
Abstract
This Practice Guideline summarizes the current evidence supporting occupational therapy intervention for adults with multiple sclerosis (MS) and includes case examples and decision-making algorithms to support practitioners in addressing client goals.
Multiple sclerosis (MS) is a chronic, disabling disease in which the immune system attacks the central nervous system and causes inflammation (National Multiple Sclerosis Society, 2021). More specifically, the immune system damages myelin, a substance that is critical for nerve conduction. The cause of MS is not yet fully understood; however, it is thought that genetics, infections or viruses, and environmental factors may be involved. MS is the most common neurological disease among young adults, with an incidence rate of 3 in 100,000 (Ma et al., 2014), and most people with MS have their first symptoms between ages 20 and 40 yr (National Institute of Neurological Disorders and Stroke, 2022). In the United States, 727,344 people have MS (Wallin et al., 2019). MS can be costly to individuals and society; total annual costs for care of people with MS range from $53,438 to $74,055. In addition, people with MS are commonly unemployed; the estimated percentage of people with MS who are employed after diagnosis ranges from 40.7% to 48.1% (Lo et al., 2021).
MS can cause a wide variety of symptoms, including problems with balance, vision, physical and cognitive fatigue, bowel and bladder dysfunction, sexual dysfunction, spasticity, tremor, pain, pseudobulbar affect, and depression. Of these symptoms, fatigue is one of the most prevalent; about 89% of people with MS experience fatigue (National Multiple Sclerosis Society, 2021). The prevalence and severity of these symptoms vary from person to person. In addition, the symptoms and severity of symptoms experienced by a person with MS on any given day are often unpredictable.
The National Multiple Sclerosis Society identifies four different disease types: clinically isolated syndrome (CIS), relapsing–remitting MS, secondary progressive MS, and primary progressive MS. A diagnosis of CIS is given when a person has a first episode of neurological symptoms caused by inflammation and demyelination that lasts more than 24 hr but does not meet the criteria for a diagnosis of MS. Not everyone diagnosed with CIS will eventually be diagnosed with MS. Relapsing–remitting MS is the most common form of MS, and about 85% of people with MS are initially diagnosed with it. Relapsing–remitting MS involves exacerbations in which the person with MS experiences worsening of symptoms followed by a full or partial recovery. Secondary progressive MS occurs when a person initially has a relapsing–remitting course of disease but transitions to a worsening and progressive course. Finally, primary progressive MS involves worsening of symptoms and function from the start of the disease with no relapses or remissions.
MS has no cure; however, a variety of options are available to manage the disease. Medical management aims to control acute attacks, manage progression, and remediate symptoms (Hauser & Cree, 2020). Medical treatments have advanced significantly in recent years, which has improved many patients’ long-term outcomes. More specifically, disease-modifying therapies can alter the course of MS for some patients; may result in less frequent relapses; and may stabilize, delay, or sometimes even improve levels of disability. In addition to medical management, therapies such as occupational therapy and physical therapy can play an important role in the management of MS. The overall focus of occupational therapy for people with MS is to support participation in meaningful activities. For example, occupational therapy practitioners may focus on areas such as prevention and health education, instruction in compensatory or remediation activities, maintenance of function, accessibility issues, and cognitive strategies (Ghahari & Finlayson, 2018). In addition, occupational therapy practitioners can play an important role in supporting the caregivers of people with MS.
These Practice Guidelines update the MS portion of the Occupational Therapy Practice Guidelines for Adults With Neurodegenerative Diseases (Preissner, 2014). The previous guidelines, which were based on a systematic review of occupational therapy–related interventions for adults with MS, discussed two broad areas of interventions for people with MS: (1) interventions focusing on activity and participation and (2) interventions focused on client factors and performance skills.
At the time of the 2014 practice guidelines, the research focused on a combination of physical and impairment-level interventions and outcomes and occupation-based outcomes. The literature has since evolved, and the current set of systematic reviews (Cunningham & Uyeshiro Simon, 2022; Foidel et al., 2021; Nastasi & Harris, 2021; Preissner & Plow, 2021; Yu et al., 2021) that inform this Practice Guideline update and expand on the prior evidence. Thus, this Practice Guideline incorporates enhanced and additional evidence to support occupational therapy practice for adults with MS.
Systematic Review Questions
This Practice Guideline is based on the following four questions: What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve and/or maintain sleep and rest and performance and participation in activities of daily living (ADLs) for adults with MS? What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve and maintain performance and participation in instrumental activities of daily living (IADLs) among adults with MS? What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve and/or maintain the performance of and participation in education, work, volunteering, leisure, and social participation among adults with MS? What is the evidence for the effectiveness of interventions for caregivers of people with MS within the scope of occupational therapy practice that facilitate and maintain participation in the caregiver role?
Goals of This Practice Guideline
Through this Practice Guideline, the American Occupational Therapy Association (AOTA) aims to help occupational therapy practitioners, as well as the people who manage, reimburse, or set policy regarding occupational therapy services, understand occupational therapy’s role in providing services to adults with MS. This guideline can also serve as a reference for health care professionals, health care facility managers, education professionals, education and health care regulators, third-party payers, managed care organizations, and those who conduct research to advance care of adults with MS.
This guideline was commissioned, edited, and endorsed by AOTA without external funding being sought or obtained. It was financially supported entirely by AOTA and was developed without any involvement of industry. AOTA supports systematic reviews on adults with MS as part of its Evidence-Based Practice (EBP) Project. AOTA’s EBP Project is based on the principle that the EBP of occupational therapy relies on the integration of information from three sources: (1) clinical experience and reasoning, (2) preferences of clients and their families, and (3) findings from the best available research.
All authors of the systematic reviews completed conflict-of-interest disclosure, with no conflicts noted. AOTA reviews practice guidelines every 5 yr, and updates them as needed, to keep recommendations on each topic current according to criteria established by ECRI (2020). Guideline topics are evaluated for their currency by a multidisciplinary advisory group consisting of AOTA members, nonmember content experts, and external stakeholders. In addition, a preliminary search of the literature is conducted to determine whether an updated systematic review is warranted.
This Practice Guideline reports the findings from systematic reviews of published scientific research addressing focused topic-specific questions; interventions that did not emerge from the published literature or did not meet the inclusion criteria were not included. The occupational therapy practitioner makes the ultimate clinical judgment regarding the appropriateness of a given intervention considering a specific client’s or group’s circumstances, needs, and response to intervention and the evidence available to support the intervention. We provide examples of how this evidence informs practice in the Clinical Case Studies and Algorithms section. In addition, the Appendix provides practitioners with tools to translate this evidence to clinical practice.
Clinical Recommendations for Occupational Therapy Interventions for People With Multiple Sclerosis
Clinical recommendations are the final phase of the synthesis of systematic review findings. The findings for each systematic review question are graded in terms of how confident a practitioner can feel that using the interventions presented in the evidence will improve the outcomes of interest to their clients. The grade is based on the specificity of the intervention, number of studies supporting the intervention, levels of evidence of the studies, quality of the studies, and significance of the studies’ findings. Interventions included in the clinical recommendations must be specific to a population, and the articles that describe them must provide sufficient detail for the reader to understand the intervention and the outcome of interest.
Describing the strength of clinical recommendations is an important part of communicating an intervention’s efficacy to practitioners and other users. Research evidence needs to be considered in conjunction with client needs and goals as well as sound clinical reasoning based on experience. The clinical recommendations for this Practice Guideline were evaluated and finalized by AOTA staff, the AOTA research methodologist, and systematic review and practice guideline authors. AOTA uses the grading methodology provided by the U.S. Preventive Services Task Force (2018) for clinical recommendations. The recommendations pertaining to each review question, along with the studies’ level of evidence and supporting details, are presented in Tables 1 through 4.
Clinical Recommendations and Supporting Evidence: Interventions to Improve or Maintain Sleep and Rest and Performance and Participation in ADLs Among Adults With MS
Note. ADLs = activities of daily living; BDI–II = Beck Depression Inventory, Second Edition; CBT = cognitive–behavioral therapy; EDSS = Expanded Disability Status Scale; Ex-PLISSIT = Extended Permission, Limited Information, Specific Suggestions, Intensive Therapy; FSFI = Female Sexual Dysfunction Index; MBSR = mindfulness-based stress reduction; MOS–S = Medical Outcomes Study Sleep Scale; MS = multiple sclerosis; MSISQ–19 = Multiple Sclerosis Sexuality and Intimacy Question–19; OT = occupational therapist; PLISSIT = Permission, Limited Information, Specific Suggestions, Intensive Therapy; PSQI = Pittsburgh Sleep Quality Index; RRMS = relapsing–remitting multiple sclerosis; SD = sexual dysfunction; SPMS = secondary progressive multiple sclerosis.
Clinical Recommendations and Supporting Evidence: Interventions to Improve or Maintain Performance of and Participation in IADLs Among Adults With MS
Note. CBT = cognitive–behavioral therapy; DMTs = disease-modifying therapies; GLTEQ = Godin Leisure-Time Exercise Questionnaire; IADLs = instrumental activities of daily living; IPAQ = International Physical Activity Questionnaire; MI = motivational interviewing; MS = multiple sclerosis; PA = physical activity; RRMS = relapsing–remitting multiple sclerosis.
Clinical Recommendations and Supporting Evidence: Interventions to Improve or Maintain the Performance of and Participation in Work, Education, Volunteering, Leisure, and Social Participation Among Adults With MS
Note. MS = multiple sclerosis.
Clinical Recommendations and Supporting Evidence: Interventions Within the Scope of Occupational Therapy Practice for Caregivers of People With MS That Facilitate Maintaining Participation in the Caregiver Role
Note. EDSS = Expanded Disability Status Scale; MS = multiple sclerosis; PRQC = Perceived Relationship Quality Components Inventory; RDAS = Revised Dyadic Adjustment Scale; SF–12 = 12-item Short Form survey.
For the purposes of this Practice Guideline, we report only findings indicating an A, B, or D grade, the grades that best support clinical decision making: ▪ A: There is strong evidence that occupational therapy practitioners should routinely provide the intervention to eligible clients. Strong evidence was found that the intervention improves important outcomes and that benefits substantially outweigh harms. ▪ B: There is moderate evidence that occupational therapy practitioners should routinely provide the intervention to eligible clients. There is high certainty that the net benefit is moderate, or there is moderate certainty that the net benefit is moderate to substantial. ▪ D: It is recommended that occupational therapy practitioners not provide the intervention to eligible clients. At least fair evidence was found that the intervention is ineffective or that harms outweigh benefits. In these reviews, we did not find Grade D evidence.
These grades are reported in Tables 1 to 4 and designated with green, indicating should do if appropriate (A), or yellow, indicating consider doing if appropriate (B). None of the studies included in these reviews reported adverse events or harms related to the interventions evaluated. We do not report the results of interventions with low strength of evidence or those that did not have enough research support to achieve an A, B, or D grade. The complete findings from the systematic reviews can be found on the AOTA website in the Critically Appraised Topics (Foidel et al., 2021; Preissner & Plow, 2021; Yu et al., 2021) and through articles published in the American Journal of Occupational Therapy (Cunningham & Uyeshiro Simon, 2022; Nastasi & Harris, 2021). As always, clinical decisions should be informed by the evidence, as presented in this Practice Guideline, in combination with clinical experience and the client’s particular goals.
Translating Clinical Recommendations Into Practice
Clinical Reasoning Considerations
The purpose of clinical practice guidelines is to help practitioners translate pertinent research findings from systematic reviews into practice. Very rarely will practitioners find an evidence-based intervention that perfectly fits their clinical setting and the client’s specific needs. Occupational therapy practitioners need to consider several questions as they evaluate the research and consider whether they can use an intervention, or adapt it in a well-reasoned way, to meet the client’s exact needs (Highfield et al., 2015): Exactly what intervention do I need to provide? ▪ What type of client outcomes am I looking for? ▪ Do the studies I’ve located provide enough detail so that I know what to do and how to do it? ▪ How well do the conditions in which I will provide the intervention match those in the studies? ▪ What are the demographic characteristics (e.g., age, gender, diagnosis, comorbidities) of the participants in the studies? ▪ In what setting (inpatient, home, community, school) did the studies take place? ▪ Do any contextual factors (e.g., resources or policies) that differ from those in the studies influence my ability to provide the intervention? How flexible is the intervention, and how much can I modify or adapt it? ▪ If my setting or client population differs from those of the studies, can I modify or adapt the intervention without changing its integrity? ▪ If I modify or adapt the intervention, what client characteristics (e.g., comorbidities) do I need to consider? ▪ Can I be proactive and plan how to modify or adapt the intervention before I start implementing it? ▪ Can I make minimal changes, such as reordering the content of the sessions, or does the need for substantial changes indicate that I should select another intervention?
To modify or adapt evidence-based interventions in practice, practitioners must plan and proactively think through the changes they need to make to fit the intervention to the client and practice setting. In addition, they must document how and why they altered the researched intervention so others in their setting know how to implement the intervention and why the changes were made. If an intervention must be adapted extensively, it may not be the right fit for the situation. When practitioners adapt an intervention, it is no longer evidence based, but rather evidence informed. If extensive adaptations to an intervention are necessary, the intervention is probably not right for the client or setting. If the practitioner finds that the intervention does not suit the client, they should not use that intervention. Clinical interventions should be as similar as possible to the interventions used in the research.
Clinical Case Studies and Algorithms
The case studies presented in this Practice Guideline illustrate how occupational therapy practitioners can translate evidence from the systematic reviews to their professional practice. We developed these cases using the evidence for the effectiveness of self-management interventions to promote performance and participation in occupations among community-dwelling adults with MS. To support the clinical decision making in the cases and ensure they fully represent current practice for adults with MS, we also describe other important resources, such as the practitioner’s expertise and the client’s values and preferences.
The case studies in this section illustrate how occupational therapy practitioners can translate evidence from the systematic reviews to professional practice when collaborating with people with MS. Each case study highlights interventions that are supported by evidence and expert opinion. The case studies include decision-making algorithms developed by the authors and AOTA staff on the basis of the clinical recommendations; each algorithm includes decision points and actions for practitioners to take. When using algorithms to inform clinical decision making, it is important for practitioners to consider each potential intervention in relation to the client’s individual goals, interests, habits, routines, and environment. When possible, we provide a CPT® billing code 1 (American Medical Association, 2021) for each intervention to aid translation to professional practice. Practitioners should choose interventions that strongly align with or are supportive of these factors in the context of the client’s occupational profile.
Case 1: Connie
Clinical Case Occupational Profile
Occupational Therapy Initial Evaluation and Findings
On the basis of Connie’s primary complaints of disrupted sexual–intimacy activities, difficulties with partner communication, and desire to return to work, the Job Procurement Self-Efficacy Scale (Wenzel, 1993), My Vocational Situation Scale (Holland et al., 1980), MS Intimacy and Sexuality Questionnaire (Sanders et al., 2000), and Perceived Relationship Quality Components Inventory (Fletcher et al., 2000) were administered. The Canadian Occupational Performance Measure (Law et al., 2019) was used to develop an occupational profile (AOTA, 2017), support collaborative goal setting and intervention planning, and monitor change in perceived activity participation and occupational performance. Connie’s scores on these measures suggested considerable disruption to performance and participation in sexual intimacy activities, self-advocacy and communication, and engagement in exploration of work options (Table 5).
Connie’s Initial Assessment Results
Note. COPM = Canadian Occupational Performance Measure; MSISQ = Multiple Sclerosis Intimacy and Sexuality Questionnaire; PRQC = Perceived Relationship Quality Components Inventory.
On the basis of Connie’s assessment results, the occupational therapist and Connie developed the following goals for treatment: Connie will improve participation in work exploration routines and will submit one job application to increase self-efficacy and support her return to part-time paid employment. Connie will increase participation in meal preparation IADLs from 1 to 2 times per day to increase independence and related activity tolerance while reducing overexertion risk. Connie will improve social participation by using an assertive communication style in one of every three interactions with her partner regarding engagement in home management IADLs to increase independence and reduce partner overcompensation. Connie will increase participation in sexual intimacy ADLs from 0 times per month to 2 times per month to increase activity tolerance while reducing overexertion risk.
Occupational Therapy Interventions
Connie attended 12 occupational therapy sessions at an outpatient occupational therapy clinic at which multiple practitioners specialize in working with people with neurological conditions. The first six sessions occurred 1 time per week, and the remaining six sessions occurred every other week.
The occupational therapist had background and training in use of the Ex-PLISSIT (Extended Permission, Limited Information, Specific Suggestions, Intensive Therapy; Daneshfar et al., 2017; Khakbazan et al., 2016) model to address engagement in sexual intimacy ADLs. The occupational therapist maintained a network of community engagement opportunities for patient referral, including a community relationship enrichment program.
Ex-PLISSIT Sexual Counseling
The occupational therapy practitioner, guided by the sexual activity algorithm in Figure 1, uses the Ex-PLISSIT model to address sexual intimacy participation with Connie (97535—Self-care/home management). The Ex-PLISSIT model was integrated into four sessions that occurred at different points in the plan of care to allow Connie to use the strategies she learned to support engagement with sexual intimacy activities. The following interventions were implemented by using the Ex-PLISSIT model: Permission: Permission takes place throughout each session. Connie explained her concerns and was provided with information about female anatomy, sexual response, and sexual dysfunction among women with MS. Limited Information: Connie identified reasons for sexual dysfunction resulting from MS and the effect of the disease on her sexual intimacy participation (sexual desire, MS symptom exacerbation, lubrication, etc.). Specific Suggestions: Connie and the occupational therapist identified specific priorities and needs to address related to sexual function. Specific suggestions for managing sexual function challenges were provided, including water-based lubrication, fluid management strategies, sexual positioning, and timing of sexual behavior.
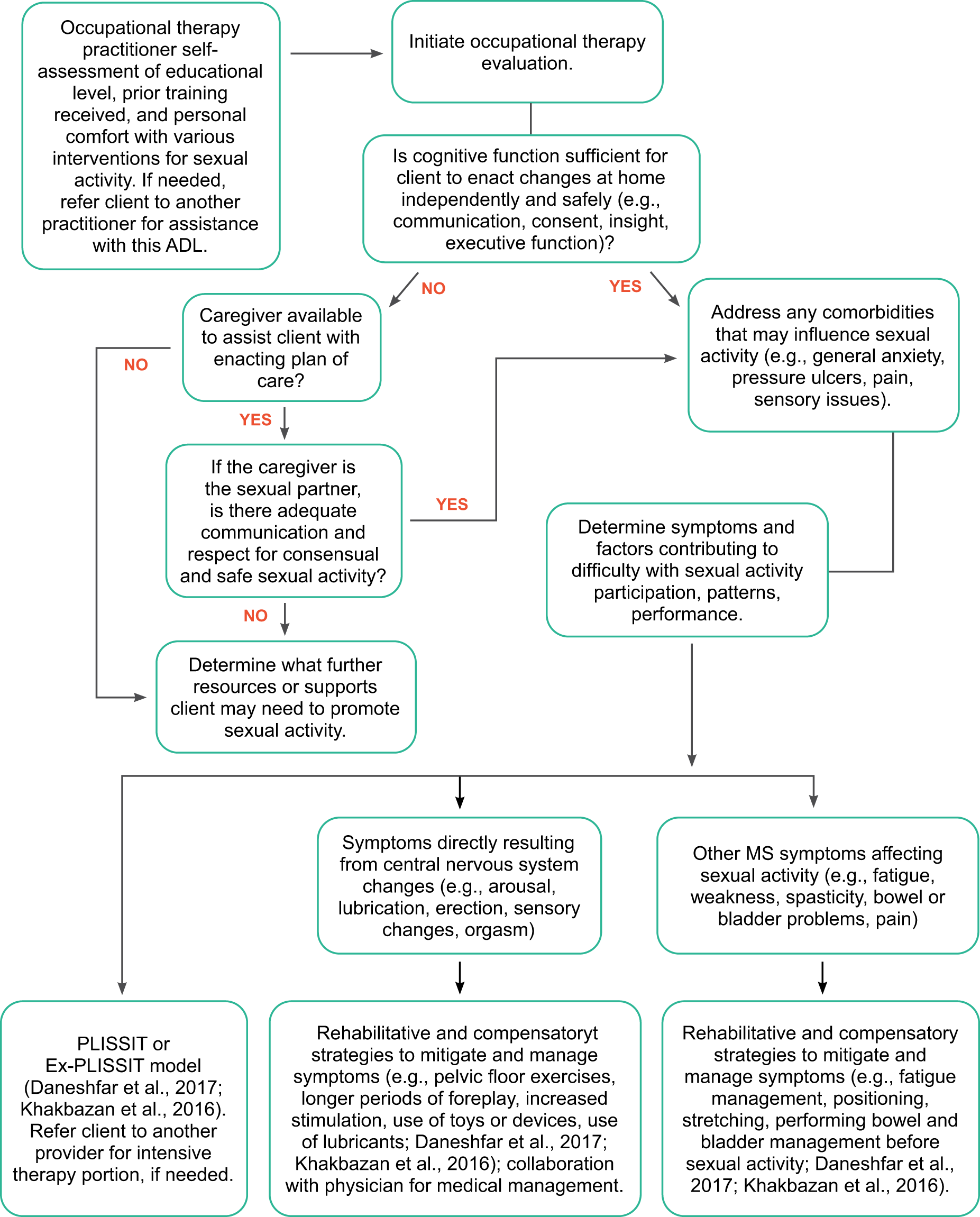
Interventions for sexual activity for adults with MS.
The occupational therapist did not engage in the Intensive Therapy (IT) component of the Ex-PLISSIT model with Connie because of a lack of IT training and expertise. However, the occupational therapist provided Connie with a referral to a local therapist who has expertise in working with people with MS to further address barriers to participation in sexual intimacy ADLs as needed.
Group Interventions for Relationship Quality
The occupational therapist referred Connie to a local community relationship enrichment program run by an occupational therapist to support her goals for communication and sexual intimacy participation with her partner (Navidian et al., 2017). Connie was encouraged to complete the enrollment process independently to reduce overcompensation by her partner. Connie enrolled in the program with her partner and reported weekly participation beginning in Week 4 of her occupational therapy treatment. The occupational therapist worked with Connie to integrate communication strategies learned during the enrichment program into interactions with her partner in the home context to support her self-advocacy efforts to increase participation in home management and meal preparation IADLs.
Work and Multiple Sclerosis Program
The occupational therapist used the Work and MS program modules (Dorstyn et al., 2017, 2018) to support Connie’s long-term goal of returning to part-time work. Six modules were delivered and used over the course of six appointments (97537—Community/work reintegration). The modules addressed the job-seeking process (three modules), job interviewing skills (two modules), and career development (one module). Each module included module objectives, interactive components to illustrate key points (e.g., case examples, worksheets), educational materials (e.g., MS and employment, benefits of work, interview preparation, disclosure of MS), and a summary of content.
The occupational therapist guided Connie in occupational self-analysis, problem solving, action planning, and short-term goal setting related to each module to support revision of her résumé, rehearsal of interview skills, job searches, and submission of job application materials.
Outcomes
Connie improved on all outcome measures and met all her occupational therapy treatment goals. She applied for a part-time job at a local elementary school, and at the time of discharge from occupational therapy services, she was preparing to participate in a job interview. Connie reported increased participation in sexual intimacy activities, improved communication with her partner, and prioritization of time and energy for engagement. Her Perceived Relationship Quality Components Inventory scores indicated improvement in the quality of her relationship with her partner. She also showed clinically meaningful improvement (≥2 points) across all selected areas of both the Performance and Satisfaction scales of the COPM, including communication with her partner. After honest and assertive conversations with her partner, Connie was able to increase her participation in home management IADLs from no more than light-intensity tasks 1 time per week to light- to moderate-intensity tasks 3 times per week. As a result of reduced overcompensation from her partner, she increased meal preparation IADLs from 1 time per day to 2 times per day. Table 6 summarizes her outcomes.
Connie’s Discharge Assessment Results
Note. COPM = Canadian Occupational Performance Measure; MSISQ = Multiple Sclerosis Intimacy and Sexuality Questionnaire; PRQC = Perceived Relationship Quality Components Inventory.
Case 2: Victor
Clinical Case Occupational Profile
Victor complains of significant sleep disruption, with anxiety and nocturia as primary contributing factors and, when he does not complete his stretching regimen during his evening sleep prep routine, spasticity that intermittently affects sleep. He identifies stretching and any steps he accumulates during chores and community outings as his primary method of physical activity engagement. Victor participates in physical therapy services to address lower extremity weakness, foot drop, and spasticity but reports difficulties with home exercise program consistency because of fatigue. He denies any self-regulation practices or routines to address anxiety. His strengths include a previous history of a consistent physical activity routine consisting of walking 2 to 3 miles per day and insight into factors contributing to occupational deficits. Victor is motivated to improve his sleep quality, increase participation in physical activity routines, and learn methods to better manage anxiety.
Occupational Therapy Initial Evaluation and Findings
On the basis of Victor’s primary complaints of falls, disrupted sleep, reduced physical activity participation, and deficits in self-regulation of anxiety, the occupational therapist administers the Godin Leisure Time Exercise Questionnaire (GLTEQ; Godin, 2011) and the Pittsburgh Sleep Quality Index (PSQI; Buysse et al., 1989). Victor’s self-reported number of falls was used to determine the impact of interventions on falls risk. The COPM was used to develop an occupational profile, support collaborative goal setting and intervention planning, and monitor change in perceived activity participation and occupational performance. Victor’s scores on these measures suggested considerable disruption to performance and participation in sleep, physical activity routines, and self-regulation routines (Table 7).
Victor’s Initial Assessment Results
Note. COPM = Canadian Occupational Performance Measure; GLTEQ = Godin Leisure Time Exercise Questionnaire; PSQI = Pittsburgh Sleep Quality Index.
On the basis of the initial assessment results, the occupational therapist and Victor developed the following goals for treatment: Victor will increase his participation in a structured sleep preparation routine from 0 to 4 of 7 nights to reduce sleep onset latency and increase sleep duration. Victor will increase participation in walking forms of physical activity health management from 0 to 3 of 7 days to improve conditioning and activity tolerance while reducing the risk of overexertion. Victor will increase participation in relaxation forms of self-regulation health management routines from 0 to 4 of 7 days to improve nervous system regulation and support sleep onset. Victor will improve self-management of weakness and spasticity secondary to MS as evidenced by reduced falls frequency during functional mobility ADLs in the home environment from 4 times per month to 1 time per month.
Occupational Therapy Intervention
Victor was seen onsite at an outpatient occupational therapy clinic at which two occupational therapists are members of a multidisciplinary team with the local MS comprehensive care center. In addition, he was seen via a telehealth platform that complies with the Health Insurance Portability and Accountability Act of 1996 (Pub. L. 104-191). He attended 12 outpatient occupational therapy sessions 2 times per week and 6 telehealth occupational therapy sessions 1 time per week.
The occupational therapist had background and training in the use of cognitive–behavioral therapy (CBT) principles and strategies to address sleep deficits and attends monthly multidisciplinary team meetings at the affiliated MS comprehensive care center, which supports coordinated and collaborative care.
Physical Activity Intervention for Falls Reduction
After communication with Victor’s physical therapist and guided by the physical activity algorithm in Figure 2, the occupational therapist teaches Victor a standardized series of exercises to reduce falls risk (Sosnoff et al., 2014) that do not contradict or duplicate his physical therapy home exercise program (97110— Therapeutic exercise). The training was completed onsite at the outpatient clinic. The exercises progressively increased in challenge over time through use of activity grading principles and focused on balance, lower limb muscle strength, core muscle strength, and stretching.
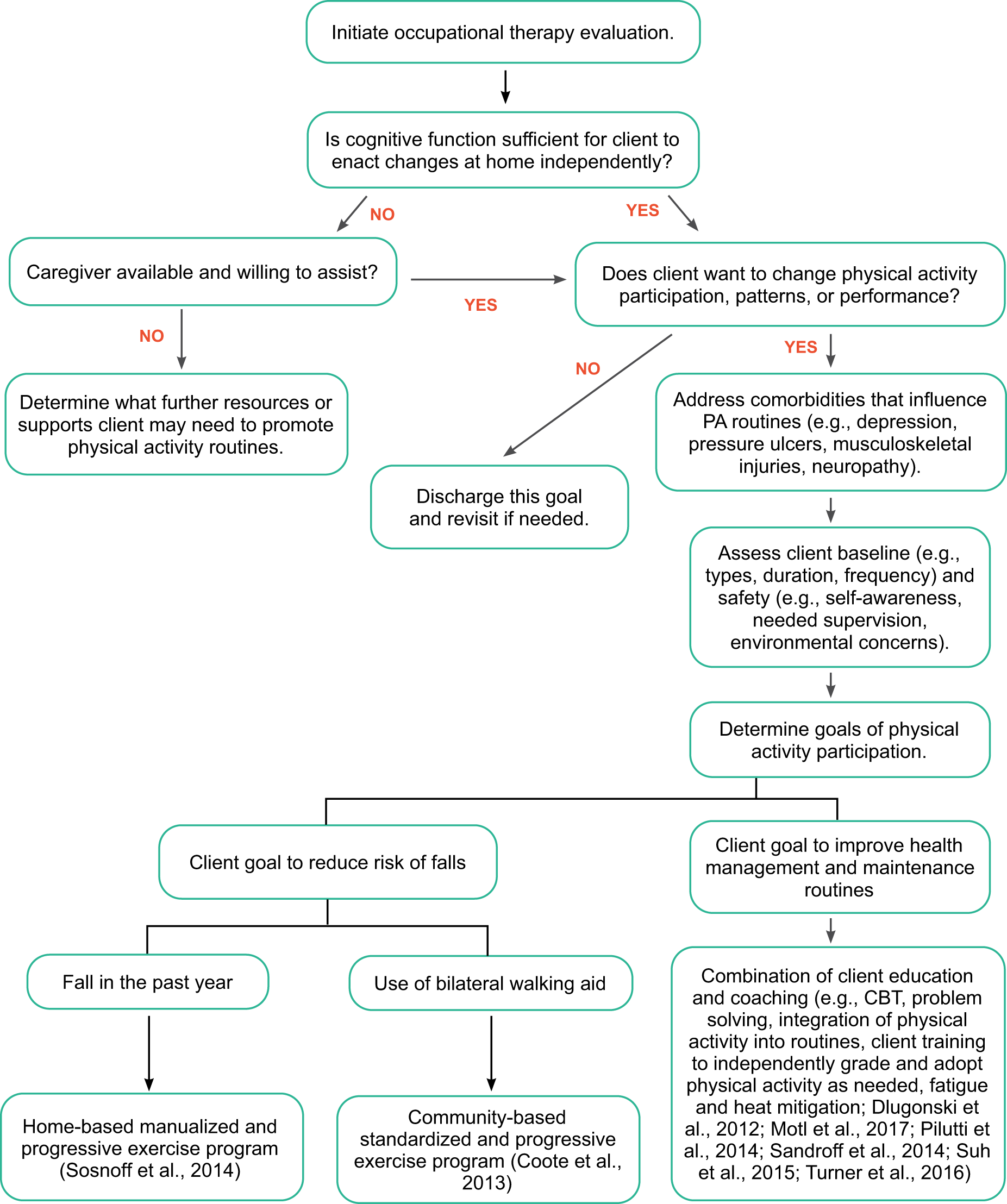
Interventions to improve or maintain physical activity for adults with MS.
The occupational therapist recommended that Victor complete the exercises 3 times per week at home and provided materials to support correct engagement and follow-through. A multicomponent intervention for physical activity was used to support carryover to the home context.
Multicomponent Intervention for Physical Activity Participation
To further support and improve Victor’s motivation for and engagement in physical activity, the occupational therapy practitioner provided telehealth-based educational materials related to physical activity and people with MS as well as coaching interventions (Turner et al., 2016). Over the course of six telehealth sessions to increase activity levels and improve compliance with his home exercise programs (97535—Self-care/home management), the occupational therapy practitioner collaborates with Victor to create functional physical activity goals, apply educational concepts (e.g., benefits of physical activity for MS, behavior change strategies), and develop a weekly plan and routine for physical activity that integrates Victor’s preferred form of physical activity, walking, and his home exercise program.
Individually Tailored Cognitive–Behavioral Therapy for Sleep
The occupational therapy practitioner uses an individualized CBT intervention (97535—Self-care/home management) to address Victor’s sleep deficits (Kiropoulos et al., 2016; Figure 3). Victor was trained to use the following CBT strategies: problem solving; scheduling pleasant activities; self-regulation practices (e.g., progressive muscle relaxation); and cognitive exercises to help identify, challenge, and manage unhelpful thoughts and beliefs that have a negative effect on sleep.
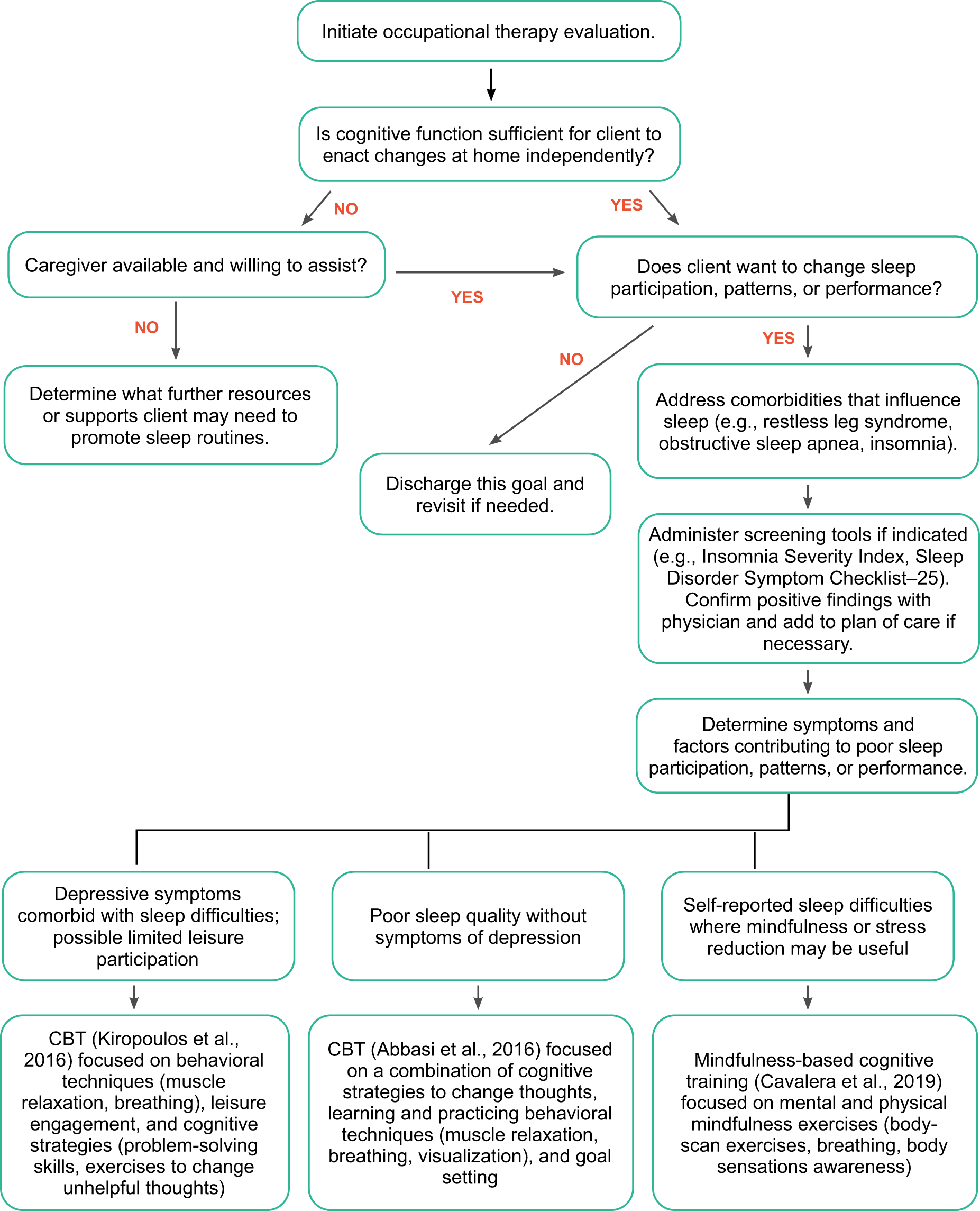
Interventions to improve sleep for adults with MS.
Because Victor identified sleep as his highest priority, the CBT intervention was used in the first eight sessions of the plan of care. Problem-solving skills were specifically used to address environmental factors affecting sleep. Scheduling strategies were used to support the consistent integration of a stretching regimen into Victor’s sleep prep routine and to more effectively manage spasticity. Cognitive exercises were used to address anxiety-driven thought patterns that contributed to sleep pressure and difficulties with sleep onset.
Online Group Mindfulness-Based Stress Reduction Intervention
The occupational therapist refers Victor to an online group mindfulness-based stress reduction (MBSR) program led by an occupational therapy colleague from the MS multidisciplinary team to support his goals to manage anxiety and improve sleep quality (Cavalera et al., 2019). The program consists of eight weekly sessions consisting of different mental and physical mindfulness exercises that use standardized MBSR core elements (97535—Self-care/home management): body‐scan exercises, mental exercises with a focus on breathing, physical exercises with a focus on being aware of bodily sensations and limits, and practice in being fully aware during everyday activities by using the breath as an anchor for attention.
Home exercises were facilitated with online multimedia content. Victor enrolled in the program and reported 8 wk of weekly participation beginning in Week 6 of his occupational therapy treatment. Victor and the occupational therapist address methods for integrating the body-scan and deep breathing exercises into his sleep prep routines to reduce sleep onset latency and improve sleep quality.
Outcomes
Victor improved on all outcome measures and met all his occupational therapy treatment goals. He reports an increase in sleep quality, improved participation in physical activity, and a reduced number of self-reported falls per month. In addition, he made clinically meaningful improvements (≥2 points) across all selected areas of the COPM for both Performance and Satisfaction, including self-regulation routines.
Victor walks 1.0 to 1.5 miles 4 days per week with good activity tolerance and has a plan to continue to slowly increase the challenge over time. He is also completing his home exercise program daily, which benefits his management of spasticity and weakness and reduces the risk of falls. Victor’s average sleep duration has increased from 5.5 hr to 7 hr per night, and he is taking no more than 30 min to fall asleep. Victor’s fall rate decreased from 4 times per month to 1 time per month. Table 8 summarizes his outcomes.
Victor’s Discharge Assessment Results
Note. COPM = Canadian Occupational Performance Measure; GLTEQ = Godin Leisure Time Exercise Questionnaire; PSQI = Pittsburgh Sleep Quality Index.
Strengths and Limitations of the Current Body of Evidence
These Practice Guidelines are based on the results of five systematic reviews that addressed specific clinical questions guided by an a priori question development and review process protocol. The current body of evidence has definite strengths and limitations related to these systematic reviews. No systematic review can address all aspects of a topic; authors must decide what to address before the review is conducted. In addition, no review is perfect, and there is always the chance for missed articles and related bias. The reduction in that bias comes from conducting a review using best-practice methodology.
Strengths
The authors have followed best-practice methodology at every step of the process, including getting input at all stages from practitioners, researchers, consumers, and experts in the areas included in the review. The review questions for the systematic reviews were developed with an intentional focus on occupation-based outcomes. Because the goal of occupational therapy is improvement in those outcomes, the systematic reviews targeted that level of intervention and outcome. AOTA also has existing specific reviews and practice guidelines for diagnoses such as stroke, Alzheimer’s disease, and arthritis. Those diagnoses were not included in this Practice Guideline to avoid overlap.
Limitations: Gaps in the Evidence
The majority of included studies involved samples that were predominantly female, including those related to caregiver involvement. Although the composition of the samples in most studies aligned with the 3:1 ratio of women to men in the MS community, the greater representation of female participants in the caregiver involvement study samples may not represent the demographics of the population of caregivers and could make it challenging to generalize findings to male caregivers of people with MS. The systematic review questions also focused on the effectiveness of interventions to improve and maintain performance and participation in different areas of occupation. Although prevention and preventive interventions are within the occupational therapy scope of practice and should be reimbursed, the questions did not include language addressing prevention or prevention-related interventions, which could limit the inclusion of pertinent articles across questions.
Gaps in knowledge exist when the literature contains insufficient, imprecise, inconsistent, or biased information about an intervention (Robinson et al., 2011). Gaps also exist when the literature is not sufficient to answer a clinical question. Therefore, practitioners must combine current evidence along with expert opinion and training to provide the best care possible.
Lack of research supporting particular interventions does not mean these interventions cannot be used. When working with clients when the evidence is insufficient to support evidence-based practice, occupational therapy practitioners should let their expert knowledge guide practice. This knowledge can come from their training or by connecting with experts in an area to gather expert opinion. We have pinpointed important gaps in evidence for interventions that we know practitioners are or should be considering using as appropriate.
Occupational therapy practitioners need to think about the elements of evidence-based practice as they evaluate this guideline in light of gaps related to clinical practice. Practitioners should consider the following questions when they identify these gaps (Gutenbrunner & Nugraha, 2020): What evidence exists? ▪ What are the best practices associated with providing client services? ▪ What interventions are contraindicated for my population? ▪ What outcomes am I hoping to achieve with this client? ▪ Does evidence exist in another field or discipline related to interventions and the desired outcomes that are within the scope of occupational therapy practice? What are my client’s preferences and values? ▪ Does my patient prefer one intervention over another? ▪ Are available resources, cost, or time influencing my client’s preference? ▪ How might the intervention I am considering affect my client’s performance patterns and roles? ▪ Does my client find the intervention I am considering meaningful? What experience and expertise do I have that can help guide my decisions? ▪ What types of interventions have I used previously that were effective with similar clients or populations? ▪ What types of interventions have I used previously that were ineffective with similar clients or populations? ▪ What potential risks does the intervention I am considering pose to my client or the population? ▪ Have the appropriate assessments been completed and documented to demonstrate my client’s need for this type of intervention? Will the health system or system organization be supportive of this intervention? ▪ How will I document this intervention? ▪ How will I document the outcomes associated with this intervention? ▪ Is it likely that this intervention will be reimbursed? ▪ Are there resources (e.g., equipment, supplies, expertise) in the practice setting to support this intervention?
Additional information and suggestions may be missing from the clinical recommendations of the systematic reviews as a result of insufficient, imprecise, inconsistent, or biased evidence. The following sections present additional information and suggestions related to occupational therapy’s role in addressing MS with adult clients. These sections are based on existing or emerging evidence, expert opinion, or both.
Fatigue Management Interventions
Fatigue is a subjective lack of energy that interferes with people’s usual and desired activities. It is experienced by 75% to 90% of people with MS, and 60% identify it as their most challenging symptom (Plow & Nicka, 2019). To adequately address fatigue, the MS literature suggests the use of a four-phase iterative process that includes identifying the presence of fatigue, screening for fatigue severity, comprehensively assessing fatigue, and delivering interventions that target primary and secondary factors that contribute to fatigue (Plow & Nicka, 2019). In addition to pharmacotherapy, behavior change interventions are recommended as the front-line nonpharmacological approach to reduce MS-related fatigue (Asano & Finlayson, 2014). More specifically, fatigue self-management interventions delivered by occupational therapy practitioners facilitate learning strategies and skills that reduce the impact of MS-related fatigue on daily activities (Ehde et al., 2015; Finlayson et al., 2011). As such, fatigue management interventions are recommended for delivery within an occupational therapy plan of care when working with people living with MS-related fatigue.
Interventions to Address Social and Emotional Regulation and Health Management and Maintenance
Research has suggested that stressful life events can contribute to the exacerbation of MS symptoms and the existence of new lesions in the brain and spinal cord (Lovera & Reza, 2013; Mohr et al., 2012). In addition, as many as 54% of people living with MS experience depression, 22% have an adjustment disorder within 2 mo of being diagnosed with MS, and the prevalence rate of generalized anxiety among people with MS is 18.6% (Khawam & Sacco, 2019). Emotional regulation interventions, such as mindfulness (Agland et al., 2018; Bogosian et al., 2015; Crescentini et al., 2018; Kolahkaj & Zargar, 2015), meditation (Agland et al., 2018; Cavalera et al., 2019), and breathing exercises (Artemiadis et al., 2012), have been studied in the population with MS and have been shown to have benefits for quality of life (Agland et al., 2018; Calandri et al., 2017; Cavalera et al., 2019), stress (Artemiadis et al., 2012; Bogosian et al., 2015; Kolahkaj & Zargar, 2015), depression (Artemiadis et al., 2012; Bogosian et al., 2015; Cavalera et al., 2019; Kolahkaj & Zargar, 2015), and anxiety (Bogosian et al., 2015; Cavalera et al., 2019; Crescentini et al., 2018; Kolahkaj & Zargar, 2015). As such, occupational therapy practitioners should consider emotional regulation interventions that support management of mood and reduce stress when working with people living with MS who have comorbid mental health diagnoses.
Cognition
Cognitive impairment occurs among 43% to 65% of people with MS and is commonly underrecognized or misdiagnosed as depression, stress, or a personality disorder (Rao, 2019). Cognitive difficulties contribute significantly to unemployment, motor vehicle accidents, challenges with ADLs, and loss of social contacts (Rao, 2019). Cognitive rehabilitation interventions and programs are designed to remediate abilities and support integration of compensatory strategies into daily activities. Recent research has highlighted rigorous randomized controlled trials that support the use of cognitive rehabilitation techniques in the population with MS (das Nair et al., 2016; Rosti-Otajärvi & Hämäläinen, 2014; Sandry et al., 2016), including the Story Memory Technique (Chiaravalloti et al., 2013) and computerized programs for retraining attention dysfunction (Amato et al., 2014; Cerasa et al., 2013). Occupational therapy practitioners should consider cognitive rehabilitation interventions and the integration of related strategies into daily occupations when working with people living with MS-related cognitive impairment.
Bowel and Bladder Management Interventions
Bladder dysfunction is reported by 50% of people with MS at the time of diagnosis and reported by 75% 6 yr after diagnosis (Moore, 2019). Bowel dysfunction occurs in as many as half of people living with MS. Fifty-three percent report constipation, and 29% to 51% report fecal incontinence (Moore, 2019). The MS literature identifies first-line interventions for urinary symptoms related to overactive bladder and storage deficits as behavioral strategies (e.g., modifying fluid routines, modifying timing of diuretic medication, scheduled voiding), dietary modifications (e.g., avoidance of bladder irritants), bladder retraining, and pelvic floor rehabilitation (Moore, 2019; Newman & Wein, 2009). In addition, to address urinary symptoms related to emptying deficits or urinary retention, intermittent catheterization is often the preferred method (Moore, 2019). Interventions to manage bowel symptoms include eliminating dietary irritants (Cotterill et al., 2018), high-fiber diet, adequate fluid intake, timed bowel regimen, incorporating fiber and bulking agents, and pelvic floor rehabilitation (Moore, 2019). These interventions are within the occupational therapy scope of practice and should be considered when working with people with MS to support adequate symptom management and the development of health management routines.
Caregiver Involvement
A caregiver is a person who helps with physical and psychological care for a person in need (Sullivan, 2019). Caregivers are often family members who are unpaid and spend more than 20 hr per week completing caregiving-related tasks (Sullivan, 2019). Caregivers are at risk of significant depression and anxiety, social isolation, lack of support from others, and reduced participation in preferred occupations (Buhse, 2008; Sullivan, 2019). The MS literature strongly encourages health care providers to refer caregivers to supportive programming and resources available from local or national-level organizations (Holland et al., 2011; Sullivan, 2019) to address health and well-being needs. Wellness programs that foster engagement in self-care, including physical activity, balanced nutrition, sufficient sleep and rest, social activities, leisure, and spiritual practices, are also recommended to support caregivers' physical and emotional health and quality of life (Holland et al., 2011; Sullivan, 2019). Because caregivers can be integral to the progress of the person living with MS, occupational therapy practitioners should consider offering referrals and resources to their clients’ caregivers to provide optimal care.
General Implications for Occupational Therapy
In addition to the specific intervention recommendations included in these guidelines, we include several general implications for occupational therapy with people with MS based on the MS-related literature and best-practice occupational therapy principles: ▪ Occupation as ends and means: The clinical recommendations demonstrate that engagement in physical activity can be the outcome of an intervention (Dlugonski et al., 2012; Motl et al., 2016; Pilutti et al., 2014; Sandroff et al., 2014; Suh et al., 2015; Turner et al., 2016), or it can serve as the means to reach a specific outcome (Coote et al., 2013; Sosnoff et al., 2014), thus highlighting the importance of viewing occupations as both means and ends. This could be a lens through which future systematic reviews can capture the full scope of research that aligns with the occupational therapy scope of practice. This lens could also be applied to other components of health management and maintenance, such as emotional regulation and symptom and condition management, to support addressing these areas in the population with MS. ▪ Coaching interventions to support health management and maintenance: The clinical recommendations highlight the benefits of independent coaching interventions based on Social Cognitive Theory, CBT, and motivational interviewing principles used independently (Bruce et al., 2016; Turner et al., 2014) and in a multicomponent intervention (Dlugonski et al., 2012; Motl et al., 2017; Pilutti et al., 2014; Sandroff et al., 2014; Suh et al., 2015; Turner et al., 2016) to improve health management and maintenance. Occupational therapy practitioners should consider additional training in these models to support integration of related interventions into practice. It may also be beneficial to explore application of these coaching models to other areas of health management, as well as participation in ADLs and IADLs, to support the development of habits and routines. ▪ Online or virtual service delivery methods: Multiple studies included in the clinical recommendations involved delivery of services through virtual (e.g., video or telephone) or online methods. Six studies used a combination of online and video or telephone methods to improve physical activity (Dlugonski et al., 2012; Motl et al., 2016; Pilutti et al., 2014; Sandroff et al., 2014; Suh et al., 2015; Turner et al., 2016). Two studies used telephone methods to improve medication management (Bruce et al., 2016; Turner et al., 2014); 2 used online methods to improve work self-efficacy (Dorstyn et al., 2017, 2018), and 1 used online methods to improve sleep (Cavalera et al., 2019). The growing use of virtual and online methods of service delivery is a meaningful trend in the MS literature because these methods support engagement in the therapeutic process while reducing barriers related to MS-related symptoms, such as fatigue. Occupational therapy practitioners should consider these methods of service delivery to support people with MS, especially in light of increased reimbursement of telehealth-based occupational therapy services during the coronavirus disease 2019 pandemic. ▪ Occupation-based performance assessment: On the basis of the findings of the systematic reviews, assessment of occupation-based outcomes continues to be limited in research on various interventions for people with MS. In addition to the use of self-report measures of function, occupational therapy practitioners should use objective, performance-based measures of occupational performance and participation to further support occupational therapy’s role with this population. To be more specific, the development of occupation-based outcomes that measure participation in a variety of health management and maintenance occupations, such as emotional regulation, symptom and condition management, and medication management, would benefit occupational therapy’s efforts to justify addressing these areas in an occupational therapy plan of care.
Conclusions
These Practice Guidelines highlight occupational therapy’s unique contribution to the clinical care of people with MS and their caregivers. They provide clinical recommendations based on current evidence and examples of application to clinical practice through case studies and decision-making algorithms (see Figures 1–3). They also address evidence gaps, determined by expert opinion and available evidence, for occupational therapy practitioners to consider when treating people with MS and their caregivers.
In summary, occupational therapy has a distinct and valuable role in supporting the participation, health, and well-being of people with MS and their caregivers. Occupational therapy practitioners consider a complex and unique set of factors that affect occupational performance and provide dynamic interventions. Therefore, practitioners can use these guidelines to integrate their professional experience and reasoning, client and caregiver preferences, and the best available research to provide the highest quality of care for people with MS and their caregivers. As the profession and care of people with MS continue to evolve, occupational therapy practitioners will need to use innovative service delivery models, develop educational opportunities to best prepare future practitioners, and advance research to provide best practice grounded in evidence, theory, and occupation.
Footnotes
1
Codes shown refer to CPT 2022 (American Medical Association, 2021, CPT 2022 Professional Edition, Chicago: American Medical Association Press) and do not represent all of the possible codes that may be used in occupational therapy evaluation and intervention. After 2022, refer to the current year’s CPT code book for available codes. CPT codes are updated annually and become effective January 1. CPT is a trademark of the American Medical Association. CPT five-digit codes, two-digit codes, modifiers, and descriptions are copyright © 2022 by the American Medical Association. All rights reserved.
*
Indicates articles included in the systematic reviews.
Appendix: Overview of Systematic Review Methods and Findings
The systematic reviews completed for this Practice Guideline were conducted according to the Cochrane Collaboration methodology (Higgins et al., 2019) and are reported consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2010).