
Abstract
The findings of this study confirm that the Chinese version of the Health Promoting Activities Scale (HPAS) is cross-culturally equivalent to the original HPAS, is psychometrically sound, and could be used as an outcome measure of Chinese mothers’ participation in health-promoting activities.
Chinese mothers of children with disabilities report poor sleep quality, reduced physical health (Lee et al., 2018), elevated parenting stress (Wang et al., 2013), and low health-related quality of life (Lee et al., 2019). These factors could affect mothers’ caregiver role, self-care occupations and routines, occupational balance, and overall well-being. Studies of non-Chinese parents of children with disabilities found they had less free time and compromised leisure participation compared with parents of typically developing children (Luijkx et al., 2017), and mothers of children with disabilities in Australia reported lower participation in health-promoting activities than other mothers (Bourke-Taylor et al., 2014). Occupational therapists are concerned with people’s patterns of participation and the development of appropriate interventions to improve their engagement in meaningful occupations (Bourke-Taylor et al., 2012). In the family-centered care framework, occupational therapists have the opportunity to provide intervention for mothers of children with disabilities (DeGrace, 2003).
It has been established that a well-resourced mother is more able to provide quality care to her child. Parent-based interventions emerging in East Asia include an intervention that helps Chinese mothers use positive thinking, reduce negative emotions, and strengthen their parenting skills (Zu et al., 2019); a mindfulness-based intervention developed for Hong Kong parents aims to reduce their stress and anxiety symptoms and increase acceptance of their children’s limitations (Lo et al., 2017), and a Japanese mother-centered program focuses on improving mothers’ physical and psychological well-being through activities and peer support (Niinomi et al., 2016). Yet none of these programs address the reduced occupational participation and routines of mothers of children with disabilities.
Healthy Mothers, Healthy Families© (HMHF) is an Australian program that aims to empower the mothers of children with disabilities to participate in health-promoting activities (Bourke-Taylor et al., 2019). Health-promoting activities are self-selected activities that are both meaningful and contribute to one’s health and well-being (Bourke-Taylor et al., 2012). Research has demonstrated that the HMHF intervention is effective (Bourke-Taylor et al., 2019; Bourke-Taylor, Joyce, Grzegorczyn, et al., 2021; Bourke-Taylor, Joyce, Morgan, et al., 2021). The Health Promoting Activities Scale (HPAS) was developed to measure the frequency of participation in health-promoting activities among Australian mothers of children with disabilities; it is the primary tool used to promote and measure healthy lifestyle behaviors and activity choices to improve maternal health. The HPAS was used as an outcome measure for the HMHF program. Petty and Trussell (2021) proposed the concept of leisure self-care, referring to activities that serve both self-care and leisure purposes, and postulated that these activities contribute to health and well-being. The HPAS items include leisure self-care activities, that is, self-care, physical, recreational, spiritual, and social types of activities. With cross-cultural validation, the HPAS could be used more widely. In this article, we report on the translation to Chinese and construct validity of the Chinese version of the HPAS in relation to measures of well-being, mental health, and activity satisfaction.
Well-Being and Participation
Well-being can be viewed from a hedonic or eudaimonic perspective. The hedonic perspective refers to the subjective experience of happiness and life satisfaction; the eudaimonic perspective refers to optimal psychological functioning, good relationships with others, capacity for self-development, autonomy, self-acceptance, self-esteem, competence, and purpose in life (Taggart et al., 2015). Hayward and Taylor (2011) proposed that eudaimonic well-being is the subjective experience of doing and may be likened to “being” or occupational satisfaction. They argued that experiences of eudaimonic well-being are unique, individual, and values dependent. This perspective implies that participation in self-selected, enjoyable, and purposeful activities could potentially contribute to both hedonic and eudaimonic well-being. It has been supported by meta-analysis, which found links between leisure engagement and hedonic well-being across a wide range of populations (Kuykendall et al., 2015). The recent coronavirus disease 2019 (COVID-19) pandemic has also raised awareness that leisure participation could meet the physical, social–cognitive, and emotional needs of isolated people during times of uncertainty (Liu et al., 2022), and evidence has shown that participation in leisure self-care is health promoting and has a positive impact on well-being and life satisfaction, which is congruent with the occupational therapy perspective (Hayward & Taylor, 2011).
Cross-Cultural Equivalence of Participation Instruments
A systematic review highlighted the importance of cross-cultural equivalence testing of participation instruments because participation can have varied meanings in different cultures (Stevelink & van Brakel, 2013). A meta-synthesis on the experiences of Asian parents of children with autism identified their challenges in a collectivist–conformist environment with disability-related stigma and familial obligations (Shorey et al., 2020). Shorey et al. (2020) also reported that to maintain their health and psychological well-being, Asian parents relied more on other community members than did non-Asian parents. Other studies have also described the influence of culture on Asian mothers’ valued occupations and parental role obligations. Hwang et al. (2020) found that Asian parents perceived their main role as helping their children with disabilities thrive, and Sim et al. (2021) reported that East Asian mothers viewed their valued activities as working toward their child’s success. These studies highlight cultural differences and reinforce the necessity for cross-cultural validation of participation instruments from another culture.
The HPAS was developed in Australia; hence, the aim of this study was to determine the construct validity of the Chinese translation of the HPAS to ensure a valid, reliable, and culturally equivalent measure of health-promoting activities for use with Chinese-speaking mothers of children with disabilities. The COnsensus-based Standards for the selection of health status Measurement INstruments (COSMIN) taxonomy of measurement properties includes cultural validity as a measurement property for construct validity (Mokkink et al., 2010), further justifying our study.
Our research questions were as follows: Is the Chinese translation of the HPAS culturally equivalent to the English HPAS? How frequently does our sample of Chinese-speaking mothers of children with disabilities participate in health-promoting leisure activities? How internally reliable is the Chinese version of the HPAS with Chinese-speaking mothers? How valid is the Chinese version of HPAS when used with Chinese-speaking mothers of children with disabilities?
Hypotheses to explore construct validity were the following: There will be moderate to strong correlations between the Chinese version of HPAS and well- being and mental health in our sample. The Chinese version of HPAS will have a moderate to strong correlation with mothers’ reports of satisfaction with their participation in health- promoting activities.
Method
Stevelink and van Brakel’s (2013) checklist for designing cross-cultural validations guided our study design. This project was approved by the Monash University Human Research Ethics committee (Approval No. 19647).
Translation of the Health Promoting Activities Scale
Cultural equivalence refers to the extent to which an instrument is equally suitable for use in two or more cultures (Stevelink & van Brakel, 2013). We used forward and backward translation and included layperson translators and an expert committee. Altogether, the translation process involved the original author of the HPAS (Helen Bourke-Taylor), four bilingual occupational therapists with postgraduate degrees (including So Sin Sim and Mong-lin Yu), and four laypeople, including two mothers of children with disabilities (Figure 1). The expert committee included reviewers who were individually proficient in different forms of Chinese to address potential variation in Chinese expressions, and their ratings and their feedback resulted in the finalized translation.
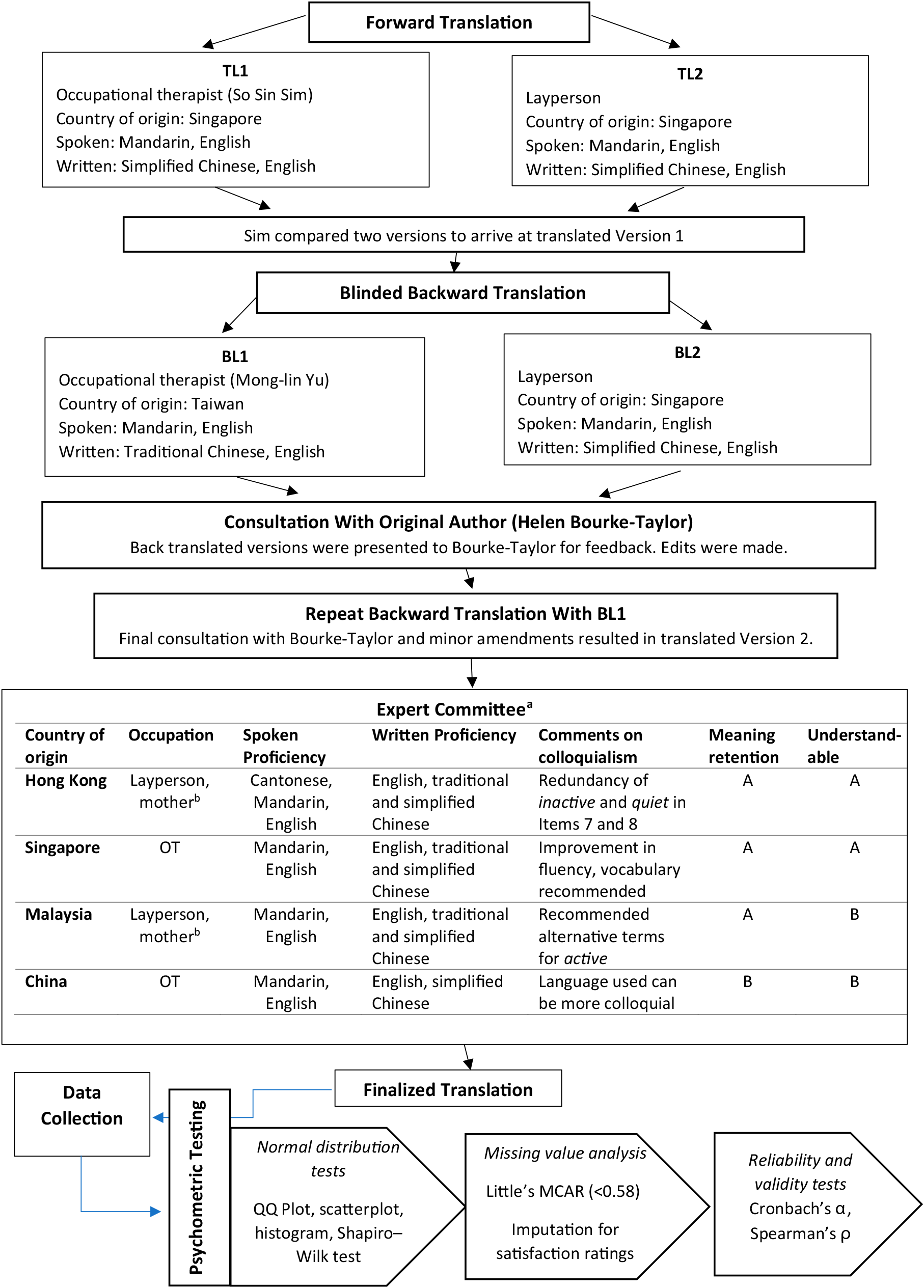
Overview of validation process.
Participants
Participants were ethnic Chinese mothers (N = 89) who had at least one child with disabilities, residing in Australia, Singapore, or Taiwan. Participants self- selected to complete the survey in Chinese. Recruitment flyers were advertised on social media platforms (Facebook, WeChat groups, WhatsApp groups), caregiver support groups, two disability agencies, a community newspaper, and community spaces, such as libraries, grocery stores, and church noticeboards, from January 2021 to August 2021. Participants were invited to complete a Qualtrics e-survey (Qualtrics, Provo, UT) via the web link or QR code on the flyer, which led them to the explanatory statement and the consent form. Purposive snowball sampling occurred by explicitly encouraging participants to forward flyers to other Chinese mothers of children with disabilities.
Measures
Demographic Data
Demographic questions were developed to collect basic information on both the mother’s and the child’s characteristics.
Health Promoting Activities Scale
The HPAS is an ordinal scale consisting of eight items that represent categories of activities that a person may participate in for enjoyment, health, or physical, social, or spiritual engagement (Bourke-Taylor et al., 2012). An accompanying key provides examples of activities for each category. Respondents are asked how frequently they participate in each category of activities on a scale ranging from 1 (never) to 7 (one or more times per day). The total score ranges from 8 to 56, with higher scores indicating higher frequency of participation in these health-promoting activities. The HPAS has moderate internal consistency (Cronbach’s α = .78). Its construct validity was supported by moderate correlations with subjective maternal mental and general health and differentiation of leisure participation among mothers reporting varying mental health statuses (Bourke-Taylor et al., 2012). Subsequent validation with Australian mothers with typically developing children showed moderate reliability and stability (Cronbach’s αs = .73–.78; intraclass correlation coefficient = .90, minimum detectable change = 5), supporting its suitability as an outcome measure for occupational therapy interventions (Bourke-Taylor et al., 2014; Muskett et al., 2017).
Satisfaction Rating
Satisfaction ratings ranging from 1 (very dissatisfied) to 4 (very satisfied) were used with each of the eight HPAS items. These ratings were used to measure mothers’ self-reported satisfaction with their participation in each category of activities. Overall internal consistency was high (Cronbach’s α = .86).
Warwick–Edinburgh Mental Well-being Scale
The Warwick–Edinburgh Mental Well-being Scale (WEMWS) is a well-validated instrument that measures both hedonic and eudaimonic well-being; it has previously been translated into several languages and is used cross-culturally (Taggart et al., 2015). Permission was sought to use the English and Chinese scales. The WEMWS has 14 items covering subjective well-being and psychological functioning. Each item is rated on a Likert scale ranging from 1 (none of the time) to 5 (all of the time) and is scored by summing the responses to statements on thoughts and feelings.
On the basis of a validation study, the Chinese WEMWS has been reported to be conceptually equivalent to the original version, with high internal reliability (Cronbach’s α = .94) and a test–retest reliability of r = .83; hence, it a reliable tool to evaluate mental well-being in nonclinical settings (Dong et al., 2016). For our study, Cronbach’s α = .91.
Personal Well-being Index
The Personal Well-being Index (PWI) is a self-rated seven-item questionnaire that measures subjective well-being across seven quality-of-life domains: standard of living, health, achieving in life, relationships, safety, community connectedness, and future security (Cummins et al., 2003). Respondents rate their level of satisfaction for each item on a scale ranging from 1 (no satisfaction at all) to 10 (completely satisfied), with the mean score representing overall personal well-being.
The Chinese PWI demonstrated good utility, validity, reliability, sensitivity, and discriminatory performance across studies with Chinese populations (Lau, 2014), with Cronbach’s αs ranging from .72 to .85, indicating moderate to high internal consistency. Cronbach’s α in our sample was .90.
Kessler Psychological Distress Scale–10
The Kessler Psychological Distress Scale–10 (K10) is a self-report measure of psychological distress. Items are rated on a 5-point scale ranging from 1 (none of the time) to 5 (all of the time), with high scores associated with diagnoses of anxiety and affective disorders (Andrews & Slade, 2001). The K10 total score is obtained by summing item ratings.
The Chinese K10 was found to be reliable (Cronbach’s α = .93) and valid in screening for psychological distress among Chinese parents of children with cancer (Bu et al., 2017). Cronbach’s α was found to be high for our sample (.94).
Data Handling and Analysis
All data were exported from Qualtrics to Excel and extracted into IBM SPSS Statistics for Windows (Version 27). Data screening and checking were first completed with checks for outliers, and normality tests on all total scores showed that our data were not normally distributed; hence, we used nonparametric tests (Spearman’s ρ) to conduct the correlational analysis.
Missing value analysis was conducted for all total scores and Little’s missing completely at random test was not significant (p = .580), indicating that values were missing completely at random (Tabachnick, 2019). Data imputation using series mean was done for satisfaction rating scores because this measure was the only one with more than 10% missing values (28.1%).
Descriptive statistics were generated for the demographic variables and the Chinese HPAS items (Tables 1 and 2). Cronbach’s α was calculated to assess internal consistency. Bivariate correlations were calculated using Spearman’s ρ and are shown in Table 3.
Participant and Child Demographic Characteristics
Child may have more than one diagnosis.
Child may have more than one difficulty.
Responses to HPAS Items
Note. N = 89. Percentages may not total 100 because of rounding. For copies of the Chinese translation of the HPAS, contact
Correlations Between the Chinese HPAS and Other Scales
Note. N = 89. HPAS = Health Promoting Activities Scale; K10 = Kessler Psychological Distress Scale–10; PWI = Personal Well-being Index; WEMWS = Warwick–Edinburgh Mental Well-being Scale.
Imputed because of >10% missing data.
p < .01.
p < .001.
Results
Table 1 summarizes the participants’ demographic data (N = 89). Most participants were ages 41 to 50 yr (46%), married (85%), and living in Taiwan (72%) and had postsecondary or higher education qualifications (90%). Nearly half of the participants (43%) were employed, 63% of whom were engaged in full-time paid work. The mean age of the children with disabilities was 12.6 yr (SD = 8.2), and autism spectrum disorder was the most common diagnosis (55%).
Table 2 presents mothers’ responses to each of the Chinese HPAS items. The mean total Chinese HPAS score was 28.6 (SD = 8.8), and Cronbach’s α was .74, indicating moderate internal reliability. Cronbach’s α did not significantly increase when items were removed individually, indicating that no item needed to be removed. Corrected item–total correlations for seven items were good (range = .32–.64), except for Item 4 (Supplemental Table A.1, available online with this article at https://research.aota.org/ajot).
Spearman’s ρ indicated a positive correlation between Chinese HPAS Total score and satisfaction rating total (r = .45, p < .001; n = 87), WEMWS Total score (r = .61, p < .001; n = 86), and PWI mean score (r = .44, p < .001; n = 84) and a negative correlation with K10 total score (r = −.33, p = .002; n = 81; see Table 3).
Discussion
We found moderate to strong correlations between scores on the Chinese translation of the HPAS and measures of well-being and mental health symptoms, supporting the construct validity of the Chinese version of the HPAS. The HPAS had moderate internal reliability (Cronbach’s α = .74). Hence, our findings indicate that the Chinese HPAS was translated appropriately and is culturally valid. Several findings suggest that a discussion of the HPAS’s cultural equivalence, the demographic comparison of our sample with the original sample, Chinese mothers’ HPAS results, and the HPAS’s potential clinical utility is warranted.
Cultural Equivalence
Cultural equivalence of a translated instrument is supported when conceptual, semantic, item, operational, and measurement equivalence are equally relevant and acceptable across both cultures (Stevelink & van Brakel, 2013). For the HPAS, the examples provided along with each category of activities clarified the meanings represented by each item, which contributed to conceptual equivalence (measured concepts are the same in both cultures) and item equivalence (scale items are equally relevant and acceptable in both cultures; Stevelink & van Brakel, 2013).
Conceptual and semantic equivalence (retention of meaning across languages) was also achieved by the use of both laypeople and occupational therapists, forward and blinded backward translation, multiple consultations with the original HPAS author, and inclusion of expert reviewers who were proficient in different forms of the Chinese language (Stevelink & van Brakel, 2013). The overall ratings for meaning retention and comprehensibility indicated that the final translation was acceptable, although suggestions were made to improve colloquialism (see Figure 1).
The Chinese HPAS was formatted, administered, and measured in the same way as the original HPAS, thus attaining operational equivalence (the same administration procedures and measurement methods were used with different translations; Stevelink & van Brakel, 2013). Measurement equivalence (validity and reliability) has been addressed by moderate to strong correlations of the HPAS with scores on measures of well-being and mental health.
Comparisons Between Samples
Our sample was similar to the Australian sample used in the validation study of the original HPAS, in which the mothers’ mean age was 41.7 yr, 84% were married or partnered, and 54% were employed. The sample in this study had a much higher proportion of mothers working full time (63% vs. 17%) and with higher education (90% vs. 56% had postsecondary qualifications). A plausible explanation for the difference could be the higher value placed on undergraduate education in East Asia, better access to other caregivers in the extended family, and the availability of paid domestic helpers (Sim et al., 2021), thus allowing mothers to work outside the home. Our sample had slightly older children than the Australian sample (12.6 yr vs. 9.5 yr), which could perhaps have contributed to mothers’ higher employment rates. In addition, the most commonly reported diagnosis was autism spectrum disorder.
Frequency of Participation
The mean HPAS Total score of our Chinese sample was higher (M = 28.6, SD = 8.8; n = 87) than that of Australian mothers (M = 21.7, SD = 8.5; n = 152), indicating higher overall participation in health-promoting activities among Chinese mothers. Mothers most frequently (at least weekly) participated in solo activities involving quiet inactive leisure (46%), physical active recreation (45%), and time out for self (44%). The results are also consistent, with nearly 43% of Chinese mothers reporting never or rarely participating in “social activities with people who are important and supportive towards you.” One possible explanation could be a cultural preference for solitude over socialization; another could be that the mothers had smaller social networks to avoid stigma (Sim et al., 2021). The cause and effect of mothers’ low social participation warrants further research. Another observation was the higher frequency of time out for self, for which the accompanying examples included facials and shopping, which are self-pampering activities highly valued by East Asian women (Yang, 2011). These findings are examples of cultural differences in participation in health-promoting activities that can be further investigated.
About half of our participants met the guidelines for weekly physical activity (World Health Organization, 2020), with an overall higher frequency of participation in physical activities compared with the Australian sample (alone, 45% vs. 16%; with others, 19% vs. 22%), implying that mothers in our sample were participating more often in physical activities. Those who did not engage enough in physical activities might eventually develop negative health consequences. Another noteworthy observation was that the frequency of physical activities done alone was about twice that of physical activities done with others, further reinforcing that mothers engaged more in solo activities than in activities with others. There was also a contrast between samples; our participants reported personal health care tasks as one of the most infrequent activities (48%), whereas Australian participants reported these tasks as their most frequent activity (46%). Personal health care tasks is related to intentional planning and formalized commitments to healthy living, which seemed less common among the Chinese mothers. A plausible explanation could be attributed to cultural beliefs, for example, advice based on nutrition science might conflict with Chinese health beliefs based on principles of heat–cool balance or personal health care tasks might be viewed as self-centered or individualistic, hence less intuitive in a collectivist culture. Despite these explanations, our findings highlight the importance of identifying potential barriers for Chinese mothers to be proactive in planning their health tasks and engaging in physical activities.
Clinical Utility
Our findings demonstrated that the Chinese version of the HPAS is a valid tool for use with Chinese-speaking mothers of children with disabilities. The translated HPAS will be useful when working with Chinese-speaking mothers to educate and empower them to self-select and engage in health-promoting activities. Specifically, occupational therapists could use the HPAS to evaluate mothers’ participation in health-promoting activities, as an initial assessment for healthy lifestyle redesign, as a reflective tool for mothers to achieve their health-promoting activity engagement goals, and as an outcome measure.
Limitations and Future Research
The sample sizes from each of the three countries (Australia, Singapore, and Taiwan) were small; future studies could replicate this study design for each country, which could resolve the minor colloquialism issues identified. Further psychometric tests of item responsiveness and validation could be performed with other Chinese-speaking populations to widen the HPAS’s utility. It is important to note that our data collection occurred during the COVID-19 pandemic, during which varying restrictions could have affected mothers’ normal frequency of daily activities and social participation. Factors that were not captured in this study—such as socioeconomic status, living conditions, and severity of child’s symptoms—could also have affected mothers’ reports of their participation. Future studies could further explore mothers’ activity participation preferences and experiences and the relationship between their occupational satisfaction and health and well-being.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: • The Chinese translation of the HPAS is the first cross-culturally valid tool measuring self-care leisure participation of Chinese-speaking mothers of children with disabilities and could be used by occupational therapists. • Occupational therapists can use the Chinese version of the HPAS as both an intervention and outcome measure with Chinese-speaking mothers of children with disabilities. • The Chinese version of the HPAS could be used to help Chinese-speaking mothers develop strategies to increase their participation in heath-promoting activities and therefore improve their health and well-being.
Conclusion
The Chinese version of the HPAS is psychometrically sound and culturally equivalent to the original English HPAS. It is a valid and reliable tool for measuring participation in health-promoting activities of Chinese mothers of children with disabilities.
Supplemental Material
Supplementary material for Cross-Cultural Validation of the Chinese Version of the Health Promoting Activities Scale
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2022.049434.pdf for Cross-Cultural Validation of the Chinese Version of the Health Promoting Activities Scale by So Sin Sim, Helen M. Bourke-Taylor, Mong-lin Yu, Ellie Fossey and Loredana Tirlea in The American Journal of Occupational Therapy
Footnotes
Acknowledgment
So Sin Sim is a recipient of an Australian Government Research Training Program Scholarship.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.