et al., 2015); and group-based teleconferences to improve energy conservation (Finlayson et al., 2011).
These findings are consistently supported by significant findings in Level 2b and 3b studies for occupational performance, ADLs, movement function, and psychosocial function through online game-based and problem-solving training (Dodakian et al., 2017; Kamwesiga et al., 2018) and videoconference problem-solving and assistive device training (Yuen, 2013). Inconsistent findings were reported for outcomes of quality of life (Finlayson et al., 2011). Overall, strong strength of evidence supports the use of telehealth approaches for occupational therapy interventions provided to people with neurological conditions.
Pain Conditions
Three studies included participants with pain conditions. Two were Level 1b, and 1 was Level 2b. Two studies had a moderate risk of bias, and 1 article had a high risk of bias (see Table A.2). Telehealth approaches varied among studies and included web-based platforms (Cottrell et al., 2019, Level 2b), telephone (Sandsjö et al., 2010, Level 1b), and remote supervision of mobile applications (Larsman et al., 2010, Level 1b). Interventions provided by practitioners included nonsurgical pain management (Cottrell et al., 2019, Level 2b) and myofeedback training (Larsman et al., 2010, Level 1b; Sandsjö et al., 2010, Level 1b) and addressed a variety of outcomes, including quality of life, IADLs, pain, and psychosocial function.
All 3 studies demonstrated statistically significant improvements in telehealth intervention groups for pain or pain-related disability as an outcome measure (Cottrell et al., 2019, Level 2b; Larsman et al., 2010, Level 1b; Sandsjö et al., 2010, Level 1b). One Level 2b study (Cottrell et al., 2019) found no significant difference in one pain severity subdomain or in quality of life from pre- to posttreatment. However, this lack of improvement was noted for both telehealth and conventional face-to-face interventions; thus, drawing conclusions regarding their effectiveness in relation to telehealth is not possible. In addition, this study demonstrated high risk of bias, so the results should be viewed with caution. Overall, intervention studies provided by occupational therapy practitioners to address pain indicated strong strength of evidence supporting interventions for recipients of telehealth focused on outcomes within the scope of occupational therapy.
Developmental Disorders
Four studies included people with developmental disorders, including general learning delays, cerebral palsy, and autism spectrum disorder. Three studies were Level 2b, and 1 was Level 3b. Three studies had low risk of bias, and 1 had moderate risk of bias (see Table A.2). Telehealth approaches were similar and included virtual tele- or videoconference sessions (Criss, 2013, Level 3b; Ferre et al., 2017, Level 2b; Langbecker et al., 2019, Level 2b; Little et al., 2018, Level 2b). Occupational therapy interventions addressed the following outcomes: overall occupational performance, education and academic performance, social participation, movement function, and sensory integration.
All 4 studies demonstrated statistically significant improvements in telehealth intervention groups for at least one outcome of interest. Three studies demonstrated significant improvements in educational performance through the use of live teleconference sessions to address handwriting (Criss, 2013, Level 3b) and academic outcomes and participation in class (Langbecker et al., 2019, Level 2b; Little et al., 2018, Level 2b). Other statistically significant outcomes included occupational performance and movement function as a result of a monitored program for upper extremity function (Ferre et al., 2017, Level 2b) and occupational performance and social participation as a result of live occupation-based coaching interventions (Little et al., 2018, Level 2b). Overall, the use of telehealth as a delivery mechanism to improve educational outcomes for children with developmental disorders is supported by moderate strength of evidence. Low strength of evidence is noted for other outcomes because of the limited and inconsistent findings.
Other Conditions
Occupational therapy practitioners provided telehealth interventions for people with other conditions, including chronic obstructive pulmonary disorder, breast cancer, and status post–intensive care, and for community wheelchair users. All 4 identified articles were Level 2b. One study had low risk of bias, and 3 had moderate risk of bias (see Table A.2). Telehealth approaches varied among the studies: tailored online programs (Giesbrecht & Miller, 2019, Level 2b), telephone and text message delivery (Hegel et al., 2011, Level 2b; Jackson et al., 2012, Level 2b), and live videoconferencing (Jackson et al., 2012, Level 2b; Knox et al., 2019, Level 2b).
All studies demonstrated at least one statistically significant outcome of interest. Statistically significant outcomes included quality of life and functional mobility as a result of wheelchair training (Giesbrecht & Miller, 2019, Level 2b); psychosocial function and quality of life after problem-solving interventions (Hegel et al., 2011, Level 2b); ADL performance, functional mobility, and cognition as a result of functional training via live teleconference (Jackson et al., 2012, Level 2b); and mobility, psychosocial, and respiratory functions after educational and exercise interventions (Knox et al., 2019, Level 2b). Because of the variability in outcome measures and moderate quality of the studies, there is low strength of evidence to support use of telehealth interventions for these conditions.
Discussion
The purpose of this systematic review was to synthesize the existing evidence on telehealth service delivery, examine the effectiveness of interventions, and inform practitioners and reimbursement entities. This review was unique in considering the breadth of interventions and outcomes within occupational therapy’s scope of practice, including health promotion, disease prevention, and other wellness strategies. Overall, positive outcomes were found within groups for most occupational therapy interventions provided via telehealth.
This systematic review of studies with people with neurological conditions resulted in strong strength of evidence to support the use of telehealth approaches for occupational therapy intervention. Neurological conditions affect one-third of Americans, and many of those affected struggle to access treatment because of lack of availability, access, and affordability (Cardinale, 2018). This systematic review supports Cardinale’s (2018) conclusion that telehealth can be a solution to these struggles to enhance care models and provide efficient and clinically effective occupational therapy services for people with neurological conditions. The American Academy of Neurology published a Telehealth Position Statement (Hatcher-Martin et al., 2021) that supports the use of telehealth services to improve patient access and identifies a need to advocate for policies that ease unnecessary restrictions on telehealth service delivery. Given the strong strength of evidence noted in this systematic review, this advocacy should include access to and reimbursement for occupational therapy services.
However, careful consideration should be given to intervention focus for recipients of telehealth service delivery. Although studies by Finlayson et al. (2011) and Giesbrecht and Miller (2019) resulted in improvement in areas such as fatigue or self-efficacy in wheelchair skills, they reported inconsistent findings regarding quality-of-life outcomes. These findings pose the question of whether interventions addressing outcomes related to quality of life might not be as suited for telehealth as traditional therapeutic interventions. However, studies not including occupational therapy as an intervening discipline have shown positive results. Valdivieso et al. (2018) found that quality-of-life measurements were higher for high-risk elderly people with chronic conditions in a telehealth group compared with those who received usual care. Another study that examined quality of life with elderly people found a significant difference, with telecare contributing to improvements in anxiety and depression compared with usual care (Hirani et al., 2014). In addition, several studies included in this systematic review showed positive outcomes for other areas of psychosocial and physical function. These promising results warrant a need for further research regarding occupational therapy intervention for quality-of-life outcomes.
Participants using the Hand Mentor Pro robot-assisted device to treat unilateral ischemic or hemorrhagic stroke showed statistically significant improvement in motor skill development but not in depression (Linder et al., 2015). This is not surprising, because Linder et al. (2015) recognized that these findings were consistent with those of other studies that showed improvements in motor skills with repetitive tasks. Linder et al. (2015) further emphasized that the lack of difference in depression might also be attributed to the individual goal setting and limitations in the robotic device’s adaptability. Practitioners need to be aware of how individual clients, modalities, and telehealth as a service delivery model may interact during treatment planning. Although occupational therapy interventions for recipients of telehealth are promising, they do not always prove effective in all outcome measures, which may affect which methods to use.
In this systematic review, strong strength of evidence was found to support the use of telehealth to deliver occupational therapy interventions to people with pain conditions. This supports the review by Perez et al. (2021) that identified telehealth as a viable option for providing pain management services. Although most evidence exists to support the use of nurse-led telehealth for pain management, this systematic review adds to that existing evidence to support the use of occupational therapy. In addition, moderate strength of evidence supported telehealth delivery for children with developmental disorders for outcomes of educational performance. Although the use of telehealth became more common as a result of COVID-19, barriers still exist to implementation of school-based occupational therapy services, including lack of practitioner training, lack of access to technology for students, and concerns about the quality of the intervention compared with in-person service delivery (Hermes et al., 2021). The results of this systematic review point to a need for ongoing research but should provide occupational therapists with confidence in the effectiveness of occupational therapy intervention via telehealth for certain conditions.
One important aspect of telehealth as a service delivery model is patient satisfaction. Cottrell et al. (2019) reported a significant increase in treatment satisfaction among patients participating in telehealth treatment compared with an on-site treatment option. The high level of satisfaction was related to treatment cost, access, and overall experience with treatment conducted via telehealth. This finding was consistent with Harkey et al.’s (2020) systematic review, which found increased rates of patient satisfaction with occupational therapy via telehealth delivery to rural communities.
Telehealth services provide practitioners with a greater scope of accessibility to assist clients. It is a service delivery model within the already existing scope of practice used for “evaluation, intervention, consultation, monitoring, and supervision” (Cason, 2015, p. 2). With the extraordinarily high cost of health care, the addition of funding travel expenses for providers to deliver services to remote patients is an important concern. Telehealth services reduce this cost while also resulting in fewer missed appointments and effecting positive health outcomes compared with traditional onsite services.
Barriers to implementation of telehealth services in practice need to be considered. Practitioners must be equipped to meet the demands of this new delivery model with the appropriate knowledge, skills, tools, and administrative support. Training in how to bridge the gap between technology and patient care as well as the application of telehealth in intervention planning and implementation should be considered. Practitioners must learn to establish therapeutic rapport and client-centered practice despite limited face-to-face interactions. Occupational therapy education also needs to respond to this change and provide more experiential learning opportunities regarding telehealth in academic settings.
Although this systematic review found strong strength of evidence to support the use of telehealth occupational therapy interventions for people with neurological and pain conditions and moderate strength of evidence for educational outcomes for people with developmental disorders, there is low strength of evidence to support other outcomes for people with developmental disorders and other conditions. This is primarily a result of a lack of evidence and consistent outcome measures from which to draw conclusions. Overall, results point to a need for practitioners to advocate for their unique contributions to the improvement of telehealth care, at both implementation and policy levels, especially for areas in which occupational therapy interventions provided using this medium are supported by strong strength of evidence. In addition, ongoing research is needed for a variety of conditions and across the scope of occupational therapy practice to continue to inform practice.
Limitations
The findings of this systematic review are limited by a variety of interventions examined in the included studies, which limits the available evidence for each type of intervention. Although outcomes were focused on those within the scope of occupational therapy practice, they were also varied. Additional research is needed that focuses solely on interventions geared toward outcomes related to quality of life to determine the efficacy of telehealth in this area. Participation in pilot programs that implement telehealth services and engagement in research regarding appropriate frequency, duration, and intensity of telehealth interventions are needed. Finally, this research focused on available evidence from 2009 to 2019. We anticipate that the available evidence has increased since COVID-19, which spurred an increase in the use of telehealth services. Completing a systematic review with updates to include studies published after 2019 is warranted.
Implications for Occupational Therapy Practice
Telehealth services provide practitioners with a greater scope of accessibility to assist recipients of occupational therapy. Telehealth is a service delivery model within the already-existing occupational therapy scope of practice (Cason, 2015). With the increased momentum toward the use of telehealth in the health care arena as a result of policy and societal changes, many implications for clinical practice can be gleaned. This systematic review has the following implications for occupational therapy practice: ▪ Telehealth can be used across the lifespan in occupational therapy practice to treat a variety of occupational performance issues, especially for people with neurological and pain conditions. ▪ Careful consideration should be given to appropriateness of clients for telehealth service delivery. ▪ Practitioners and professional organizations should advocate at the individual and community levels for appropriate use of telehealth and at the policy level for health system changes that advance telehealth-based interventions and support reimbursement.
Conclusion
Before the COVID-19 pandemic, there was a growing need and interest in telehealth services by both clients and practitioners; however, the pandemic accelerated the need to examine the effectiveness of occupational therapy interventions delivered via various platforms, such as synchronous or asynchronous telehealth services. Although this systematic review was initiated before the COVID-19 pandemic and does not include studies resulting from the pandemic, it contains an updated synthesis of evidence to support the use of telehealth as a delivery format for occupational therapy interventions across the lifespan and includes both rehabilitation and habilitation outcomes across the scope of occupational therapy practice. Strong strength of evidence was found to support occupational therapy interventions provided via telehealth for neurological and pain conditions, and moderate strength of evidence was found for educational outcomes for people with developmental delays. Further research for other conditions and other outcomes for people with developmental delays is warranted.
Supplemental Material
Supplementary material for Telehealth Interventions Within the Scope of Occupational Therapy Practice: A Systematic Review
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.049417.pdf for Telehealth Interventions Within the Scope of Occupational Therapy Practice: A Systematic Review by Diana R. Feldhacker, Vanessa D. Jewell, Sadie Jung LeSage, Haley Collins, Helene Lohman and Marion Russell in The American Journal of Occupational Therapy
Footnotes
*
Indicates studies included in the systematic review.
Acknowledgments
All authors participated in the conceptual design of the study, engaged in data collection, and were involved in drafting and editing this systematic review. None of the authors declare competing financial interests. This research was not funded by any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. However, it was supported by a student research fellow, Sadie Jung, who was paid by Creighton University.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.