
Abstract
This Practice Guideline provides a summary and applications of current evidence supporting a multidisciplinary, tailored, and goal-oriented intervention that is recommended for people with Parkinson’s disease. Case examples are presented along with suggested decision-making algorithms to support practitioners in addressing client goals.
Parkinson’s disease (PD) is a chronic, progressive neurodegenerative condition associated with progressive synucleinopathy, degeneration of nigrostriatal dopaminergic neurons, basal ganglia dysfunction, and widespread functional brain network disruptions. As a result of these neuropathological changes, people with PD experience myriad insidious motor and nonmotor signs and symptoms that can negatively affect their occupational performance, participation, and quality of life (QOL). Although the cause of PD remains largely unknown and there is no cure, treatment options are available to manage this complex and heterogeneous condition.
Approximately 1 million people in North America currently live with PD (Marras et al., 2018). This number is rising steeply as the population ages and life expectancy increases, making PD the fastest growing neurological disorder in the world (GBD 2016 Parkinson’s Disease Collaborators, 2018). Men are about 1.5 times more likely than women to be diagnosed with PD, and a majority of studies have reported the highest prevalence in White populations (Ben-Joseph et al., 2020; Wright Willis et al., 2010). The incidence of PD increases with age; the current average age at diagnosis is around age 60 yr. Thus, many people with PD have almost two full decades after diagnosis to fully live and experience life.
Each person with PD possesses a unique combination of signs and symptoms that can affect their well-being and ability to safely and independently engage in their desired occupations. PD is traditionally characterized by a complex set of motor signs including bradykinesia, akinesia, rigidity, tremor, and postural instability, which result in a decline in initiation, speed, and coordination of fine and gross motor function; impaired mobility; and speech and swallowing dysfunction. Despite the classification of PD as a movement disorder, a wide array of nonmotor manifestations are also associated with it, such as cognitive impairment, fatigue, neuropsychiatric concerns (e.g., depression, anxiety), sleep disturbances, sensory dysfunction (e.g., pain, loss of olfaction, visual problems), and autonomic disruptions. These nonmotor issues may appear earlier and have a greater impact on function and QOL than the motor signs (Martinez-Martin et al., 2011; Müller et al., 2013; Poewe, 2008).
People with PD have available a variety of treatment options for managing the multidimensional nature of their disease. One common approach is the use of a tailored and closely monitored medication regimen to control symptoms. Initially, people with PD experience a good response to medication. As the disease progresses, however, they may notice unpredictable changes in function because the medication wears off before they take the next dose (sometimes called on–off syndrome), and medications may become less effective over time. In addition, antiparkinsonian medications typically do not relieve the nonmotor symptoms and may even make them worse, and the long-standing use of such medications is frequently associated with negative side effects (e.g., dyskinesias, impulse control disorder, hallucinations). Surgery, such as deep brain stimulation or lesioning, is an option for people whose symptoms are not controlled effectively by medication or who are experiencing troublesome medication side effects. Regardless of the course of the disease and the combination of treatment, people with PD and their care partners need a multidisciplinary, client- and family-centered approach to best address their unique needs (Qamar et al., 2017; Radder et al., 2017; van der Marck et al., 2009).
“Achieving health, well-being, and participation in life through engagement in occupation” summarizes the domain and process of occupational therapy in its fullest sense (American Occupational Therapy Association [AOTA], 2020, p. 5). The role of occupational therapy practitioners in the care of people with PD is to promote their engagement in meaningful tasks, activities, and roles in the home and community (Foster et al., 2014; Jansa & Aragon, 2015; Radder et al., 2017). Limitations in daily activities among people with PD can occur soon after diagnosis and typically progress over the course of the disease (Schenkman et al., 2011). Occupational performance problems can stem from any number or combination of factors, including motor and nonmotor impairments, medication regimens, and environmental barriers. The varied and unique presentation of PD across individuals requires practitioners to combine a client-centered approach to assessment and intervention with models of practice (e.g., Model of Human Occupation, Person–Environment–Occupation–Performance Model) and theoretical models (e.g., motor learning, challenge point framework) to address this complex condition (Jansa & Aragon, 2015).
Treatment goals may differ over the progression of the disease within and across individuals. For example, in the early stages of PD, occupational therapy intervention may be directed toward self-management, prevention of reduced participation in roles and activities, and enhancement of activity performance. In the middle and later stages of PD, occupational therapy intervention may shift focus toward adaptation and compensation to preserve engagement and independence in meaningful activities. Over the course of the disease, practitioners continually assess the environment, other contextual factors, and task demands and modify them as necessary to support the client’s optimal safety, independence, comfort, and satisfaction in daily occupational performance. In addition, they play a role in supporting care partners to appropriately assist the person with PD in daily activities while remaining mindful of their own needs to maintain well-being (Radder et al., 2017).
Although people with PD and their care partners desire nonmedical interventions, and although growing evidence supports the role of occupational therapy in the management of PD, occupational therapy services are underutilized by this population in the United States. A claims-based study identified 174,643 Medicare beneficiaries with a diagnosis of PD and followed them from 2007 to 2009, tracking annual receipt of physical, occupational, and speech therapy services (Fullard et al., 2017). In 2007, only 14.2% of beneficiaries with PD had claims for physical or occupational therapy, and this rate showed a small decline from 2007 to 2009. In contrast, rehabilitation utilization rates among people with PD in the Netherlands and the United Kingdom were more than 50% around that time period (Fullard et al., 2017; Jansa et al., 2011; Keus et al., 2004). Furthermore, a survey of the experiences and views of people with PD in four European countries found that of those who had received occupational therapy services since their diagnosis, almost all would recommend occupational therapy to other people with PD (Jansa et al., 2011). Clear, evidence-based, and practical guidelines may help fill the gap between the perceived value and actual utilization of occupational therapy by people with PD in the United States.
The current Practice Guideline updates the PD portion of the Occupational Therapy Practice Guidelines for Adults With Neurodegenerative Diseases (Preissner, 2014). Those guidelines, which were based on a systematic review of occupational therapy–related interventions for adults with PD (Foster et al., 2014), discussed three categories of interventions: (1) exercise or physical activity; (2) environmental cues, stimuli, and objects; and (3) self-management and cognitive– behavioral strategies. The clinical recommendations for PD included supporting clients’ engagement in exercise and physical activity to improve their performance skills and occupational performance, specifically through (1) multisession repetitive physical exercise to improve balance, postural stability, and motor performance and (2) complex and multimodal activity (e.g., tango dancing) to improve functional movement. Other review findings indicated that specialized or more intense exercise can improve performance to a greater extent than traditional or less-intense exercise, task-specific interventions can improve skill development, tai chi can enhance motor and postural performance skills, and multimodal physical activity can improve cognitive performance. The previous guidelines also recommended the use of external cues during movement and activities of daily living (ADLs) to improve task and occupational performance, with auditory rhythmic external cues being most effective for walking. Finally, the guidelines recommended individualized interventions focused on wellness and personal control through self-management and cognitive–behavioral strategies to improve QOL.
At the time of the prior Practice Guideline (Preissner, 2014), research focused on interventions and outcomes for people with PD at the physical activity and impairment level, on one hand, and related occupation-based interventions and outcomes, on the other, was just beginning to emerge. The literature has since evolved, and the set of systematic reviews that informed the current Practice Guidelines updated and expanded on the prior evidence. Three of the systematic reviews examined outcomes of interest in three occupational domains: ADLs, rest, and sleep (Doucet et al., 2021); instrumental activities of daily living (IADLs; Foster et al., 2021); and education, work, volunteering, leisure, and social participation (Reiling Ott & Kolodziejczak, 2020), and one focused on interventions for caregivers of people with PD (Boone et al., 2021). Thus, this Practice Guideline incorporates enhanced and additional evidence to support occupational therapy practice with adults with PD. The information in this Practice Guideline reflects the current state of the research for interventions within the scope of occupational therapy for people with PD and their caregivers and can be used to support evidence-based practice.
Systematic Review Questions
This Practice Guideline is based on the following four questions: What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve or maintain performance and participation in ADLs and rest and sleep for adults with PD (Doucet et al., 2021)? What is the evidence for the effectiveness of interventions within the scope of occupational therapy to improve or maintain performance and participation in IADLs for adults with PD (Foster et al., 2021)? What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve or maintain the performance of and participation in education, work, volunteering, leisure, and social participation among adults with PD (Reiling Ott & Kolodziejczak, 2020)? What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice for caregivers of people with PD to facilitate or maintain their participation in the caregiver role (Boone et al., 2021)?
Goals of This Practice Guideline
Through this Practice Guideline, AOTA aims to help occupational therapy practitioners, as well as the people who manage, reimburse, or set policy regarding occupational therapy services, understand occupational therapy’s contribution in providing services to people with PD and their care partners. This guideline can also serve as a reference for health care professionals, health care facility managers, education professionals, education and health care regulators, third-party payers, managed care organizations, and those who conduct research to advance care of people with PD.
This Practice Guideline was commissioned, edited, and endorsed by AOTA without external funding being sought or obtained. It was financially supported entirely by AOTA and was developed without any involvement of industry. All authors of the reviews completed conflict-of-interest disclosure forms, with no conflicts noted. AOTA reviews practice guidelines, and updates them as needed, every 5 years to keep recommendations on each topic current according to criteria established by ECRI (2021). Guideline topics are evaluated by a multidisciplinary advisory group consisting of AOTA members, nonmember content experts, and external stakeholders. This Practice Guideline was reviewed and revised on the basis of feedback from a group of content experts on people with PD that included practitioners, researchers, educators, practitioners, and policy experts. Reviewers who agreed to be identified are listed in the Acknowledgments.
This Practice Guideline reports the findings from systematic reviews of published scientific research on focused topic-specific questions. The systematic reviews were conducted according to the Cochrane Collaboration methodology (Higgins et al., 2019) and are reported according to the PRISMA guidelines for conducting systematic reviews (Moher et al., 2009). The protocol and questions were developed with input from a multidisciplinary advisory group that also included consumers and information end users. A medical research librarian conducted searches of the literature, and review teams evaluated the search results and synthesized the findings (see the Appendix for an overview of the systematic review methods and findings). Interventions that were described in sources other than the published literature and that did not meet the inclusion criteria were excluded from the reviews.
Occupational therapy practitioners should not consider this Practice Guideline to be a source of comprehensive information about PD or about application of the occupational therapy process. The occupational therapist makes the ultimate clinical judgment regarding the appropriateness of a given intervention in light of a specific client’s or group’s circumstances, needs, and response to intervention, as well as the evidence available to support the intervention. Examples of how evidence can inform practice with people with PD are included in the “Clinical Case Studies and Algorithms” section.
AOTA supported the systematic reviews on the effectiveness of interventions within the scope of occupational therapy for people with PD as part of its Evidence-Based Practice (EBP) Project. AOTA’s EBP Project is based on the principle that the evidence-based practice of occupational therapy relies on the integration of information from three sources: (1) clinical experience and reasoning, (2) preferences of clients and their families, and (3) findings from the best available research. The systematic reviews and this Practice Guideline report the findings from the best available research.
Clinical Recommendations for Occupational Therapy Interventions for People With Parkinson’s Disease
Clinical recommendations are the final phase of the synthesis of systematic review findings. The findings for each systematic review question are graded in terms of how confident a practitioner can feel that using the interventions presented in the evidence will improve the outcomes of interest to their clients. The grade is based on the specificity of the intervention, number of studies supporting the intervention, levels of evidence of the studies, quality of the studies, and significance of the study findings. Interventions included in the clinical recommendations are specific to a population, and the articles that describe them provide sufficient detail for practitioners to understand the intervention and the outcomes of interest.
Describing the strength of clinical recommendations is an important part of communicating an intervention’s efficacy to practitioners and other users. The recommendations for this practice guideline were evaluated and finalized by AOTA staff, the AOTA research methodologist, and systematic review and practice guideline authors. AOTA uses the grading methodology provided by the U.S. Preventive Services Task Force (2018) for clinical recommendations. The clinical recommendations pertaining to each review, along with the studies’ level of evidence and supporting details, are presented in Tables 1–3. No strong or moderate clinical recommendations emerged from the systematic review on caregiver interventions, so there is no corresponding table.
Clinical Recommendations and Supporting Evidence: Interventions to Address ADLs, Sleep, and Rest for People With PD
Note. All studies had statistically significant positive outcomes related to the interventions discussed. ABC Scale = Activities-specific Balance Confidence Scale; ADLs = activities of daily living; BBS = Berg Balance Scale; BDNF = brain-derived neurotrophic factor; CBT = cognitive–behavioral therapy; CS–PFP = Continuous Scale–Physical Functional Performance; DASS–21 = Depression, Anxiety and Stress Scale–21 Items; DextQ–24 = Dexterity Questionnaire 24; ESS = Epworth Sleepiness Scale; FES = Tinetti Falls Efficacy Scale; FRT = Functional Reach Test; FSS = Fatigue Severity Scale; HR = heart rate; H&Y = Hoehn & Yahr Scale; IADLs = instrumental activities of daily living; IRT = intensive rehabilitation treatment; ISI = Insomnia Severity Index; MBSR = mindfulness-based stress reduction; MDS–UPDRS = Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (I = nonmotor ADLs; II = motor ADLs; III = motor skills); Mini-BEST = Mini Balance Evaluation Systems Test; MIRT = multidisciplinary intensive rehabilitation treatment; MMBCEP = mindfulness meditation–based complex exercise program; MSQ = Mini-Sleep Questionnaire; 9HPT = Nine-Hole Peg Test; NR = not reported; OT = occupational therapy; PDDS = Parkinson’s Disease Disability Scale; PDQ–39 = Parkinson’s Disease Questionnaire; PDQL = Parkinson’s Disease Quality of Life Questionnaire; PDSS = Parkinson’s Disease Sleep Scale; PHQ–9 = Patient Health Questionnaire–9; PIRS20 = Pittsburgh Insomnia Rating Scale; PPDS = Parkinson’s Disease Disability Scale; PPT = Physical Performance Test; PSQI = Pittsburgh Sleep Quality Index; PT = physical therapy; SE-ADL Scale = Schwab and England Activities of Daily Living Scale; ST = speech therapy; TUG = Timed Up and Go test; UPDRS = Unified Parkinson’s Disease Rating Scale (II = ADLs; III = motor skills; IB = nonmotor experiences rated by patient with or without caregiver).
Clinical Recommendations and Supporting Evidence: Interventions to Address IADLs for People With PD
Note. All studies had statistically significant positive outcomes related to the interventions discussed. ACS = Activity Card Sort; IADLs = instrumental activities of daily living; IPAQ = International Physical Activity Questionnaire; MDS–UPDRS = Movement Disorder Society–Unified Parkinson’s Disease Rating Scale; MMAS–4 = Morisky Medication Adherence Scale–4; PASS = Physical Activity Status Scale; PD = Parkinson’s disease; SOS = Systematic Screening of Handwriting Difficulties.
Clinical Recommendations and Supporting Evidence: Interventions to Address Participation in Education, Work, Volunteering, Leisure, and Social Participation Among People With PD
Note. This study had statistically significant positive outcomes related to the intervention discussed. PD = Parkinson’s disease.
For the purposes of this Practice Guideline, we report recommendations graded A, B, and D, the grades that best support clinical decision making: A: There is strong evidence that occupational therapy practitioners should routinely provide the intervention to eligible clients. Strong evidence was found that the intervention improves important outcomes and that benefits substantially outweigh harms. B: There is moderate evidence that occupational therapy practitioners should routinely provide the intervention to eligible clients. There is high certainty that the net benefit is moderate, or there is moderate certainty that the net benefit is moderate to substantial. D: It is recommended that occupational therapy practitioners not provide the intervention to eligible clients. At least fair evidence was found that the intervention is ineffective or that harms outweigh benefits. In these reviews, we did not find Grade D evidence.
These grades are reported in Tables 1–3 and designated with green, indicating should consider if appropriate (A), or yellow, indicating could consider if appropriate (B). None of the studies included in these reviews reported adverse events or harms related to the interventions evaluated (D).
The complete findings from the systematic reviews can be found in the applicable articles in the American Journal of Occupational Therapy (Boone et al., 2021; Doucet et al., 2021; Foster et al., 2021) and the Critically Appraised Topic (Reiling Ott & Kolodziejczak, 2020). As always, practitioners’ clinical decisions should be informed by the evidence presented in this Practice Guideline, in combination with their clinical experience and the client’s particular goals.
Translating Clinical Recommendations Into Practice
Clinical Reasoning Considerations
The purpose of clinical practice guidelines is to help practitioners translate pertinent research findings from systematic reviews into practice. Very rarely will practitioners find an evidence-based intervention that perfectly fits their clinical setting and the client’s specific needs. Occupational therapy practitioners need to consider several questions as they evaluate the research and consider whether they can use an intervention, or adapt it in a well-reasoned way, to exact meet the client’s needs (Highfield et al., 2015): Exactly what intervention do I need to provide? What types of client outcomes am I looking for? Do the studies I’ve located provide enough detail on the intervention so that I know what to do and how to do it? How well do the conditions in which I will provide the intervention match those in the studies? What are the demographic characteristics (e.g., age, gender, diagnosis, comorbidities) of the participants in the research studies? In which setting (e.g., inpatient, home, community, school) did the studies take place? Do any contextual factors (e.g., resources, policies) that are different from those in the studies influence my ability to provide the intervention? How flexible is the intervention, and how much can I modify or adapt it? If my setting or client population differs from those of the studies, can I modify or adapt the intervention without changing its integrity? If I modify or adapt the intervention, what client characteristics (e.g., comorbidities) do I need to consider? Can I be proactive and plan how to modify or adapt the intervention before I start implementing it? Can I make minimal changes to the intervention, such as reordering the content of the sessions, or does the need for substantial changes indicate I should select another intervention?
To modify or adapt evidence-based interventions in practice, practitioners must plan and proactively think through the changes they need to make to fit the intervention to the client and practice setting. In addition, they must document how and why they altered the researched intervention so others in their setting know how to implement the intervention and why the changes were made. If an intervention must be adapted extensively, it may not be the right fit for the situation. When practitioners adapt an intervention, it is no longer evidence based, but rather evidence informed. If extensive adaptations to the intervention are necessary, the intervention is probably not right for the client or setting. If the practitioner finds that the intervention does not suit the client, they should not use that intervention. Clinical interventions should be as similar as possible to the interventions used in the research.
Clinical Case Studies and Algorithms
The case studies in this section illustrate how occupational therapy practitioners can translate evidence from the systematic reviews to professional practice when collaborating with people with PD across the continuum of care. Each case study highlights interventions that are supported by evidence and expert opinion. The case studies contain decision-making algorithms developed by the authors and AOTA staff on the basis of the clinical recommendations; each algorithm includes decision points and actions for practitioners to take. We provide a CPT ® billing code 1 (American Medical Association, 2021) for each intervention to aid translation to professional practice.
Occupational therapy practitioners can use these algorithms to inform their own clinical decision making, as appropriate. Practitioners must consider each potential intervention in relation to the client’s individual goals, interests, habits, routines, and environment and choose interventions that strongly align with or are supportive of these factors in the context of the client’s occupational profile. It is important to note that the algorithms in this Practice Guideline present simplified examples of the decision-making processes occupational therapy practitioners might use to address their specific clients’ goals.
Case Study 1: Steven
Occupational Profile
Occupational Therapy Initial Evaluation and Findings
On the basis of Steven’s primary complaints of disrupted sleep and fatigue, the occupational therapist administered the Parkinson’s Disease Sleep Scale second edition (PDSS–2; Trenkwalder et al., 2011) and the Fatigue Severity Scale (Friedman et al., 2010) to quantify the sleep disruption and fatigue he was experiencing. The therapist created a nonstandardized sleep log for Steven to track his bedtime, wake time, and estimated number of times he woke during the night. The therapist also used the Activity Card Sort (Baum & Edwards, 2008) and the Canadian Occupational Performance Measure (COPM; Law et al., 2014) to develop an occupational profile (AOTA, 2021), support Steven in setting client-centered goals, inform intervention planning, and monitor change in Steven’s perceived activity participation and occupational performance during treatment. Steven’s COPM scores indicated he was experiencing considerable disruption in his performance of and participation in IADLs and leisure and social activities because of disrupted sleep and significant fatigue. Table 4 summarizes Steven’s initial assessment results.
Steven’s Initial Assessment Results
On the basis of Steven’s assessment results, the occupational therapist and Steven developed the following treatment goals: Steven will improve his ability to fall asleep and report a decrease in nightly sleep disruptions with use of mindfulness and complex exercise. Steven will report a reduction in severity of fatigue with use of fatigue management strategies and improvements in physical activity and sleep. Steven will demonstrate the ability to use computer applications of his choice to enhance social participation using compensatory strategies and aids to support computer use. Steven will complete meal preparation and cleaning tasks using task-oriented and fatigue management strategies. Steven will demonstrate engagement in physical activity 5 of 7 days per week by discharge to improve sleep and promote symptom management, tracking his activity with a fitness log.
Occupational Therapy Interventions
Steven received occupational therapy in a multidisciplinary center specializing in outpatient occupational, physical, and speech therapy for people with neurological movement disorders. He attended sessions 3 times per week for 8 wk. The occupational therapist selected a tailored goal-oriented multicomponent approach to intervention (Sturkenboom et al., 2014) that included self-management techniques to address Steven’s sleep, fatigue, and physical activity levels and task-specific training and compensatory strategies to support meal preparation, cleaning, and email use.
The occupational therapist had background and training in use of cognitive–behavioral therapy techniques and mindfulness meditation and maintained a network of community engagement opportunities for client referral. The occupational therapist collaborated with Steven’s physical therapist, who assessed his balance, to select appropriate exercise options for Steven to include in the behavioral change intervention.
Mindfulness Meditation–Based Complex Exercise Program
After reviewing the sleep algorithm in Figure 1, the occupational therapy practitioner selected a mindfulness meditation–based complex exercise program (Son & Choi, 2018) to address Steven’s sleep, fatigue, and physical activity goals (97530—Therapeutic activities). The program included strength, endurance, coordination, and flexibility exercises combined with meditation exercises. Steven’s training included warm-up stretches, elastic band exercises for the upper and lower extremities, ball exercises, and breath and mindfulness meditation training.
ParkFit
The occupational therapist, after reviewing and guided by the functional mobility algorithm in Figure 2, selected the ParkFit program (van Nimwegen et al., 2013) to support and improve Steven’s motivation to engage in physical activity. ParkFit is an individually tailored, multifaceted behavioral change program designed to target and increase physical activity levels (97350—Therapeutic activities). The ParkFit program provides clients with an educational brochure about physical activity and PD, personalized activity coaching sessions, individualized goal setting, coping planning, and motivation to participate in exercise. The therapist collaborated with Steven to create a daily plan for physical activity to improve his compliance with the home exercise program and increase his activity level. The therapist also gave Steven an ambulatory monitor to provide feedback on his daily physical activity levels.
Community Tango Class
The occupational therapist referred Steven to a local community tango class to support his goals for physical activity, social engagement, and IADL participation (Foster et al., 2013). The occupational therapist encouraged Steven to communicate with the tango instructor via email to practice his email skills. Steven signed up for the class and reported weekly participation beginning in Week 3 of his occupational therapy treatment.
Task-Specific Training, Self-Management, and Compensatory Strategies
The occupational therapist incorporated several individually tailored approaches to address Steven’s fatigue, social engagement, and IADL goals (Sturkenboom et al., 2014; 97535—Self-care/home management). The occupational therapist trained Steven to use email and the internet to communicate with former colleagues, friends, and family and to find out about local activities and events. The therapist provided task-specific training incorporating use of a variety of keyboards, mouse types, and accessibility settings to optimize Steven’s performance. Steven practiced sending emails to the therapist, family, and friends during his occupational therapy sessions, and the occupational therapist provided feedback.
The occupational therapist educated Steven in the use of fatigue management strategies (Kluger, 2017). The practitioner stressed the use of planning and pacing strategies to prevent extreme fatigue and trained Steven trained to use a daily planner to organize his day and balance activities and rest. The therapist educated Steven in the use of strategies to simplify meal preparation and cleaning tasks.
Outcomes
Steven attended 22 of 24 outpatient occupational therapy sessions. He improved in all outcome measures and met all of his occupational therapy treatment goals. Steven’s PDSS–2 scores and sleep journal showed a reduction in fragmented sleep, improved ability to manage his fatigue and daytime sleepiness, and clinically meaningful improvements (≥2 points) in COPM Performance and Satisfaction scores. Table 5 summarizes his outcomes.
Steven’s Discharge Assessment Results
Case Study 2: Linda
Occupational Profile
Occupational Therapy Initial Evaluation and Findings
During the evaluation, Linda reported fear of falling and concern for her safety during kitchen mobility. She demonstrated upper extremity tremor, bradykinesia, and rigidity and reported difficulty using her arms and hands in daily tasks, resulting in extended time needed for dressing tasks and difficulty with fine motor coordination. She reported needing occasional assistance from her partner to thread her arms into jacket sleeves and don and doff garments over her head; the growing need for assistance from her partner makes her feel “dependent.” She demonstrated micrographia when completing clinical forms and complained of difficulty reading her own writing when making lists at home. She reported medication management problems; she often missed her midday dose of dopaminergic medications when she was not at home, which resulted in it wearing off and increased episodes of freezing of gait. She also reported decreased participation in meal preparation tasks because of her episodes of freezing of gait and related fear of falling.
The occupational therapist administered the Activities-specific Balance Confidence Scale (Powell & Myers, 1995) to further explore Linda’s fear of falling. The therapist used the Patient-Specific Functional Scale (Stratford et al., 1995) to identify and quantify Linda’s activity limitations and assist in setting client-centered goals. Linda identified zipper manipulation, jewelry fastening, upper body dressing, handwriting, and medication management as important areas for improvement. The therapist used a timed assessment of upper body dressing and jewelry fastening to provide an objective baseline measure of ADL performance. The therapist also provided Linda with a log to record how long it took her to perform these tasks on a daily basis. Linda’s scores on these measures indicate reduced efficiency and decreased independence in ADL tasks. Table 6 summarizes Linda’s initial assessment results.
Linda’s Initial Assessment Results
On the basis of Linda’s initial assessment results, the occupational therapist and Linda developed the following goals for treatment: Linda will demonstrate increased efficiency in dressing tasks with use of large-amplitude, task-specific strategies to support manipulation of clothing and jewelry fasteners. Linda will demonstrate increased size and legibility in handwriting with use of visual targets and home practice to support participation in work, bill paying, and shopping tasks. Linda will use strategies and environmental cues to manage three out of four episodes of freezing of gait to prevent falls, reduce fear of falling, and improve safety. Linda will engage in regular physical activity (at least 40 min, at least 2×/wk) to support symptom management and improve or maintain ADL function and functional mobility. Linda will demonstrate accurate compliance with her dopaminergic medication regimen 7 out of 7 days per week to support symptom management.
Occupational Therapy Interventions
Linda was referred to home-based outpatient occupational therapy services after discharge from an inpatient stay. Linda’s plan of care includes physical therapy 2×/wk and occupational therapy 3×/wk to continue multidisciplinary care to improve her ADL performance. One occupational therapy session each week is conducted by an occupational therapy assistant. The occupational therapy and physical therapy practitioners collaborate to provide multicomponent interventions to address Linda’s goals. They use task-specific training to address specific problematic ADLs and IADLs (e.g., upper body dressing, handwriting; Foster et al., 2021), exercise to address general ADL function (Doucet et al., 2021), and environmental modifications and external cues to address functional mobility (Foster et al., 2014). In addition, the occupational therapy team uses a cognitive–behavioral approach to address medication adherence (Daley et al., 2014).
Five days per week of therapy services was a departure from the norm, but the therapy team felt that research evidence (Doucet et al., 2021 ; Foster et al., 2021) on the need for intensity and repetition of practice supported a more intensive plan of care to increase Linda’s safety and independence. The occupational therapist and physical therapist reviewed the handwriting algorithm in Figure 3 and the ADL algorithm in Figure 4 and collaborated to develop Linda’s plan of care, focusing on different yet complementary aspects of assessment and intervention. Throughout Linda’s care, both practitioners communicated and supported the other practitioner’s instructions and strategies to provide consistent cues to address her freezing of gait and functional mobility (Radder et al., 2017).
Task-Specific Training
The occupational therapy assistant provided training and practice in strategies to support Linda’s handwriting performance, including the use of visual stimuli (e.g., colored target zones, lines) to provide external cues to support writing size and legibility (Nackaerts et al., 2016; Ziliotto et al., 2015; 97530—Therapeutic activities). After two 30-min sessions, the occupational therapy assistant provided Linda with a workbook with hand exercises and writing activities (e.g., cued, free writing, copying shapes, writing a postcard) and recommended Linda practice on her own 1 hr 2×/wk (Collett et al., 2017).
For the first 4 wk, the occupational therapist and physical therapist provided Linda with four 60-min sessions per week of task-specific training using the LSVT BIG® protocol (Fox et al., 2012; LSVT BIG, n.d.). The goals were to improve Linda’s performance of ADL tasks (zipper manipulation, jewelry fastening, upper body dressing) and kitchen mobility (97112—Neuromuscular reeducation, 97530—Therapeutic activities). During LSVT BIG training, Linda performed exercise and functional tasks while applying large-amplitude strategies to support her performance. In addition, Linda completed exercises, functional components, and carryover tasks at home every day, tracking them in her log.
Medication Adherence Therapy
After obtaining Linda’s prescribed medication regimen from her movement disorder specialist, the occupational therapy assistant addressed medication management with Linda and her partner by reviewing her medication, including her beliefs and attitudes about it (Daley et al., 2014; 97535—Self-care/home management). The assistant provided education on taking medication at the correct time intervals and reassured her that the medication would improve Linda’s symptoms and reduce her freezing of gait and risk of falling. Together they developed practical solutions to improve her adherence, including setting a daily timer on her phone for her midday dose and keeping a small vial of backup pills in her purse for when she is out. Linda collaborated with the assistant to create a medication log to track all her daily doses.
Physical Activity
During a discussion of the importance of exercise for people with PD, Linda mentioned that she had enjoyed doing Wii exercises while in inpatient rehabilitation and that her partner had a Wii system (Nintendo, Kyoto, Japan; see Figure 2). The occupational therapist recommended exercising using the Wii for at least 40 min 2×/wk (Herz et al., 2013).
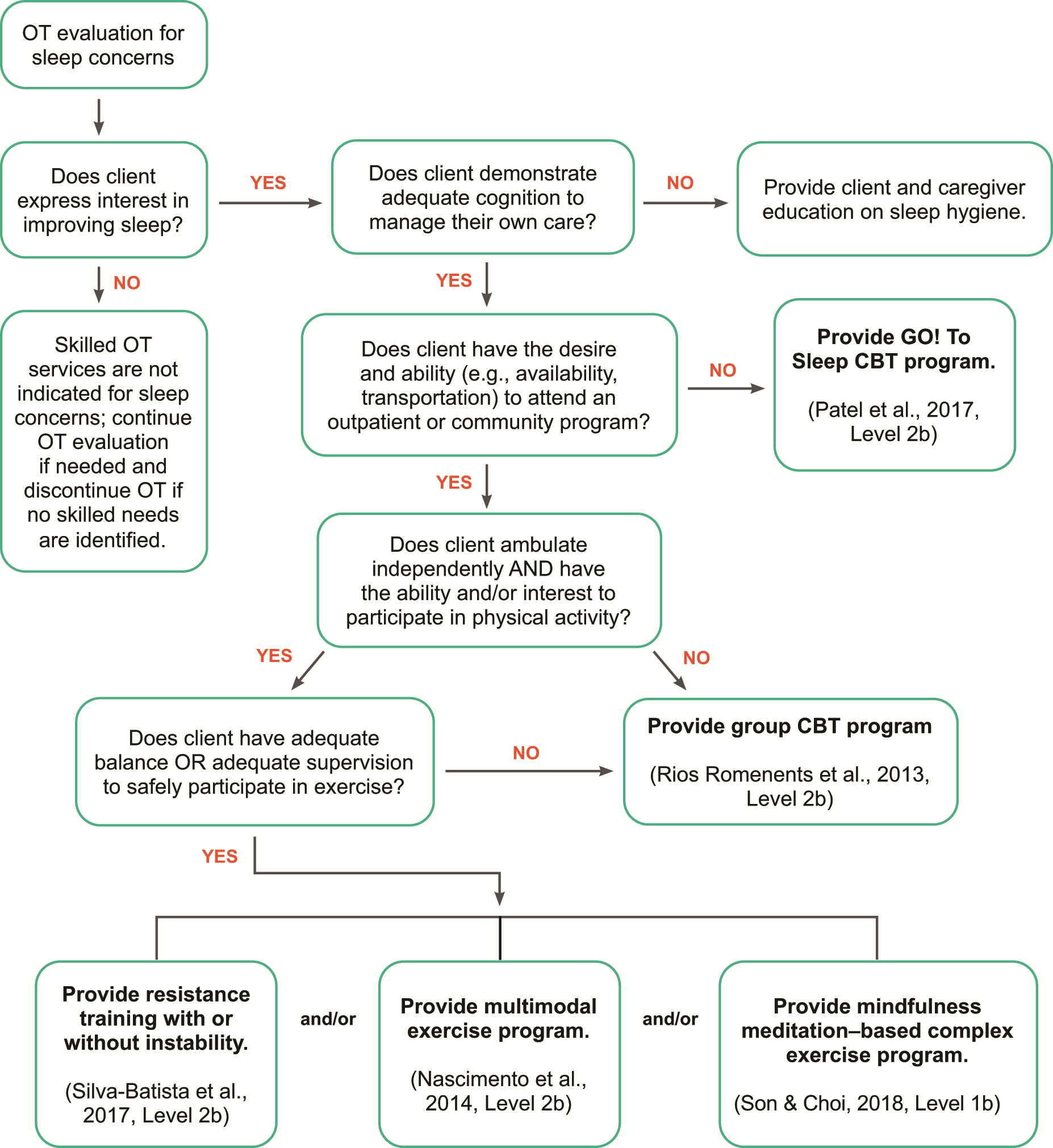
Decision-making algorithm for interventions to improve sleep and rest for people with Parkinson’s disease.
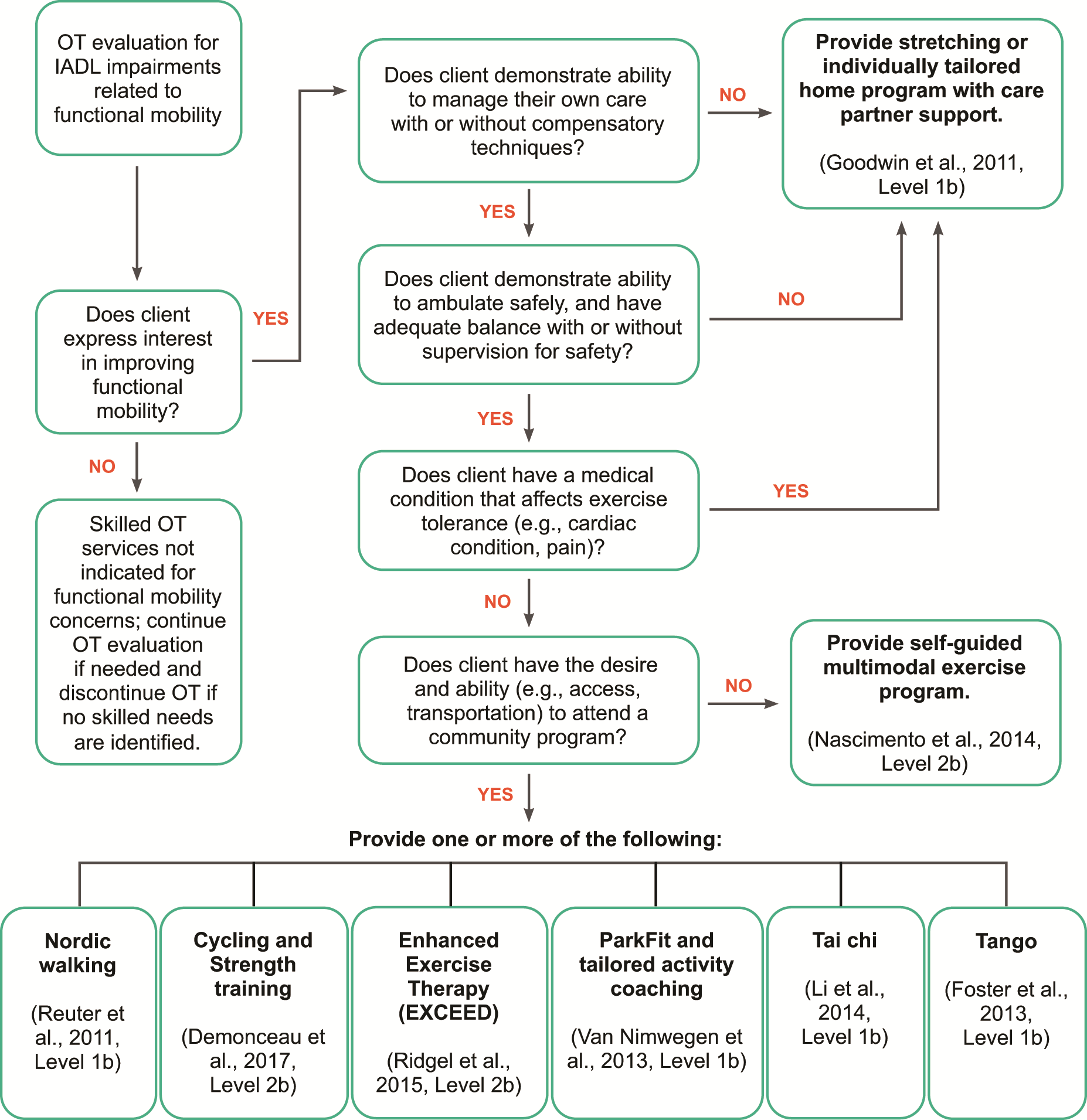
Decision-making algorithm for interventions incorporating physical activity to improve functional mobility for people with Parkinson’s disease.
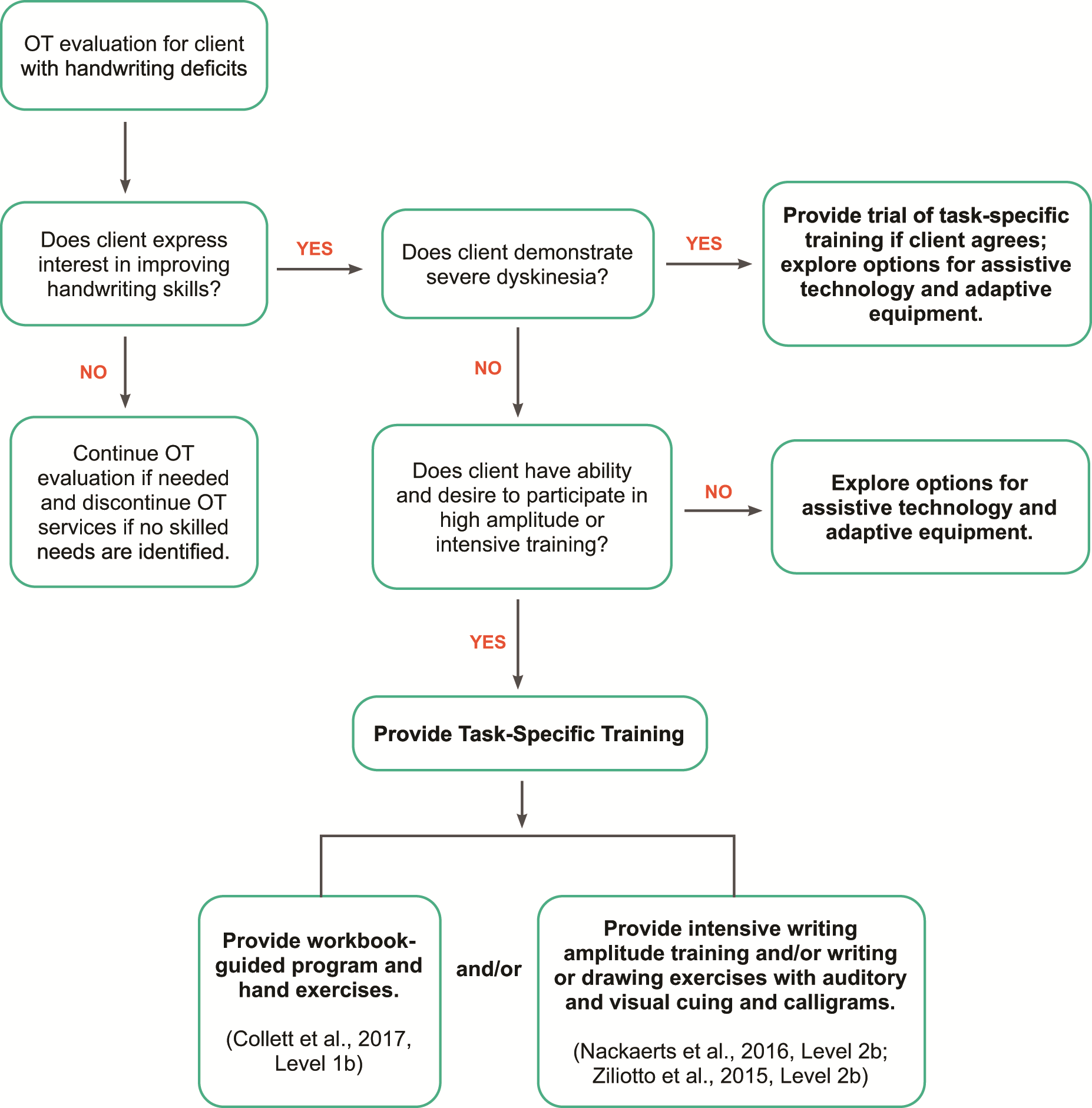
Decision-making algorithm for interventions to improve handwriting for people with Parkinson’s disease.
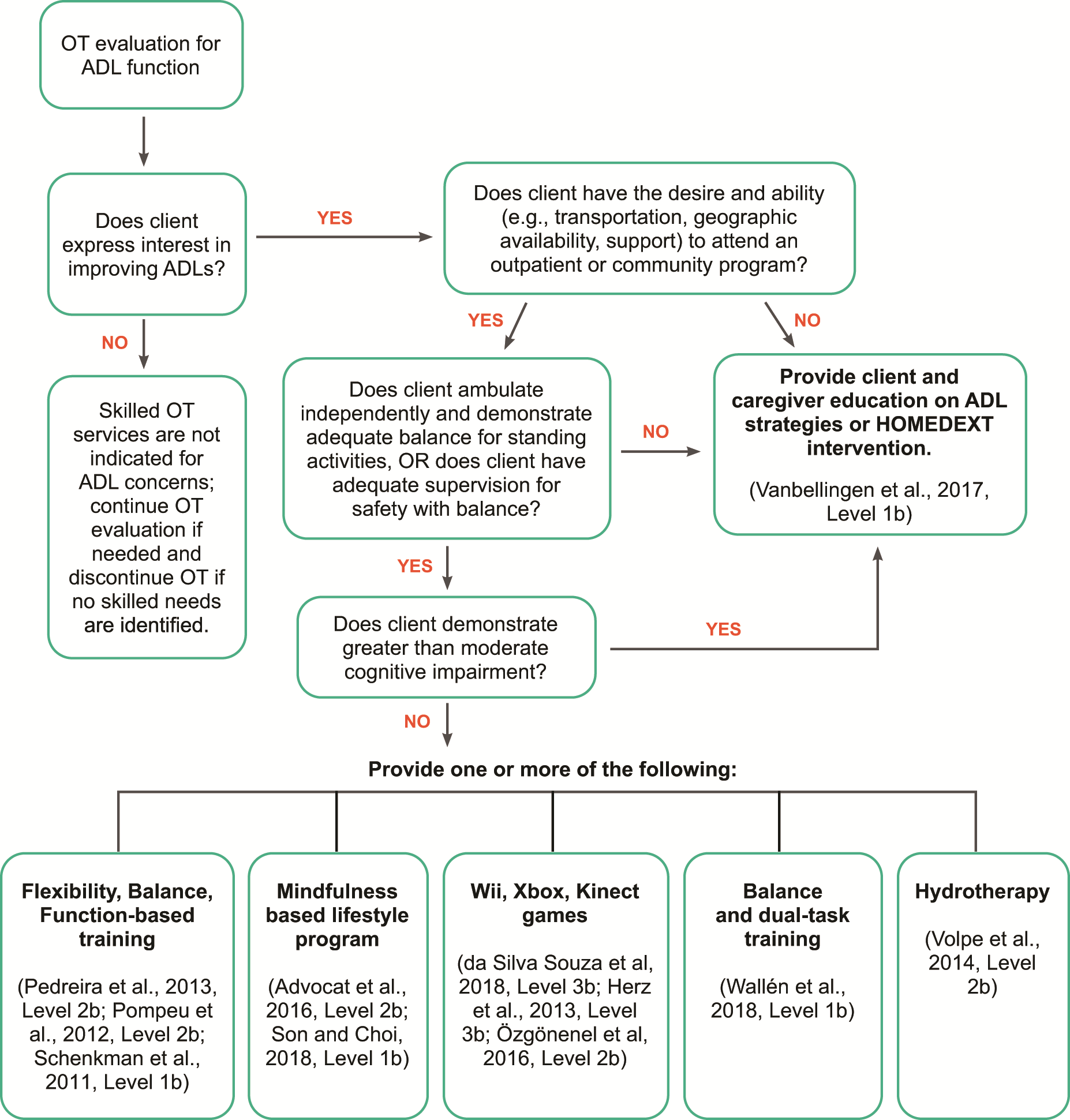
Decision-making algorithm for interventions to address ADLs for people with Parkinson’s disease.
Environmental Modifications, External Cues, and Functional Mobility Training
To increase Linda’s safety and prevent falls, the occupational therapist performed a home safety evaluation and recommended home modifications such as removing throw rugs, installing grab bars in the bathroom, and rearranging items in closets and cabinets to avoid bending and reaching (97535—Self-care/home management). The occupational therapist and occupational therapy assistant collaborated with the physical therapist to identify the best external cues and movement strategies to reduce Linda’s freezing of gait. Linda practiced using taped lines on the floor as an external cue to support walking through the kitchen doorway without freezing, and she was trained to use marching quarter turns and side stepping to address concerns with turning tasks in kitchen.
Outcomes
Linda met all of her goals for therapy. She demonstrated increased safety and independence in ADLs and IADLs and increased balance confidence, and she performed better than expected on goal attainment scaling for management of freezing of gait episodes during meal preparation activities. She demonstrated significant reduction in time for dressing tasks, reported no longer needing assistance for upper body dressing tasks, and made noticeable improvement in zipper manipulation, jewelry fastening, and handwriting. She demonstrated consistent tracking of her dopaminergic medications with accurate and timely compliance 7 days per week. Table 7 summarizes Linda’s outcomes.
Linda’s Discharge Assessment Results
Strengths and Limitations of the Current Body of Evidence
There are strengths and limitations related to the current body of evidence in the systematic reviews that informed this practice guideline. Systematic reviews address specific clinical questions that are guided by an a priori protocol for the question development and review process. No systematic review can address all aspects of a topic; authors make many decisions before conducting the review. Additionally, no review is perfect, and even the most careful searches sometimes miss articles. The way to reduce these potential sources of bias is to conduct the review using best-practice methodology.
Strengths
The review authors followed best-practice methodology to the best of their ability at every step of the process—for example, by getting input at all stages from practitioners, researchers, consumers, and experts in the areas included in the reviews. The review questions for the systematic reviews were developed with an intentional focus on occupation-based outcomes. Improvement in these outcomes is the goal of occupational therapy, so the systematic reviews targeted studies reporting occupation-based interventions and outcomes.
Limitations: Gaps in the Evidence
Gaps in knowledge exist when there is insufficient, imprecise, inconsistent, or biased information in the literature about an intervention (Robinson et al., 2011). Gaps also exist when the literature is not sufficient to answer a clinical question.
Lack of research supporting particular interventions does not mean practitioners should not use those interventions. In work with clients, practitioners considering specific interventions when there is not enough evidence to support evidence-based practice should use expert knowledge and their own training and experience to guide practice. In this section, we pinpoint important gaps in evidence for interventions and approaches practitioners may consider using as appropriate.
Occupational therapy practitioners need to think about the elements of evidence-based practice as they evaluate this guideline in light of gaps in the literature related to their clinical practice. Practitioners should consider the following questions when they identify these gaps (Gutenbrunner & Nugraha, 2020): What evidence exists? What are the best practices associated with providing services to this client population? What interventions are contraindicated for this population? What outcomes am I hoping to achieve with this client? Does evidence exist in another field or discipline related to interventions and desired outcomes that are within the scope of occupational therapy practice? What are my client’s preferences and values? Does my client prefer one intervention over another? Are available resources, cost, or time influencing my client’s preference? How might the intervention I am considering affect my client’s performance patterns and roles? Does my client find the intervention I am considering meaningful? What experience and expertise do I have that can help guide my decisions? What types of interventions have I used previously that were effective with similar clients or populations? What types of interventions have I used previously that were ineffective with similar clients or populations? What potential risks does the intervention I’m considering pose to my client or this client population? Will the health care system or organization be supportive of this intervention? How will I document this intervention? How will I document the outcomes associated with this intervention? Is it likely that this intervention will be reimbursed?
The following sections present additional information and common occupational therapy interventions for clients with PD that are not addressed in these guidelines because of a lack of relevant evidence. These sections are based on existing or emerging evidence, expert opinion, or both.
LSVT BIG
LSVT BIG is a popular task-oriented approach to improving movement in people with PD. Participants in LSVT BIG have shown improvements in balance, dexterity, posture, and gait speed (Flood et al., 2020; McDonnell et al., 2018). These motor-related improvements may translate into improved daily function for clients who are interested in the interventions and can tolerate the intensity. Occupational therapy practitioners may recommend additional activities or community programs (e.g., Rock Steady Boxing, n.d.) but should determine their appropriateness for clients and select the method of delivery (e.g., setting, training of professional, skills) to best fit their unique needs.
Nonmotor Impairments
Low vision
Occupational therapy practitioners should screen clients with PD for visual dysfunction and, if warranted, complete a formal evaluation to identify specific deficits. Interventions for low vision can include home safety modifications and strategies to support safe task performance (Savitt & Mathews, 2018).
Cognitive impairment
Occupational therapy practitioners should address cognition with clients with PD as it affects occupational performance and participation. They should assess cognition and provide treatment that matches the client’s cognitive abilities and functional goals. Goal-oriented and strategy-based cognitive interventions may help clients meet their personalized functional goals (e.g., Foster et al., 2018; Hindle et al., 2018; Reuter et al., 2012). In addition, cognitive stimulation therapy may be beneficial for people with PD-related dementia and their care partners (McCormick, McDonald, Vatter, Orgeta, Poliakoff, Smith, & Leroi, 2017; McCormick, McDonald, Vatter, Orgeta, Poliakoff, Smith, Silverdale, et al., 2017).
Occupations
Driving
Because participation in driving carries significant meaning and has an impact on safety, occupational therapy practitioners should screen clients with PD for fitness to drive. Practitioners should also consider the caregiver’s risk impressions (Classen & Alvarez, 2016) and the client’s scores on the Trail Making Test Part B (Arbuthnott & Frank, 2000), Useful Field of View (Edwards et al., 2006), and contrast sensitivity measures when screening to identify at-risk drivers with PD who need a comprehensive driving evaluation (Alvarez & Classen, 2018).
Work performance and employment
Occupational therapy practitioners should assess work-related skills and duties and provide strategies, modifications, and accommodations to support participation in work or productivity. Resources such as the Job Accommodation Network (n.d.) provide occupational therapy practitioners with useful ideas for job accommodations for people with PD.
Sexuality and intimacy
Intimacy and sexual expression are important dimensions of quality of life for people with PD and their partners. Occupational therapy practitioners should ensure a private and comfortable environment to discuss any changes to sexuality and can proactively address sexual health issues by providing information, recognizing and addressing the sexual needs of people with PD, and referring them to specialists (Bronner, 2009).
Care Partner–Oriented Intervention
Care partners are an integral part of the team when providing client-centered care to people with PD, and they often experience significant challenges (e.g., financial, social, work-related, psychological) as they navigate this complex role. Occupational therapy practitioners can support the participatory roles of care partners of people with PD by providing education on home modifications, task adaptations, cuing strategies, handling, equipment use, and fall prevention. They should also directly address the care partner’s well-being by discussing topics such as stress management, engagement in physical activity, communication, social support, respite care, and occupational balance (e.g., yoga [Walter et al., 2018], cognitive–behavioral therapy [Okai et al., 2013]).
Additional Implications for Occupational Therapy
To complement the intervention recommendations provided in Tables 1–3, the sections that follow describe general implications for occupational therapy with people with PD and their care partners based on PD-related evidence and best-practice occupational therapy principles.
Specialized Multidisciplinary Care
The clinical recommendations regarding multidisciplinary inpatient rehabilitation to improve ADL performance are based on the findings of studies conducted in Italy. Although this model of care is not (yet) standard practice in the United States, a consensus of expert opinion is that occupational therapy with people with PD should occur in the context of specialized multidisciplinary care across the continuum of settings and stages. In all settings and countries, occupational therapy practitioners should use their professional reasoning and experiences to determine whether findings on specialized multidisciplinary care interventions can be generalized to the specific individual, family, and context with which they are working.
Client-Centered Goal-Oriented Treatment
Occupational therapy places value on the delivery of client-centered goal-oriented care, and evidence supports the effectiveness of this approach for people with PD (e.g., Cabrera-Martos et al., 2019; Hindle et al., 2018; Sturkenboom et al., 2014). To develop and track personally meaningful functional goals and measure their achievement, occupational therapy practitioners should use comprehensive and standardized tools such as the Canadian Occupational Performance Measure (Law et al., 2014), goal attainment scaling, the Bangor Goal-Setting Interview (Clare et al., 2016), and the Patient-Specific Functional Scale (Stratford et al., 1995).
Occupation-Based Performance Assessment
Assessment of occupation-based outcomes in research on interventions for people with PD continues to be limited. In addition to using self-report measures of function, occupational therapy practitioners should use objective, performance-based measures of occupational performance and participation to further support the profession’s role with this population. Such measures include the Assessment of Motor and Process Skills (Fisher, 2006), the Performance Assessment of Self-Care Skills (Holm & Rogers, 2008), the Executive Function Performance Test (Baum et al., 2016), the Weekly Calendar Planning Activity (Toglia, 2015), and the Continuous Scale Physical Function Test (Cress et al., 1996).
Late-Stage Parkinson’s Disease
A majority of occupational therapy–related intervention research does not include participants in the late or more severe stages of PD (i.e., Hoehn and Yahr Stages 4 and 5 dementia). Occupational therapy practitioners are often involved in the care of such individuals and offer valuable services, such as maintaining safety of clients and care partners; maximizing comfort; providing opportunities for meaningful occupational engagement; providing caregiver training; planning for posture, positioning, and pressure care; and assisting in end-of-life planning (Aragon & Kings, 2018).
Summary
This Practice Guideline highlights occupational therapy’s unique contribution to the clinical care of people with PD and their care partners. Clinical recommendations based on the current evidence are provided, and application to clinical practice has been exemplified through case studies and decision-making algorithms. Gaps in the evidence on interventions for this population have been highlighted; occupational therapy practitioners should consider these gaps when treating people with PD and their care partners, and researchers should further investigate these gaps to advance the care of people with PD.
Occupational therapy has a distinct and valuable role in supporting the participation, health, and well-being of people with PD and their care partners. In selecting dynamic interventions, occupational therapy practitioners consider a complex and unique set of factors that influence occupational performance. Practitioners can use this Practice Guideline to integrate their own professional experience and reasoning, their clients’ individual and family preferences, and the best available research evidence to provide the highest quality of care for people with PD and their care partners. As the profession and care of people with PD continue to evolve, occupational therapy will need to remain innovative in service delivery models, increase educational opportunities to best prepare future practitioners, and advance the research evidence to provide best-practice services grounded in evidence, theory, and occupation.
Footnotes
1
Codes shown refer to CPT 2022 (American Medical Association, 2021, CPT 2022 Professional Edition, Chicago: American Medical Association Press) and do not represent all of the possible codes that may be used in occupational therapy evaluation and intervention. After 2022, refer to the current year’s CPT code book for available codes. CPT codes are updated annually and become effective January 1. CPT is a trademark of the American Medical Association. CPT five-digit codes, two-digit codes, modifiers, and descriptions are copyright © 2022 by the American Medical Association. All rights reserved.
*
Indicates articles included in the systematic reviews.
Acknowledgments
The authors acknowledge and thank the following individuals for their participation in the content review and development of this publication:
Hillary Richardson, MOT, OTR/L, AOTA Practice Manager, Knowledge Translation, Evidence-Based Practice and Practice Improvement, for her contributions related to knowledge translation and algorithm development.
Deborah Lieberman, MHSA, OTR/L, FAOTA, Vice President, Practice Improvement, and Staff Liaison to the Commission on Practice, American Occupational Therapy Association, North Bethesda, MD
Susan Cahill, PhD, OTR/L, FAOTA, Director of Evidence-Based Practice, American Occupational Therapy Association, North Bethesda, MD
Elizabeth G. Hunter, PhD, OTR/L, Assistant Professor, Graduate Center for Gerontology, College of Public Health, University of Kentucky, Lexington
Jamie Archer, MOT, OTR/L; Lisa Carson, OTD, OTR/L; Heather J. Cianci, PT, MS, GCS; Barbara M. Doucet, PhD, LOTR; Joellyn Fox, DPT; Ingrid Franc, PhD, LOTR; Darla Freeman, SLPD, CCC-SLP; Jennifer Goldman, MD, MS; Bernadette Kosir, OTR/L; Kelli Reiling Ott, OTD, OTR/L, MSCS; Chuck Willmarth, CAE; Lance Wilson, MSS, LSW, C-SWHC, ASW-G
The authors acknowledge the following individuals for their contributions to the evidence-based systematic review: Jamie Archer, MOT, OTR/L; Anna E. Boone, MSOT, PhD, OTR/L; Lisa Carson, OTD, OTR/L; Barbara M. Doucet, PhD, LOTR; Erin Foster, PhD, OTD, OTR/L; Ingrid Franc, PhD, LOTR; Whitney Henderson, MOT, OTR/L, OTD; Elizabeth G. Hunter, PhD, OTR/L; Sherry Kolodziejczak, MS, OTR/L, FEW, PAMC, cNDT; Kelli Reiling Ott, OTD, OTR/L, MSCS.
Appendix: Overview of the Systematic Review Methods and Findings
The systematic reviews completed for this Practice Guideline were conducted according to the Cochrane Collaboration methodology (Higgins et al., 2019) and are reported consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009).